Fungal Skin Infections on October 1, 2021 by Guest
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Systematic Review of Diagnosis and Treatment Options for Tinea Imbricata
Int. J. Life Sci. Pharma Res. 2019 Oct; 9(4): (L) 28-33 ISSN 2250-0480 Review Article Dermatology International Journal of Life science and Pharma Research A SYSTEMATIC REVIEW OF DIAGNOSIS AND TREATMENT OPTIONS FOR TINEA IMBRICATA RANA ABDULAZEEM AL-BASSAM1, BASMAH SALEM AL AFARI 1 AND MANAL HASSAN MOHAMED SALEM2* 1Intern doctor, Dar Al Uloom University Riyadh, Saudi Arabia., 2Mater degree of dermatology,venereology and andrology , Doctor Abdulazeem Albassam Medical Group, Department of Dermatology, Riyadh, Saudi Arabia ABSTRACT Tinea imbricata is a cutaneous fungal disease and sometimes called (Tokelau). The causative agent is a dermatophyte known as Trichophyton concentricum. It is an endemic in developing countries particularly in South Pacific, India, Central and South America, as well as Mexico. It is generally observed in people with poor living conditions and poor personal hygiene. Predisposing factors are hot weather, humidity, and host immunity in addition to genetic factors. The patients usually presented with concentric or lamellar skin lesions. The aim of this review is to highlight important information about microbial, clinical and therapeutic aspects of tinea imbricta. In this review, we search the literature to identify articles talking different aspects of tinea imbricta. The electronic search was performed in four databases to identify eligible articles in the literature. Electronic databases were searched including MEDLINE and EMBASE using PubMed search engine. In addition, Cochrane library and ovid was searched. The titles and abstracts of the resulted articles were screened to identify eligible studies. Based on the primary screening results the irrelevant studies, duplicated and reviews were excluded. Tinea imbricta is found to be endemic in 3 main geographical regions, Southwest Pacific, Southeast Asia, and Central and South America. -

Introduction to Mycology
INTRODUCTION TO MYCOLOGY The term "mycology" is derived from Greek word "mykes" meaning mushroom. Therefore mycology is the study of fungi. The ability of fungi to invade plant and animal tissue was observed in early 19th century but the first documented animal infection by any fungus was made by Bassi, who in 1835 studied the muscardine disease of silkworm and proved the that the infection was caused by a fungus Beauveria bassiana. In 1910 Raymond Sabouraud published his book Les Teignes, which was a comprehensive study of dermatophytic fungi. He is also regarded as father of medical mycology. Importance of fungi: Fungi inhabit almost every niche in the environment and humans are exposed to these organisms in various fields of life. Beneficial Effects of Fungi: 1. Decomposition - nutrient and carbon recycling. 2. Biosynthetic factories. The fermentation property is used for the industrial production of alcohols, fats, citric, oxalic and gluconic acids. 3. Important sources of antibiotics, such as Penicillin. 4. Model organisms for biochemical and genetic studies. Eg: Neurospora crassa 5. Saccharomyces cerviciae is extensively used in recombinant DNA technology, which includes the Hepatitis B Vaccine. 6. Some fungi are edible (mushrooms). 7. Yeasts provide nutritional supplements such as vitamins and cofactors. 8. Penicillium is used to flavour Roquefort and Camembert cheeses. 9. Ergot produced by Claviceps purpurea contains medically important alkaloids that help in inducing uterine contractions, controlling bleeding and treating migraine. 10. Fungi (Leptolegnia caudate and Aphanomyces laevis) are used to trap mosquito larvae in paddy fields and thus help in malaria control. Harmful Effects of Fungi: 1. -

Use of Propolis for Topical Treatment of Dermatophytosis in Dog
Open Journal of Veterinary Medicine, 2014, 4, 239-245 Published Online October 2014 in SciRes. http://www.scirp.org/journal/ojvm http://dx.doi.org/10.4236/ojvm.2014.410028 Use of Propolis for Topical Treatment of Dermatophytosis in Dog Tonatiuh Alejandro Cruz Sánchez1, Perla Alejandra Estrada García1, Cristian Ismael López Zamora1, Marcela Autran Martínez2, Víctor Pérez Valencia2, Amparo Londoño Orozco1 1Facultad de Estudios Superiores Cuautitlán, Universidad Nacional Autónoma de México, Cuautitlán Izcalli, México 2Belén Veterinary Hospital, Tultitlan, México Email: [email protected] Received 12 July 2014; revised 10 August 2014; accepted 16 September 2014 Copyright © 2014 by authors and Scientific Research Publishing Inc. This work is licensed under the Creative Commons Attribution International License (CC BY). http://creativecommons.org/licenses/by/4.0/ Abstract Here we present three clinical cases of canine dermatophytosis resolved with topical propolis treatment that involved alopecia and well-demarcated erythematous lesions. These cases were positively identified by direct observation of samples from the affected zones with 10% KOH. Each sample was cultured, leading to the isolation of Microsporum gypseum in one case and Microspo- rum canis in the other two cases. The animals’ subsequent treatment included bathing using a commercial soap with propolis every seven days for 3 to 8 weeks, as well as the use of a propolis- containing ointment elaborated in our laboratory, which was applied to the lesions once a day for three weeks. From the second week of treatment, all cultures were negative. At the end of treat- ment, all cases displayed full recovery of the injuries and hair growth in these areas. -

The Burden of Serious Fungal Diseases in Russia
mycoses Diagnosis,Therapy and Prophylaxis of Fungal Diseases Supplement article The burden of serious fungal diseases in Russia N. Klimko,1 Y. Kozlova,1 S. Khostelidi,1 O. Shadrivova,1 Y. Borzova,1 E. Burygina,1 N. Vasilieva1 and D. W. Denning2 1I. Metchnikov North-Western State Medical University, St. Petersburg, Russia and 2Manchester Academic Health Science Centre, The National Aspergillosis Centre, University Hospital of South Manchester, The University of Manchester, Manchester, UK Summary The incidence and prevalence of fungal infections in Russia is unknown. We estimated the burden of fungal infections in Russia according to the methodol- ogy of the LIFE program (www.LIFE-worldwide.org). The total number of patients with serious and chronic mycoses in Russia in 2011 was three million. Most of these patients (2607 494) had superficial fungal infections (recurrent vulvovaginal candidiasis, oral and oesophageal candidiasis with HIV infection and tinea capitis). Invasive and chronic fungal infections (invasive candidiasis, invasive and chronic aspergillosis, cryptococcal meningitis, mucormycosis and Pneumocystis pneumonia) affected 69 331 patients. The total number of adults with allergic bronchopulmonary aspergillosis and severe asthma with fungal sensitisation was 406 082. Key words: aspergillosis, candidiasis, cryptococcal meningitis, fungal infections, mucormycosis, Russia. obstructive pulmonary disease (COPD) or liver failure, Introduction to name some examples. Over the past decades fungal diseases have become a The incidence and prevalence of fungal infections in serious clinical problem. Worldwide mortality from Russia is unknown. The aim of this research is to esti- fungal infections is comparable to mortality from mate the burden of serious and chronic fungal diseases tuberculosis or malaria and is thought to exceed in Russia. -

Fungal Infections (Mycoses): Dermatophytoses (Tinea, Ringworm)
Editorial | Journal of Gandaki Medical College-Nepal Fungal Infections (Mycoses): Dermatophytoses (Tinea, Ringworm) Reddy KR Professor & Head Microbiology Department Gandaki Medical College & Teaching Hospital, Pokhara, Nepal Medical Mycology, a study of fungal epidemiology, ecology, pathogenesis, diagnosis, prevention and treatment in human beings, is a newly recognized discipline of biomedical sciences, advancing rapidly. Earlier, the fungi were believed to be mere contaminants, commensals or nonpathogenic agents but now these are commonly recognized as medically relevant organisms causing potentially fatal diseases. The discipline of medical mycology attained recognition as an independent medical speciality in the world sciences in 1910 when French dermatologist Journal of Raymond Jacques Adrien Sabouraud (1864 - 1936) published his seminal treatise Les Teignes. This monumental work was a comprehensive account of most of then GANDAKI known dermatophytes, which is still being referred by the mycologists. Thus he MEDICAL referred as the “Father of Medical Mycology”. COLLEGE- has laid down the foundation of the field of Medical Mycology. He has been aptly There are significant developments in treatment modalities of fungal infections NEPAL antifungal agent available. Nystatin was discovered in 1951 and subsequently and we have achieved new prospects. However, till 1950s there was no specific (J-GMC-N) amphotericin B was introduced in 1957 and was sanctioned for treatment of human beings. In the 1970s, the field was dominated by the azole derivatives. J-GMC-N | Volume 10 | Issue 01 developed to treat fungal infections. By the end of the 20th century, the fungi have Now this is the most active field of interest, where potential drugs are being January-June 2017 been reported to be developing drug resistance, especially among yeasts. -

Failure of Treatment in Chronic Dermatophyte Infections R
Postgraduate Medical Journal (September 1979) 55, 608-610 Failure of treatment in chronic dermatophyte infections R. J. HAY M.R.C.P. Department ofMicrobiology, London School of Hygiene and Tropical Medicine, London WC1E 7HT Summary (Roth, Sallman and Blank, 1959). It seems, there- A proportion of dermatophyte infections fail to fore, that the effectiveness of griseofulvin is depen- respond to normally adequate courses of griseofulvin dent on host factors such as the immune response and tropical antifungal therapy. The organism Tricho- and a normal turnover of epidermis which tends to phyton rubrum was isolated from 96°o of 50 patients shed the organism into the environment. studied, but no instances of in vitro resistance were Griseofulvin remains a useful drug, surprisingly seen. Of these patients, 57%o had an underlying free of side effects in the doses normally used condition, commonly hay fever/asthma, atopic eczema, (Livingood et al., 1960). Gastric intolerance, head- collagen disease or ichthyosis. Defective delayed type aches, urticaria and rashes, and leucopenia have hypersensitivity responses and leucocyte migration been described. inhibition to the specific antigen, trichophytin, were The patients described here had chronic dermato- demonstrated. Immediate type hypersensitivity was phyte infections, often of many years' standing. The seen in 58% and this was partially suppressible with clinical presentation was remarkably constant and chlorpheniramine and cimetidine. The relationship the very rare variants, dermatophyte mycetoma -

The New Species Concept in Dermatophytes—A Polyphasic Approach
Mycopathologia DOI 10.1007/s11046-008-9099-y The New Species Concept in Dermatophytes—a Polyphasic Approach Yvonne Gra¨ser Æ James Scott Æ Richard Summerbell Received: 15 October 2007 / Accepted: 30 January 2008 Ó Springer Science+Business Media B.V. 2008 Abstract The dermatophytes are among the most among these are the cosmopolitan bane of nails and frequently observed organisms in biomedicine, yet feet, Trichophyton rubrum, and the endemic African there has never been stability in the taxonomy, agent of childhood tinea capitis, Trichophyton identification and naming of the approximately 25 soudanense, which are effectively inseparable in all pathogenic species involved. Since the identification analyses. The molecular data require some reinter- of these species is often epidemiologically and pretation of results seen in conventional phenotypic ethically important, the difficulties in dermatophyte tests, but in most cases, phylogenetic insight is identification are a fruitful topic for modern molec- readily integrated with current laboratory testing ular biological investigation, done in tandem with procedures. renewed investigation of phenotypic characters. Molecular phylogenetic analyses such as multilocus Keywords Dermatophytes Á Taxonomy Á sequence typing have had to be tailored to accom- Molecular identification Á modate differing the mechanisms of speciation that Morphological identification Á Species concept have produced the dermatophytes that are commonly seen today. Even so, some biotypes that were unambiguously considered species in the past, based Introduction: Why Dermatophyte Biosystematics on profound differences in morphology and pattern of and Identification are Important (Medical infection, appear consistently not to be distinct and Scientific Aspects) species in modern molecular analyses. Most notable The dermatophytes belong to the small category of disease organisms that almost every human alive will Y. -

How Much Human Ringworm Is Zoophilic? Mcphee A, Cherian S, Robson J Adapted from Poster Produced for the Zoonoses Conference 25–26 July 2014 Brisbane
How much human ringworm is zoophilic? McPhee A, Cherian S, Robson J Adapted from poster produced for the Zoonoses Conference 25–26 July 2014 Brisbane Introduction Epidermophyton floccosum Humans Common Dermatophytes can be the cause of common infections in both Trichophyton rubrum [worldwide] Humans Very common humans and animals. The source of human infection may be Trichophyton rubrum [African] Humans Less common anthropophilic (human), geophilic (soil) or zoophilic (animal). Trichophyton interdigitale Anthropophilic Humans Common Zoophilic dermatophyte infections usually elicit a strong host [anthropophilic] response on the skin where there is contact with the infective Trichophyton tonsurans Humans Common animal or contaminated fomites. Table 1 illustrates the range of Trichophyton violaceum Humans Less common dermatophytes that are isolated from the mycology laboratory Microsporum audouinii Humans Less common and grouped by source of acquisition. Microsporum gypseum Soil Common Geophilic Microsporum nanum Soil/Pigs Rare Guinea pigs, Aim Trichophyton interdigitale [zoophilic] Common kangaroos To characterize and compare zoophilic with non-zoophilic Microsporum canis Cats Common dermatophyte human infections isolated at Sullivan Nicolaides Zoophilic Trichophyton verrucosum Cattle Rare Pathology (SNP) for the year 2013. Trichophyton equinum Horses Rare Microsporum nanum Soil/pigs Rare Method Table 1: Classification of dermatophytes according to source Superficial fungal cultures submitted in 2013 to Sullivan Nicolaides Pathology were reviewed. This laboratory services Queensland and extends into New South Wales as far south as Coffs Harbour. Specimens include skin scrapings, skin biopsies, nails and involved hair. All cutaneous samples (Figure 1) submitted for fungal culture receive direct examination using Calcofluor white/Evans Blue/ KOH/Glycerol under fluorescent and/or light microscopy (Figure 2) and cultured. -
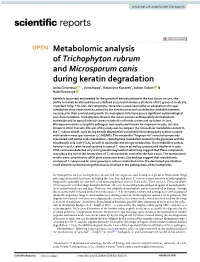
Metabolomic Analysis of Trichophyton Rubrum and Microsporum Canis
www.nature.com/scientificreports OPEN Metabolomic analysis of Trichophyton rubrum and Microsporum canis during keratin degradation Anita Ciesielska 1*, Anna Kawa1, Katarzyna Kanarek1, Adrian Soboń 1 & Rafał Szewczyk 2 Keratin is important and needed for the growth of dermatophytes in the host tissue. In turn, the ability to invade keratinised tissues is defned as a pivotal virulence attribute of this group of medically important fungi. The host–dermatophyte interaction is accompanied by an adaptation of fungal metabolism that allows them to adhere to the host tissue as well as utilize the available nutrients necessary for their survival and growth. Dermatophyte infections pose a signifcant epidemiological and clinical problem. Trichophyton rubrum is the most common anthropophilic dermatophyte worldwide and its typical infection areas include skin of hands or feet and nail plate. In turn, Microsporum canis is a zoophilic pathogen, and mostly well known for ringworm in pets, it is also known to infect humans. The aim of the study was to compare the intracellular metabolite content in the T. rubrum and M. canis during keratin degradation using liquid chromatography system coupled with tandem mass spectrometer (LC-MS/MS). The metabolite “fngerprints” revealed compounds associated with amino acids metabolism, carbohydrate metabolism related to the glycolysis and the tricarboxylic acid cycle (TCA), as well as nucleotide and energy metabolism. The metabolites such as kynurenic acid, l-alanine and cysteine in case of T. rubrum as well as cysteine and ribofavin in case of M. canis were detected only during keratin degradation what may suggest that these compounds may play a key role in the interactions of T. -
Mycology Proficiency Testing Program
Mycology Proficiency Testing Program Test Event Critique January 2013 Mycology Laboratory Table of Contents Mycology Laboratory 2 Mycology Proficiency Testing Program 3 Test Specimens & Grading Policy 5 Test Analyte Master Lists 7 Performance Summary 11 Commercial Device Usage Statistics 15 Mold Descriptions 16 M-1 Exserohilum species 16 M-2 Phialophora species 20 M-3 Chrysosporium species 25 M-4 Fusarium species 30 M-5 Rhizopus species 34 Yeast Descriptions 38 Y-1 Rhodotorula mucilaginosa 38 Y-2 Trichosporon asahii 41 Y-3 Candida glabrata 44 Y-4 Candida albicans 47 Y-5 Geotrichum candidum 50 Direct Detection - Cryptococcal Antigen 53 Antifungal Susceptibility Testing - Yeast 55 Antifungal Susceptibility Testing - Mold (Educational) 60 1 Mycology Laboratory Mycology Laboratory at the Wadsworth Center, New York State Department of Health (NYSDOH) is a reference diagnostic laboratory for the fungal diseases. The laboratory services include testing for the dimorphic pathogenic fungi, unusual molds and yeasts pathogens, antifungal susceptibility testing including tests with research protocols, molecular tests including rapid identification and strain typing, outbreak and pseudo-outbreak investigations, laboratory contamination and accident investigations and related environmental surveys. The Fungal Culture Collection of the Mycology Laboratory is an important resource for high quality cultures used in the proficiency-testing program and for the in-house development and standardization of new diagnostic tests. Mycology Proficiency Testing Program provides technical expertise to NYSDOH Clinical Laboratory Evaluation Program (CLEP). The program is responsible for conducting the Clinical Laboratory Improvement Amendments (CLIA)-compliant Proficiency Testing (Mycology) for clinical laboratories in New York State. All analytes for these test events are prepared and standardized internally. -

The Role of Dendritic Cells in the Innate Recognition of Pathogenic Fungi (A. Fumigatus, C. Neoformans and C. Albicans)
SPECIAL FOCUS REVIEW: DENDRITIC CELLS Virulence 3:7, 635–646; November 15, 2012; G 2012 Landes Bioscience The role of dendritic cells in the innate recognition of pathogenic fungi (A. fumigatus, C. neoformans and C. albicans) Zaida G. Ramirez-Ortiz and Terry K. Means* Center for Immunology and Inflammatory Diseases and Division of Rheumatology, Allergy, and Immunology; Massachusetts General Hospital and Harvard Medical School; Charlestown, MA USA Keywords: plasmacytoid dendritic cells, conventional dendritic cells, fungi, Toll-like receptors, scavenger receptors Dendritic cells (DCs) are the bridge between the innate and The Big Three: Aspergillus fumigatus, Candida adaptive immune system. DCs are responsible for sensing and albicans and Cryptococcus neoformans patrolling the environment, initiating a host response and instructing the proper adaptive immune response against Increase in the incidence of fungal infections correlates with pathogens. Recent advances in medical treatments have led to increased use of immunosuppressive drugs, leading to the advances in medical treatment resulting in increased numbers of emergence of fungal species that cause life-threatening immune-compromised patients, particularly those suffering from infections in humans. Three of these opportunistic fungal AIDS, cancer patients receiving chemotherapy and those taking pathogens: Aspergillus fumigatus, Candida albicans and immunosuppressive drugs following solid organ transplantation.3 Cryptococcus neoformans pose the biggest concern for the Aspergillus fumigatus is the primary causative species of human immune-compromised host. Here we will review the interac- aspergillosis. On a daily basis, humans inhale hundreds of tions between DCs and these fungal pathogens, the receptors microscopic conidia or non-motile spores of this mold. These 2–3 expressed on DCs that mediate these responses and the mm conidia are small enough to bypass the mucosal barriers and signaling mechanisms that shape the adaptive host response. -

Mycologic Disorders of the Skin Catherine A
Mycologic Disorders of the Skin Catherine A. Outerbridge, DVM, MVSc, DACVIM, DACVD Cutaneous tissue can become infected when fungal organisms contaminate or colonize the epidermal surface or hair follicles. The skin can be a portal of entry for fungal infection when the epithelial barrier is breached or it can be a site for disseminated, systemic fungal disease. The two most common cutaneous fungal infections in small animals are dermato- phytosis and Malassezia dermatitis. Dermatophytosis is a superficial cutaneous infection with one or more of the fungal species in the keratinophilic genera Microsporum, Tricho- phyton,orEpidermophyton. Malassezia pachydermatis is a nonlipid dependent fungal species that is a normal commensal inhabitant of the skin and external ear canal in dogs and cats. Malassezia pachydermatis is the most common cause of Malassezia dermatitis. The diagnosis and treatment of these cutaneous fungal infections will be discussed. Clin Tech Small Anim Pract 21:128-134 © 2006 Elsevier Inc. All rights reserved. KEYWORDS dermatophytosis, Malassezia dermatitis, dogs, cats, Microsporum, Trichophyton, Malassezia pachydermatis ver 300 species of fungi have been reported toDermatophytosis be animal O pathogens.1 Cutaneous tissue can become infected when fungal organisms contaminate or colonize the epider- Etiology mal surface or hair follicles. The skin can be a portal of entry Dermatophytosis is a superficial cutaneous infection with for fungal infection when the epithelial barrier is breached or one or more of the fungal species in the keratinophilic genera it can be a site for disseminated, systemic fungal disease. Microsporum, Trichophyton,orEpidermophyton. Dermato- Canine and feline skin and hair coats can be transiently con- phyte genera that infect animals are divided into 3 or 4 taminated with a large variety of saprophytic fungi from the groups based on their natural habitat.