14Q11.2 Deletions FTNP
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Topological Scoring of Protein Interaction Networks
bioRxiv preprint doi: https://doi.org/10.1101/438408; this version posted October 8, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Topological Scoring of Protein Interaction Networks Mihaela E. Sardiu1, Joshua M. Gilmore1,2, Brad D. Groppe1,3, Arnob Dutta1,4, Laurence Florens1, and Michael P. Washburn1,5‡ 1Stowers Institute for Medical Research, Kansas City, MO 64110 U.S.A. 2Current Address: Boehringer Ingelheim Vetmedica, St. Joseph, MO 64506 U.S.A. 3Current Address: Thermo Fisher Scientific, Waltham, MA 02451, U.S.A. 4Current Address: Department of Cell and Molecular Biology, University of Rhode Island, 287 CBLS, 120 Flagg Road, Kingston, RI 02881. 5 Department of Pathology and Laboratory Medicine, The University of Kansas Medical Center, 3901 Rainbow Boulevard, Kansas City, Kansas 66160, USA ‡To whom correspondence should be addressed: Michael Washburn, Ph.D. Stowers Institute for Medical Research 1000 E. 50th St. Kansas City, MO 64110 Phone: 816-926-4457 E-mail: [email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/438408; this version posted October 8, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Abstract It remains a significant challenge to define individual protein associations within networks where an individual protein can directly interact with other proteins and/or be part of large complexes, which contain functional modules. Here we demonstrate the topological scoring (TopS) algorithm for the analysis of quantitative proteomic analyses of affinity purifications. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Supplementary Materials
Supplementary materials Supplementary Table S1: MGNC compound library Ingredien Molecule Caco- Mol ID MW AlogP OB (%) BBB DL FASA- HL t Name Name 2 shengdi MOL012254 campesterol 400.8 7.63 37.58 1.34 0.98 0.7 0.21 20.2 shengdi MOL000519 coniferin 314.4 3.16 31.11 0.42 -0.2 0.3 0.27 74.6 beta- shengdi MOL000359 414.8 8.08 36.91 1.32 0.99 0.8 0.23 20.2 sitosterol pachymic shengdi MOL000289 528.9 6.54 33.63 0.1 -0.6 0.8 0 9.27 acid Poricoic acid shengdi MOL000291 484.7 5.64 30.52 -0.08 -0.9 0.8 0 8.67 B Chrysanthem shengdi MOL004492 585 8.24 38.72 0.51 -1 0.6 0.3 17.5 axanthin 20- shengdi MOL011455 Hexadecano 418.6 1.91 32.7 -0.24 -0.4 0.7 0.29 104 ylingenol huanglian MOL001454 berberine 336.4 3.45 36.86 1.24 0.57 0.8 0.19 6.57 huanglian MOL013352 Obacunone 454.6 2.68 43.29 0.01 -0.4 0.8 0.31 -13 huanglian MOL002894 berberrubine 322.4 3.2 35.74 1.07 0.17 0.7 0.24 6.46 huanglian MOL002897 epiberberine 336.4 3.45 43.09 1.17 0.4 0.8 0.19 6.1 huanglian MOL002903 (R)-Canadine 339.4 3.4 55.37 1.04 0.57 0.8 0.2 6.41 huanglian MOL002904 Berlambine 351.4 2.49 36.68 0.97 0.17 0.8 0.28 7.33 Corchorosid huanglian MOL002907 404.6 1.34 105 -0.91 -1.3 0.8 0.29 6.68 e A_qt Magnogrand huanglian MOL000622 266.4 1.18 63.71 0.02 -0.2 0.2 0.3 3.17 iolide huanglian MOL000762 Palmidin A 510.5 4.52 35.36 -0.38 -1.5 0.7 0.39 33.2 huanglian MOL000785 palmatine 352.4 3.65 64.6 1.33 0.37 0.7 0.13 2.25 huanglian MOL000098 quercetin 302.3 1.5 46.43 0.05 -0.8 0.3 0.38 14.4 huanglian MOL001458 coptisine 320.3 3.25 30.67 1.21 0.32 0.9 0.26 9.33 huanglian MOL002668 Worenine -

Methods for Using Small Non-Coding Rnas to Improve Recombinant Protein Expression in Mammalian Cells
G C A T T A C G G C A T genes Review Methods for Using Small Non-Coding RNAs to Improve Recombinant Protein Expression in Mammalian Cells Sarah Inwood 1,2 ID , Michael J. Betenbaugh 2 and Joseph Shiloach 1,* 1 Biotechnology Core Laboratory, NIDDK, NIH, Bethesda, MD 20892, USA; [email protected] 2 Department of Chemical and Biomolecular Engineering, Johns Hopkins University, Baltimore, MD 21218, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-301-496-9719 Received: 17 November 2017; Accepted: 3 January 2018; Published: 9 January 2018 Abstract: The ability to produce recombinant proteins by utilizing different “cell factories” revolutionized the biotherapeutic and pharmaceutical industry. Chinese hamster ovary (CHO) cells are the dominant industrial producer, especially for antibodies. Human embryonic kidney cells (HEK), while not being as widely used as CHO cells, are used where CHO cells are unable to meet the needs for expression, such as growth factors. Therefore, improving recombinant protein expression from mammalian cells is a priority, and continuing effort is being devoted to this topic. Non-coding RNAs are RNA segments that are not translated into a protein and often have a regulatory role. Since their discovery, major progress has been made towards understanding their functions. Non-coding RNA has been investigated extensively in relation to disease, especially cancer, and recently they have also been used as a method for engineering cells to improve their protein expression capability. In this review, we provide information about methods used to identify non-coding RNAs with the potential of improving recombinant protein expression in mammalian cell lines. -

Nuclear PTEN Safeguards Pre-Mrna Splicing to Link Golgi Apparatus for Its Tumor Suppressive Role
ARTICLE DOI: 10.1038/s41467-018-04760-1 OPEN Nuclear PTEN safeguards pre-mRNA splicing to link Golgi apparatus for its tumor suppressive role Shao-Ming Shen1, Yan Ji2, Cheng Zhang1, Shuang-Shu Dong2, Shuo Yang1, Zhong Xiong1, Meng-Kai Ge1, Yun Yu1, Li Xia1, Meng Guo1, Jin-Ke Cheng3, Jun-Ling Liu1,3, Jian-Xiu Yu1,3 & Guo-Qiang Chen1 Dysregulation of pre-mRNA alternative splicing (AS) is closely associated with cancers. However, the relationships between the AS and classic oncogenes/tumor suppressors are 1234567890():,; largely unknown. Here we show that the deletion of tumor suppressor PTEN alters pre-mRNA splicing in a phosphatase-independent manner, and identify 262 PTEN-regulated AS events in 293T cells by RNA sequencing, which are associated with significant worse outcome of cancer patients. Based on these findings, we report that nuclear PTEN interacts with the splicing machinery, spliceosome, to regulate its assembly and pre-mRNA splicing. We also identify a new exon 2b in GOLGA2 transcript and the exon exclusion contributes to PTEN knockdown-induced tumorigenesis by promoting dramatic Golgi extension and secretion, and PTEN depletion significantly sensitizes cancer cells to secretion inhibitors brefeldin A and golgicide A. Our results suggest that Golgi secretion inhibitors alone or in combination with PI3K/Akt kinase inhibitors may be therapeutically useful for PTEN-deficient cancers. 1 Department of Pathophysiology, Key Laboratory of Cell Differentiation and Apoptosis of Chinese Ministry of Education, Shanghai Jiao Tong University School of Medicine (SJTU-SM), Shanghai 200025, China. 2 Institute of Health Sciences, Shanghai Institutes for Biological Sciences of Chinese Academy of Sciences and SJTU-SM, Shanghai 200025, China. -

Human Brain Organoids Reveal Accelerated Development of Cortical Neuron Classes As a Shared Feature of Autism Risk Genes
bioRxiv preprint doi: https://doi.org/10.1101/2020.11.10.376509; this version posted November 12, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Human brain organoids reveal accelerated development of cortical neuron classes as a shared feature of autism risk genes Bruna Paulsen1,2,†, Silvia Velasco1,2,†,#, Amanda J. Kedaigle1,2,3,†, Martina Pigoni1,2,†, Giorgia Quadrato4,5 Anthony Deo2,6,7,8, Xian Adiconis2,3, Ana Uzquiano1,2, Kwanho Kim1,2,3, Sean K. Simmons2,3, Kalliopi Tsafou2, Alex Albanese9, Rafaela Sartore1,2, Catherine Abbate1,2, Ashley Tucewicz1,2, Samantha Smith1,2, Kwanghun Chung9,10,11,12, Kasper Lage2,13, Aviv Regev3,14, Joshua Z. Levin2,3, Paola Arlotta1,2,# † These authors contributed equally to the work # Correspondence should be addressed to [email protected] and [email protected] 1 Department of Stem Cell and Regenerative Biology, Harvard University, Cambridge, MA 02138, USA 2 Stanley Center for Psychiatric Research, Broad Institute of MIT and Harvard, Cambridge, MA 02142, USA 3 Klarman Cell Observatory, Broad Institute of MIT and Harvard, Cambridge, MA 02142, USA 4 Department of Stem Cell Biology and Regenerative Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA 90033, USA; 5 Eli and Edythe Broad CIRM Center for Regenerative Medicine and Stem Cell Research at the University of Southern California, Los Angeles, CA 90033, USA. 6 Department of Psychiatry, -

Chd8 Mutation Leads to Autistic-Like Behaviors and Impaired Striatal Circuits
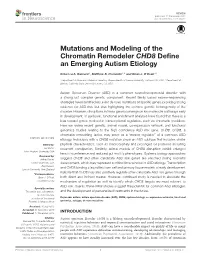
Chd8 Mutation Leads to Autistic-like Behaviors and Impaired Striatal Circuits The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Platt, Randall J.; Zhou, Yang; Slaymaker, Ian M.; Shetty, Ashwin S.; Weisbach, Niels R.; Kim, Jin-Ah; Sharma, Jitendra et al. “Chd8 Mutation Leads to Autistic-Like Behaviors and Impaired Striatal Circuits.” Cell Reports 19, no. 2 (April 2017): 335–350 © 2017 The Authors As Published http://dx.doi.org/10.1016/j.celrep.2017.03.052 Publisher Elsevier Version Final published version Citable link http://hdl.handle.net/1721.1/109830 Terms of Use Creative Commons Attribution-NonCommercial-NoDerivs License Detailed Terms http://creativecommons.org/licenses/by-nc-nd/4.0/ Article Chd8 Mutation Leads to Autistic-like Behaviors and Impaired Striatal Circuits Graphical Abstract Authors Randall J. Platt, Yang Zhou, Ian M. Slaymaker, ..., Gerald R. Crabtree, Guoping Feng, Feng Zhang Correspondence [email protected] (R.J.P.), [email protected] (F.Z.) Macrocephaly Gene dysregulation In Brief Platt et al. demonstrate that loss-of- +/– Chd8 function mutation of the high-confidence ASD-associated gene Chd8 results in behavioral and synaptic defects in mice. ASD-like behavior Synaptic dysfunction Highlights À d Chd8+/ mice display macrocephaly and ASD-like behaviors d Major insult to genome regulation and cellular processes in Chd8+/– mice d LOF Chd8 mutations cause synaptic dysfunction in the nucleus accumbens d NAc-specific perturbation of Chd8 in adult Cas9 mice recapitulates behavior Platt et al., 2017, Cell Reports 19, 335–350 April 11, 2017 ª 2017 The Authors. -

A 40-Cm Region on Chromosome 14 Plays a Critical Role in the Development of Virus Persistence, Demyelination, Brain Pathology An
A 40-cM Region on Chromosome 14 Plays a Critical Role in the Development of Virus Persistence, Demyelination, Brain Pathology and Neurologic Deficits in a Murine Viral Model of Multiple Sclerosis Shunya Nakane, Laurie Zoecklein, Jeffrey Gamez, Louisa Papke, Kevin Pavelko, Jean- François Bureau, Michel Brahic, Larry Pease, Moses Rodriguez To cite this version: Shunya Nakane, Laurie Zoecklein, Jeffrey Gamez, Louisa Papke, Kevin Pavelko, et al.. A 40-cM Region on Chromosome 14 Plays a Critical Role in the Development of Virus Persistence, Demyelination, Brain Pathology and Neurologic Deficits in a Murine Viral Model of Multiple Sclerosis. Brain Pathology, Wiley, 2003, 13 (4), pp.519-533. 10.1111/j.1750-3639.2003.tb00482.x. hal-03223233 HAL Id: hal-03223233 https://hal.archives-ouvertes.fr/hal-03223233 Submitted on 10 May 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. RESEARCH ARTICLE A 40-cM Region on Chromosome 14 Plays a Critical Role in the Development of Virus Persistence, Demyelination, Brain Pathology and Neurologic Deficits in a Murine Viral Model of Multiple Sclerosis Shunya Nakane1; Laurie J. Zoecklein1; Jeffrey D. Introduction Gamez1; Louisa M. Papke1; Kevin D. -
Mutations and Modeling of the Chromatin Remodeler CHD8 Define an Emerging Autism Etiology
REVIEW published: 17 December 2015 doi: 10.3389/fnins.2015.00477 Mutations and Modeling of the Chromatin Remodeler CHD8 Define an Emerging Autism Etiology Rebecca A. Barnard 1, Matthew B. Pomaville 1, 2 and Brian J. O’Roak 1* 1 Department of Molecular & Medical Genetics, Oregon Health & Science University, Portland, OR, USA, 2 Department of Biology, California State University, Fresno, CA, USA Autism Spectrum Disorder (ASD) is a common neurodevelopmental disorder with a strong but complex genetic component. Recent family based exome-sequencing strategies have identified recurrent de novo mutations at specific genes, providing strong evidence for ASD risk, but also highlighting the extreme genetic heterogeneity of the disorder. However, disruptions in these genes converge on key molecular pathways early in development. In particular, functional enrichment analyses have found that there is a bias toward genes involved in transcriptional regulation, such as chromatin modifiers. Here we review recent genetic, animal model, co-expression network, and functional genomics studies relating to the high confidence ASD risk gene, CHD8. CHD8, a chromatin remodeling factor, may serve as a “master regulator” of a common ASD etiology. Individuals with a CHD8 mutation show an ASD subtype that includes similar Edited by: physical characteristics, such as macrocephaly and prolonged GI problems including Gul Dolen, recurrent constipation. Similarly, animal models of CHD8 disruption exhibit enlarged Johns Hopkins University, USA head circumference and reduced gut motility phenotypes. Systems biology approaches Reviewed by: Jeffrey Varner, suggest CHD8 and other candidate ASD risk genes are enriched during mid-fetal Cornell University, USA development, which may represent a critical time window in ASD etiology. -

The Highly Conserved Defender Against the Death 1 (DAD1) Gene
FEBS Letters 363 (1995) 304-306 FEBS 15393 The highly conserved defender against the death 1 (DAD 1) gene maps to human chromosome 14qll-q12 and mouse chromosome 14 and has plant and nematode homologs Suneel S. Apte"'*, Marie-Genevieve Mattei b, Michael F. Seldin c, Bjorn R. Olsen a aDepartment of Cell Biology, Harvard Medical School, 25 Shattuck St., Boston, MA 02115, USA bHopital d'Enfants, INSERM U 406, Groupe Hospitalier de la Timone, 13385 Marseille Cedex 5, France CDepartments of Medicine and Microbiology, Duke University School of Medicine, Box 3380, Durham, NC 27710, USA Received 8 March 1995 demonstrated the remarkable degree of conservation of this Abstract We have cloned the cDNA encoding the mouse DAD1 protein in these 3 species [5]. It is identical in humans and (defender against apoptotic cell death) protein. While showing an hamster and varies only slightly in Xenopus. No homologies expected high homology with the previously cloned human and with previously isolated genes have been reported, and neither Xenopus DADl-encoding cDNAs, this sequence has striking ho- mology to partial eDNA sequences reported from Oo sativa (rice) the precise intracellular localization nor the protein-protein and C. elegans (nematode), suggesting the existence of plant and interactions of DAD1 are currently known [5]. invertebrate homologs of this highly conserved gene. The human We report the cloning of the mouse Dadl eDNA. As ex- and mouse DAD1 genes map to chromosome 14qll-q12 and pected, this is similar to the previously cloned human and chromosome 14, respectively. This mapping data supports and hamster cDNAs. -

Novel Targets of Apparently Idiopathic Male Infertility
International Journal of Molecular Sciences Review Molecular Biology of Spermatogenesis: Novel Targets of Apparently Idiopathic Male Infertility Rossella Cannarella * , Rosita A. Condorelli , Laura M. Mongioì, Sandro La Vignera * and Aldo E. Calogero Department of Clinical and Experimental Medicine, University of Catania, 95123 Catania, Italy; [email protected] (R.A.C.); [email protected] (L.M.M.); [email protected] (A.E.C.) * Correspondence: [email protected] (R.C.); [email protected] (S.L.V.) Received: 8 February 2020; Accepted: 2 March 2020; Published: 3 March 2020 Abstract: Male infertility affects half of infertile couples and, currently, a relevant percentage of cases of male infertility is considered as idiopathic. Although the male contribution to human fertilization has traditionally been restricted to sperm DNA, current evidence suggest that a relevant number of sperm transcripts and proteins are involved in acrosome reactions, sperm-oocyte fusion and, once released into the oocyte, embryo growth and development. The aim of this review is to provide updated and comprehensive insight into the molecular biology of spermatogenesis, including evidence on spermatogenetic failure and underlining the role of the sperm-carried molecular factors involved in oocyte fertilization and embryo growth. This represents the first step in the identification of new possible diagnostic and, possibly, therapeutic markers in the field of apparently idiopathic male infertility. Keywords: spermatogenetic failure; embryo growth; male infertility; spermatogenesis; recurrent pregnancy loss; sperm proteome; DNA fragmentation; sperm transcriptome 1. Introduction Infertility is a widespread condition in industrialized countries, affecting up to 15% of couples of childbearing age [1]. It is defined as the inability to achieve conception after 1–2 years of unprotected sexual intercourse [2]. -

Integrative Genomic Analysis of Hnrnp L Splicing Regulation
University of Pennsylvania ScholarlyCommons Publicly Accessible Penn Dissertations 2015 Terrae Incognitae: Integrative Genomic Analysis of Hnrnp L Splicing Regulation Brian Sebastian Cole University of Pennsylvania, [email protected] Follow this and additional works at: https://repository.upenn.edu/edissertations Part of the Allergy and Immunology Commons, Biochemistry Commons, Bioinformatics Commons, Immunology and Infectious Disease Commons, and the Medical Immunology Commons Recommended Citation Cole, Brian Sebastian, "Terrae Incognitae: Integrative Genomic Analysis of Hnrnp L Splicing Regulation" (2015). Publicly Accessible Penn Dissertations. 1664. https://repository.upenn.edu/edissertations/1664 This paper is posted at ScholarlyCommons. https://repository.upenn.edu/edissertations/1664 For more information, please contact [email protected]. Terrae Incognitae: Integrative Genomic Analysis of Hnrnp L Splicing Regulation Abstract Alternative splicing is a critical component of human gene control that generates functional diversity from a limited genome. Defects in alternative splicing are associated with disease in humans. Alternative splicing is regulated developmentally and physiologically by the combinatorial actions of cis- and trans- acting factors, including RNA binding proteins that regulate splicing through sequence-specific interactions with pre-mRNAs. In T cells, the splicing regulator hnRNP L is an essential factor that regulates alternative splicing of physiologically important mRNAs, however the broader physical and functional impact of hnRNP L remains unknown. In this dissertation, I present analysis of hnRNP L-RNA interactions with CLIP-seq, which identifies transcriptome-wide binding sites and uncovers novel functional targets. I then use functional genomics studies to define pre-mRNA processing alterations induced by hnRNP L depletion, chief among which is cassette-type alternative splicing.