Strengthening Health Systems Through Organizing Communities (SHASTO) Baseline Survey Report October 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Investor Protection in a Disclosure Regime: an International and Comparative Perspective on Initial Public Offerings in the Bangladesh Securities Market
University of Wollongong Thesis Collections University of Wollongong Thesis Collection University of Wollongong Year 2003 Investor protection in a disclosure regime: an international and comparative perspective on initial public offerings in the Bangladesh securities market S. M. Solaiman University of Wollongong Solaiman, S. M., Investor protection in a disclosure regime: an international and comparative perspective on initial public offerings in the Bangladesh securities market, Doctor of Philoso- phy thesis, Faculty of Law, University of Wollongong, 2003. http://ro.uow.edu.au/theses/1855 This paper is posted at Research Online. Investor Protection in a Disclosure Regime: An International and Comparative Perspective on Initial Public Offerings in the Bangladesh Securities Market A thesis submitted in fulfilment of the requirements for the award of the degree DOCTOR OF PHILOSOPHY from UNIVERSITY OF WOLLONGONG By S M Solaiman LLM (Western Sydney) LLM (Dhaka) LLB Hons (Raj) FACULTY OF LAW 2003 THESIS DECLARATION This is to certify that I, S M Solaiman, being a candidate for the degree of Doctor of Philosophy (PhD), am fully aware of the University of Wollongong's rules and procedures relating to the preparation, submission, retention and use of higher degree theses, and its policy on intellectual property. I acknowledge that the University requires the thesis to be retained in the Library for record purposes and that within copyright privileges of the author, it should be accessible for consultation and copying at the discretion of the Library officer in charge and in accordance with the Copyright Act (1968). I authorise the University of Wollongong to publish an abstract of this thesis. -

Bangladesh: Human Rights Report 2015
BANGLADESH: HUMAN RIGHTS REPORT 2015 Odhikar Report 1 Contents Odhikar Report .................................................................................................................................. 1 EXECUTIVE SUMMARY ............................................................................................................... 4 Detailed Report ............................................................................................................................... 12 A. Political Situation ....................................................................................................................... 13 On average, 16 persons were killed in political violence every month .......................................... 13 Examples of political violence ..................................................................................................... 14 B. Elections ..................................................................................................................................... 17 City Corporation Elections 2015 .................................................................................................. 17 By-election in Dohar Upazila ....................................................................................................... 18 Municipality Elections 2015 ........................................................................................................ 18 Pre-election violence .................................................................................................................. -

Recruitment and Placement of Bangladeshi Migrant Workers an Evaluation of the Process
1 RECRUITMENT AND PLACEMENT OF BANGLADESHI MIGRANT WORKERS AN EVALUATION OF THE PROCESS INTERNATIONAL ORGANIZATION FOR MIGRATION (IOM) NOVEMBER 2002 2 Opinions expressed in the publications are those of the researcher and do not necessarily reflect the views of the International Organization for Migration. IOM is committed to the principle that humane and orderly migration benefits migrants and society. As an inter-governmental body, IOM acts with its partners in the international community to: assist in meeting the operational challenges of migration; advance understanding of migration issues; encourage social and economic development through migration; and work towards effective respect of the human dignity and well-being of migrants. Publisher International Organization for Migration (IOM), Regional Office for South Asia House # 3A, Road # 50, Gulshan : 2, Dhaka : 1212, Bangladesh Telephone : +88-02-8814604, Fax : +88-02-8817701 E-mail : [email protected] Internet : http://www.iom.int Funded by United Nations Development Programme (UNDP), Dhaka ISBN : 984-32-0435-2 © [2002] International Organization for Migration (IOM) Printed by Bengal Com-print 23 F/1, Free School Street, Panthapath, Dhaka-1205 Telephone : 8611142, 8611766 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means electronic, mechanical, photocopying, recording, or otherwise without prior written permission of the publisher. 3 RECRUITMENT AND PLACEMENT OF BANGLADESHI MIGRANT WORKERS -

Housing the Urban Poor: Planning, Business and Politics a Case Study of Duaripara Slum, Dhaka City, Bangladesh
Housing the Urban Poor: Planning, Business and Politics A Case Study of Duaripara Slum, Dhaka city, Bangladesh Kh. Md. Nahiduzzaman Thesis submitted to the Department of Geography, Faculty of Social Sciences and Technology Management, Norwegian University of Science and Technology (NTNU), in partial fulfillment of the requirements for Master of Philosophy in Development Studies, specializing in Geography. Norway, May 2006 NTNU Declaration Except where duly acknowledged, I certify that this thesis is my own work under the supervision of Professor Axel Baudouin of the Department of Geography, Norwegian University of Science and Technology, Trondheim, Norway Kh. Md. Nahiduzzaman Abstract This study is conducted on Duripara slum of Dhaka city which is one of the fastest growing megalopolis and primate cities not only among the developing but also among the developed countries. The high rate of urbanization has posed a challenging dimension to the central, local govt. and concerned development authority. In Dhaka about 50% of the total urban population is poor and in the urbanization process the poor are the major contributors which can be characterized as urbanization of poverty. In response to the emerging urban problems, the development authority makes plan to solve those problems as well as to manage the urban growth. By focusing on the housing issue for the urban poor in Dhaka Metropolitan Development Plan (DMDP), this study is aimed to find out the distortion between plan and reality through making a connection between such planning practice, political connections and business dealings. Knowledge gained from the reviewed literature, structuration theory, actors oriented approach, controversies of urban growth and theoretical framework were used as interpretative guide for the study. -

Special Original Jurisdiction)
1 IN THE SUPREME COURT OF BANGLADESH HIGH COURT DIVISION (SPECIAL ORIGINAL JURISDICTION) WRIT PETITION NO. ............. OF 2013. IN THE MATTER OF: An application under Article 102 of the Constitution of the People’s Republic of Bangladesh. AND IN THE MATTER OF: Public Interest Litigation (PIL). AND IN THE MATTER OF: 1. Human Rights and Peace for Bangladesh (HRPB), represented by it’s Secretary, Advocate Asaduzzaman Siddique, Hall No. 2, Supreme Court Bar Association Bhaban, Dhaka, Bangladesh. .............Petitioner. -V E R S U S- 1. Bangladesh represented by the Secretary, Ministry of Home Affairs, Bangladesh Secretariat , P.S.: Shahbag, District: Dhaka. 2. The Secretary, Ministry of Health, Bangladesh Secretariat , P.S.: Shahbag, District: Dhaka. 3. The Director General, Health, Health Directorate, Mohakhali, Dhaka, Bangladesh. 4. The Director, Dhaka Medical College Hospital, Dhaka, Bangladesh. 5. Inspector General of Police (IGP), Police Head Quarter Bhaban, Ramna, Dhaka, Bangladesh. 6. The Joint Commissioner, Detective Branch (DB), DB Head Quarter, Mintu Road, Dhaka, Bangladesh. 7. The Police Commissioner, Dhaka Metropolitan Police (DMP), District- Dhaka. [ 8. The Deputy Police Commissioner, (Motijheel Zone), Motijheel, Dhaka, Bangladesh 9. The officer in charge, Motijheel Thana, P.S. Motijheel, District-Dhaka, Bangladesh ..................Respondents. AND IN THE MATTER OF: For a direction upon the respondents to find out the real culprit who has tortured the journalist Nadia Sharmin at Motijheel at the meeting of Hefajote Islam and complete the investigation as early as possible and ensure the trail of the miscreant in accordance with law. 2 G R O U N D S I. For that Article 31 of the constitution of Bangladesh has provided a provision that ‘to enjoy protection of law and to be treated in accordance with law and only in accordance with law’ but in the instant case it has been violated by the law enforcing agencies. -

Annual Report for the Year Ended 31 December 2017
ANNUAL REPORT 2017 COMMITTED TO GROWING STRONGER TOGETHER Committed to Growing Stronger Together Southeast Bank, already a strong Bank, is thriving to be efficient ways. Our maturing understanding of corporate stronger in close cooperation and association with its social responsibility is part and parcel of our approach to stakeholders. We maintain and cherish our relationship drive our business forward. with them; from customers, employees and shareholders to suppliers, business partners and wider community. We Today the Bank is more profitable, more flexible and look forward to collectively growing our business together better structured. It is a powerhouse with outstanding in the coming years. As an experienced Bank, we always solutions and attractive products for customers, excellent have the first-mover advantage to offer the best-in-class opportunities for employees and exceptional potential value-added services to the customers. Our people are for investors. In the growth graph, the Bank has been honest, skilled and efficient. They are better sourced, continuously making good profit and declaring good better motivated and better incentivized. We have the dividend to shareholders. The curve of growth keeps power and commitment today to write our future – we shall write it together. Together we are growing stronger soaring upward everyday. Every year, we leave an indelible and together we shall reach new heights of success. We stamp of success on the annals of Bank’s history. For us, are destined to grow because we have proved our strength yesterday is but today’s memory and tomorrow is today’s in the banking sector. We are accessible, committed vision. -
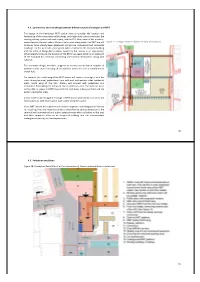
30 4.2. Connectivity and Interchange Between Different Modes of Transport and MRT the Design of the Kamalapur MRT Station Have T
>5<5 ('',".",1'"',*!' ,/'"*',&(+(,*'+)(*,' ! ," ' ( -! &%).+ ,--"(' !/ -( (',"+ -! %(-"(' ' .'-"('"' (-!"('"-+&"'%."%"' ,4(-!"'-+:",-+"-'(&&.-+4-! 1",-"' +"%02,2,-&'-+$%2(.-4'-! 7%,(4,(&(-!)+"/-%2: (0'%'('-!,-,"(.-+"+.%++(4%(' 0!"!-!%"'0"%% &#/5+ $%( # %!$!%# $"!#%$ ('-"'.4 !/ %+2 ' /%() , !" !:+",(&&+"%'+,"'-"% ."%"' ,7'-!0,-,"4()' +',)"'-0'-!-+&"'%."%"' ' -! (" ( ' %,! +"%024 (0' 2 -! +"%02 ", ' ())(+-.'"-27 -!+())(+-.'"-",+-!%(-"('(-!.,)(-0!"!",'1-',"(' ( -! " ., -+&"'%4 (''-"' "'-+'-"('% ,-"'-"(', %(' 0"-! '-"('%7 !,!&-"," '4-!+(+4,. ,-,-(/%()'"'-+%"'$(&)%1( -"/"-",+-!+-!'+%(-"' %%-!-"/"-",.'+('+((,&.%-":&(% -+',"-!.7 (+1&)%4-!'(+-!0"' (-!,--"('0"%%(''-),,' +,0"-!-! &"'+"%02-+&"'%4),-+"',+(&(-!,-'0,-+',",+,"'-"% +,7 (.-! 0"' ( -! ,--"(' 0"%% (''- 0"-! ),-+"' ' (&&.-+,+(&(-"#!%,--"('( "'G4%(%.,.,+,7!%(%.,.,+, 0"%%%-(,,-!.,-+&"'%4(&&.-++"%02-+&"'%'-! ,-+'+,"'-"%+,7 %"'+'(+-!,(.-!%(' -+('- (,--"(''%(%.,-"/"-",0"%% !/()-"(',-(-$/'- (()').%"' +',)7 "',--"('/%()&'-0"%%'-(' (-"-0"-!' %,!"%02 (+*."+"' %'4('"''-"/'-((+-!&-(/%()1-',"('(-! -+&"'%0"-!(&&+"%').%"'-+-"'&'-0!"!",%$"' "'-!+ ' -!"+ (+)(+- (" , ' "'- +- ."%"' -!- ' (&&(- .'+ +(.')+$"' (+-!(&)%1.,+,7 DA >5=5 +,*"'"*-%,"(' &#/6+! "%&% %% %#$%! !%%! #! &%##&##! DB &#/7+! "%&%! ,!%%! #! �.+! "%&%! ,!%%! #! !(+-:-+&"'-+/'-"(' !(+-:-+&"'-+/'-"(' (' :-+&"'-+/'-"(' (' :-+&"'-+/'-"(' DC >5>5 !"-%*++')*$"' �/+! "%&% (%'&##!"-! "# DD >5?5 (%-++,()'/","' �+! "%&% (%!&$$%!" (% # DE ?5 (&(-!"'-+/'-"(',",.,,"'(')-.%)%''"' ',!&-"," ''"&)%&'-"'"+'-)!,,7 -
Paper Title -.Us.Org
ABC Research Alert Vol 9, Number 1 Published Online: 16 April 2021 https://abc.us.org/ojs/index.php/abcra Radiation Risk Assessment on Public in Motijheel Thana, Dhaka, Bangladesh Mohammed Belayet Hossain¹, M. S. Rahman²*, Mohammad Amir Hossain Bhuiyan3, S. Yeasmin4 1,3Department of Environmental Science, Jahangirnagar University, Dhaka-1342, BANGLADESH *2,4Health Physics Division, Atomic Energy Centre, Shahbag, Dhaka-1000, BANGLADESH *([email protected]) This journal is licensed under a Creative Commons Attribution-Noncommercial 4.0 International License (CC-BY-NC). Articles can be read and shared for noncommercial purposes under the following conditions: • BY: Attribution must be given to the original source (Attribution) • NC: Works may not be used for commercial purposes (Noncommercial) This license lets others remix, tweak, and build upon your work non-commercially, and although their new works must also acknowledge you and be non-commercial, they don’t have to license their derivative works on the same terms. License Deed Link: http://creativecommons.org/licenses/by-nc/4.0/ Legal Code Link: http://creativecommons.org/licenses/by-nc/4.0/legalcode ABC Research Alert uses the CC BY-NC to protect the author's work from misuse. Abstract Objective: The pollution free environment is required for healthy life. The real-time radiation monitoring is very important for radiation hazard detection in the environment. The excess life-time cancer risk (ELCR) on public is to assess based on the real-time radiation monitoring data in the area. Methods: The real-time radiation monitoring was performed using portable digital radiation monitoring device. This real-time digital portable radiation monitoring device meets all European CE standards as well as the American “FCC 15 standard”. -

Vehicular Emission Inventory Analysis of a Residential and a Commercial Area of Dhaka City
Proceedings of the 3rd International Conference on Civil Engineering for Sustainable Development (ICCESD 2016), 12~14 February 2016, KUET, Khulna, Bangladesh (ISBN: 978-984-34-0265-3) VEHICULAR EMISSION INVENTORY ANALYSIS OF A RESIDENTIAL AND A COMMERCIAL AREA OF DHAKA CITY M. Alam*1 and M. S. Hoque2 1 Under Graduation Student ,Bangladesh University of Engineering and Technology, Bangladesh, e-mail: [email protected] 2 Professor, Bangladesh University of Engineering and Technology, Bangladesh, e-mail: [email protected] ABSTRACT ‘Sustainable Transportation System’ has become one of the biggest clichés around the world nowadays; especially for a country like Bangladesh which has been ranked 4th among 91 countries with worst urban air quality in the latest air pollution monitoring report of World Health Organization (WHO). Amongst various sources of air pollution, transportation sector alone is responsible for 23% of world’s Green House Gas (GHG) emissions with about 75% coming from road vehicles. This Study is aimed at determining transport (vehicular) footprint of a residential (Dhanmondi) and a commercial (Motijheel) area and comparing them with their corresponding bio-capacity. The analogy also compares six global emission parameters between these two areas which include CO2, CH4, SO2, Suspended Particulate Matter, Black Carbon and Organic Carbon. Traffic volume data were collected through video footages from 8 and 10 different major links of Dhanmondi and Motijheel Thana respectively. By transcribing different types of motorized vehicles manually from footages and using vehicular expansion factors, the Annual Average Daily Traffic (AADT) of each vehicle types are calculated. The annual emissions of aforementioned six parameters are calculated using percentage share of fuel types and individual emission factors for each type of vehicles collected from international literatures and slightly modified in context of Dhaka. -

Development of Congestion Maps for Selected Corridors of Dhaka City Using Instrumented Vehicle
DEVELOPMENT OF CONGESTION MAPS FOR SELECTED CORRIDORS OF DHAKA CITY USING INSTRUMENTED VEHICLE. MST. TAHNIN TARIQ DEPARTMENT OF CIVIL ENGINEERING BANGLADESH UNIVERSITY OF ENGINEERING AND TECHNOLOGY (BUET) Dhaka, Bangladesh November, 2015 DEVELOPMENT OF CONGESTION MAPS FOR SELECTED CORRIDORS OF DHAKA CITY USING INSTRUMENTED VEHICLE. Bangladesh University of Engineering and Technology A THESIS SUBMITTED TO THE DEPARTMENT OF CIVIL ENGINEERING IN PARTIAL FULFILLMENT OF THE REQUIREMENT FOR THE DEGREE OF MASTERS OF SCIENCE IN CIVIL ENGINEERING (TRANSPORTAION) A THESIS SUBMITTED BY MST. TAHNIN TARIQ DEPARTMENT OF CIVIL ENGINEERING BANGLADESH UNIVERSITY OF ENGINEERING AND TECHNOLOGY (BUET) Dhaka, Bangladesh November, 2015 This thesis titled "Developmenl of congestion maps lbr selecled corridors ol' Dh:rkn cify using instrumented vehicle.". submitted by Mst. Tahnin Tariq. Iloll No. 0412042405F, Session: Aplil 2012, has been accepted as satisthctory in prrt ia I fulfilhnent ol the requirernent for the degree of Master of Science in Civil Engineering (Transportation) on I 0rl' Novenrber, 201 5. BOARD OF EXAMINERS (ass_- Dr. 'fanrveer Hasan. Chairman Professor (SLrperv isor.; Depaftnlent of Civil Engineering, BUET Dr. K.A.M. Abdul Muqtadir Menrber Professor and Head (Ex-ot'ficio) Department ol Civil Engineering. BUET Dr. Md. Mizanur Rahman Member Prolessor Department of Civil Engineering, BUET '6:u3 r.^"-- IL-''-h *-o t't- Dr. Farzana Rahman Memher Associate Prot'essor ( External) Depa ment olCivil Engineering. University of Asia Pacitic (UAP) CANDIDATE'S DECLARATION Declared that, the studies in this thesis is the result of research work by author, except for the contents where specific reference has been made to the work ofothers. The thesis or any part of the thesis has not been submitted to any other university or educational institute for the award for any degree, except for publication. -

Okf"Kzd Fjiksvz 2014 - 2015
okf"kZd fjiksVZ 2014 - 2015 Hkkjrh; bfrgkl vuqlaèkku ifj"kn~ 35] fiQjks”k'kkg jksM+] ubZ fnYyh&110001 izdk'ku lg;ksx lnL; lfpo mifuns'kd ¼iz'kklu½ lykgdkj ¼lEiknu@izdk'ku½ iathdj.k la[;k % ,l&5339 fnukad 7 ekpZ 1972 lokZfèkdkj © Hkk-bZ-v-i- o"kZ 2016 izdk'kd lnL; lfpo Hkkjrh; bfrgkl vuqlaèkku ifj"kn~ 35 fQjkst+'kkg jksM+] ubZ fnYyh&110 001 Qksu % 011&23387877] 011&23386033( QSDl % 011&23387829] 011&23383421 Email: [email protected] Web: www.ichr.ac.in eqnzd % ekud ifCyds'kUl izk- fy-] ch&7] ljLorh dkWeIysDl] lqHkk"k pkSd] y{eh uxj] fnYyh&110 092 e-mail: [email protected] www.manakpublications.in Qksu % 011&22453894] 011&22042529 fo"k;&lwph rkfydk lwph v Hkkx&I ([k.M) I lkekU; 1 II vk; 2014&15 9 III 'kks/k çksRlkgu dk;Zdyki 2014&15 13 IV Hkk-b-v-i- ds çdk'ku 2014&15 27 V Hkk-b-v-i- if=dk % bafM;u fgLVksfjdy fjO;q ¼vkb,pvkj½ ,oa bfrgkl fgUnh 'kks/k if=dk rFkk Hkkjrh; bfrgkl vuqla/kku ifj"kn~ dk U;wt+ysVj 33 VI Hkk-b-v-i- fo'ks"k vuqla/kku ifj;kstuk,a 2014&15 41 VII Hkk-b-v-i- }kjk vk;ksftr xksf"B;ka vkSj ifjlaokn 2014&15 49 VIII iqLrkdky;&lg&çys[ku dsaæ 2014&15 53 IX Hkk-b-v-i- {ks=h; dsaæksa ds dk;Zdyki 2014&15 57 X fgUnh i[kokM+k 2014&15 75 Hkkx&II ifjf'k"V I 27-03-2015 ds ifj"kn~ osQ u;s lnL;x.k (26 ekpZ 2015 rd) 79 II iz'kklfud lfefr ,oa vuqlaèkku ifj;kstuk lfefr osQ lnL; 2014&2015 89 II (d) vU; lykgdkj lfefr;ksa ds lnL;ksa dh ukelwph 2014&2015 93 III 31 ekpZ 2015 dh fLFkfr ds vuqlkj Hkk-b-v-i- deZpkfj;ksa dh la[;k 101 IV o"kZ 2014&2015 osQ lacaèk esa Hkk-b-v-i- osQ okf"kZd ys[ks 107 V Hkk-b-v-i- osQ o"kZ 2014&2015 osQ ys[kksa -

2013-14 English
p PART – I SECTIONS Section I GENERAL p p INDIAN COUNCIL OF HISTORICAL RESEARCH ANNUAL REPORT 2013-2014 GENERAL The Indian Council of Historical Research (ICHR) is an autonomous organization under Ministry of Human Resources Development (MHRD), Government of India duly registered, vide Registration No.S 5339 dated 7th March 1972 under Societies Registration Act (Act.xxi of 1860) being an Act for registration of Literary, Scientific and Charitable Societies. The Govt. of India (now, MHRD) on 29th March 1972 on the recommendation of a Working Group set up by the Govt. of Indian in December 1971 comprising Professor R.S. Sharma, Patna University (Chairman); Professor Satish Chandra, Jawaharlal Nehru University; Professor Tapan Raychaudhuri, Delhi University; Dr. S.N. Prasad, Director National Archives; Shri J. Veeraraghvan, Director (Internal Finance), Ministry of Education and Social Welfare; and Smt. S. Doraiswami, Deputy Education Adviser, Ministry of Education and Social Welfare. The primary objective of the Council is to promote and give direction to historical research and to encourage and foster objective and scientific writing of history. Enhancing the academic standard of the output of ICHR activities has been foremost objective in our agenda. The broad aims of the Council as laid down in the Memorandum of Association (MoA) are to bring historians together and provide a forum exchange of views between them and to give a national direction to an objective and rational presentation and interpretation of history, to sponsor historical research programmes and projects and to assist institutions and organizations engaged in historical research. The Council also awards and administers various categories of fellowships for historical research.