Zacks Small-Cap Research April 12, 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Fig. L COMPOSITIONS and METHODS to INHIBIT STEM CELL and PROGENITOR CELL BINDING to LYMPHOID TISSUE and for REGENERATING GERMINAL CENTERS in LYMPHATIC TISSUES
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date Χ 23 February 2012 (23.02.2012) WO 2U12/U24519ft ft A2 (51) International Patent Classification: AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, A61K 31/00 (2006.01) CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (21) International Application Number: HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, PCT/US201 1/048297 KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, (22) International Filing Date: ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, 18 August 201 1 (18.08.201 1) NO, NZ, OM, PE, PG, PH, PL, PT, QA, RO, RS, RU, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, (25) Filing Language: English TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (26) Publication Language: English ZW. (30) Priority Data: (84) Designated States (unless otherwise indicated, for every 61/374,943 18 August 2010 (18.08.2010) US kind of regional protection available): ARIPO (BW, GH, 61/441,485 10 February 201 1 (10.02.201 1) US GM, KE, LR, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, 61/449,372 4 March 201 1 (04.03.201 1) US ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, TJ, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, (72) Inventor; and EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, ΓΓ, LT, LU, (71) Applicant : DEISHER, Theresa [US/US]; 1420 Fifth LV, MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, Avenue, Seattle, WA 98101 (US). -

Of Anti-CD3 Action? This Information Is Current As of September 26, 2021
Differential Response of Regulatory and Conventional CD4 + Lymphocytes to CD3 Engagement: Clues to a Possible Mechanism of Anti-CD3 Action? This information is current as of September 26, 2021. Li Li, Junko Nishio, André van Maurik, Diane Mathis and Christophe Benoist J Immunol published online 28 August 2013 http://www.jimmunol.org/content/early/2013/08/27/jimmun ol.1300408 Downloaded from Supplementary http://www.jimmunol.org/content/suppl/2013/08/28/jimmunol.130040 Material 8.DC1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 26, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2013 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Published August 28, 2013, doi:10.4049/jimmunol.1300408 The Journal of Immunology Differential Response of Regulatory and Conventional CD4+ Lymphocytes to CD3 Engagement: Clues to a Possible Mechanism of Anti-CD3 Action? Li Li,* Junko Nishio,* Andre´ van Maurik,† Diane Mathis,* and Christophe Benoist* Several clinical trials have shown anti-CD3 treatment to be a promising therapy for autoimmune diabetes, but its mechanism of action remains unclear. -

Predictive QSAR Tools to Aid in Early Process Development of Monoclonal Antibodies
Predictive QSAR tools to aid in early process development of monoclonal antibodies John Micael Andreas Karlberg Published work submitted to Newcastle University for the degree of Doctor of Philosophy in the School of Engineering November 2019 Abstract Monoclonal antibodies (mAbs) have become one of the fastest growing markets for diagnostic and therapeutic treatments over the last 30 years with a global sales revenue around $89 billion reported in 2017. A popular framework widely used in pharmaceutical industries for designing manufacturing processes for mAbs is Quality by Design (QbD) due to providing a structured and systematic approach in investigation and screening process parameters that might influence the product quality. However, due to the large number of product quality attributes (CQAs) and process parameters that exist in an mAb process platform, extensive investigation is needed to characterise their impact on the product quality which makes the process development costly and time consuming. There is thus an urgent need for methods and tools that can be used for early risk-based selection of critical product properties and process factors to reduce the number of potential factors that have to be investigated, thereby aiding in speeding up the process development and reduce costs. In this study, a framework for predictive model development based on Quantitative Structure- Activity Relationship (QSAR) modelling was developed to link structural features and properties of mAbs to Hydrophobic Interaction Chromatography (HIC) retention times and expressed mAb yield from HEK cells. Model development was based on a structured approach for incremental model refinement and evaluation that aided in increasing model performance until becoming acceptable in accordance to the OECD guidelines for QSAR models. -

Psoriasis and the New Biologic Agents: Interrupting a T-AP Dance
Review Synthèse Psoriasis and the new biologic agents: interrupting a T-AP dance Scott R.A. Walsh, Neil H. Shear Abstract corticosteroids, tar, anthralin, calcipotriol or tazarotene be- come cumbersome to apply as lesional surface area increases. PSORIASIS IS AN IMMUNE-MEDIATED SKIN DISEASE in which chronic T- Furthermore, potential side effects of these therapies increase cell stimulation by antigen-presenting cells (APC) occurs in the with the level of application. Nevertheless, topical treatment skin. This interplay between the T-cell and APC has been likened remains an adjunct in more severe disease to limit the re- to a “T-AP dance” where specific steps must occur in sequence to quirement for more aggressive therapies. Phototherapy is a result in T-cell activation and the disease phenotype; otherwise T- popular option in the treatment of more widespread disease. cell anergy would occur. Several novel engineered proteins de- However, ultraviolet light is generally only available in larger signed to block specific steps in immune activation (biologic treatment centres, requires a major time commitment (2–3 agents) have demonstrated efficacy in the treatment of psoriasis. times per week for many months) and can be associated with These agents include fusion proteins, monoclonal antibodies and an increased risk of cutaneous neoplasms.6 For moderate to recombinant cytokines. These medications act at specific steps during the T-AP dance either to inhibit T-cell activation, costimu- severe disease, oral systemic immunosuppressives such as lation and subsequent proliferation of T-cells, lead to immune de- methotrexate and cyclosporine or oral retinoids are generally viation or induce specific cytokine blockades. -

Infliximab, Adalimumab and Golimumab for Treating Moderately
HEALTH TECHNOLOGY ASSESSMENT VOLUME 20 ISSUE 39 MAY 2016 ISSN 1366-5278 Infliximab, adalimumab and golimumab for treating moderately to severely active ulcerative colitis after the failure of conventional therapy (including a review of TA140 and TA262): clinical effectiveness systematic review and economic model Rachel Archer, Paul Tappenden, Shijie Ren, Marrissa Martyn-St James, Rebecca Harvey, Hasan Basarir, John Stevens, Christopher Carroll, Anna Cantrell, Alan Lobo and Sami Hoque DOI 10.3310/hta20390 Infliximab, adalimumab and golimumab for treating moderately to severely active ulcerative colitis after the failure of conventional therapy (including a review of TA140 and TA262): clinical effectiveness systematic review and economic model Rachel Archer,1* Paul Tappenden,1 Shijie Ren,1 Marrissa Martyn-St James,1 Rebecca Harvey,1 Hasan Basarir,1 John Stevens,1 Christopher Carroll,1 Anna Cantrell,1 Alan Lobo2 and Sami Hoque3 1Health Economics and Decision Science, School of Health and Related Research (ScHARR), University of Sheffield, Sheffield, UK 2Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK 3Barts Health NHS Trust, London, UK *Corresponding author Declared competing interests of authors: none Published May 2016 DOI: 10.3310/hta20390 This report should be referenced as follows: Archer R, Tappenden P, Ren S, Martyn-St James M, Harvey R, Basarir H, et al. Infliximab, adalimumab and golimumab for treating moderately to severely active ulcerative colitis after the failure of conventional therapy (including a review of TA140 and TA262): clinical effectiveness systematic review and economic model. Health Technol Assess 2016;20(39). Health Technology Assessment is indexed and abstracted in Index Medicus/MEDLINE, Excerpta Medica/EMBASE, Science Citation Index Expanded (SciSearch®) and Current Contents®/ Clinical Medicine. -

Delivery of Orally Administered Digestible Antibodies Using Nanoparticles
International Journal of Molecular Sciences Review Delivery of Orally Administered Digestible Antibodies Using Nanoparticles Toshihiko Tashima Tashima Laboratories of Arts and Sciences, 1239-5 Toriyama-cho, Kohoku-ku, Yokohama, Kanagawa 222-0035, Japan; [email protected] Abstract: Oral administration of medications is highly preferred in healthcare owing to its simplicity and convenience; however, problems of drug membrane permeability can arise with any administra- tion method in drug discovery and development. In particular, commonly used monoclonal antibody (mAb) drugs are directly injected through intravenous or subcutaneous routes across physical barri- ers such as the cell membrane, including the epithelium and endothelium. However, intravenous administration has disadvantages such as pain, discomfort, and stress. Oral administration is an ideal route for mAbs. Nonetheless, proteolysis and denaturation, in addition to membrane impermeability, pose serious challenges in delivering peroral mAbs to the systemic circulation, biologically, through enzymatic and acidic blocks and, physically, through the small intestinal epithelium barrier. A num- ber of clinical trials have been performed using oral mAbs for the local treatment of gastrointestinal diseases, some of which have adopted capsules or tablets as formulations. Surprisingly, no oral mAbs have been approved clinically. An enteric nanodelivery system can protect cargos from proteolysis and denaturation. Moreover, mAb cargos released in the small intestine may be delivered to the systemic circulation across the intestinal epithelium through receptor-mediated transcytosis. Oral Abs in milk are transported by neonatal Fc receptors to the systemic circulation in neonates. Thus, well-designed approaches can establish oral mAb delivery. In this review, I will introduce the imple- mentation and possibility of delivering orally administered mAbs with or without nanoparticles not Citation: Tashima, T. -
Report, Please Call the Telephone Number Listed
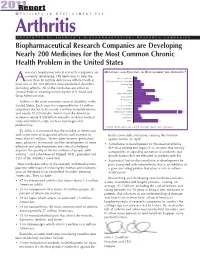
201R1e port M E D I C I N E S I N D E V E L O P M E N T F O R Arthritis P R E S E N T E D B Y A M E R I C A ’ S B I O P H A R M A C E U T I C A L R E S E A R C H C O M P A N I E S Biopharmaceutical Research Companies are Developing Nearly 200 Medicines for the Most Common Chronic Health Problem in the United States merica’s biopharmaceutical research companies are MEDICINES AND VACCINES IN DEVELOPMENT FOR ARTHRITIS* currently developing 198 medicines to help the Behcet’s Syndrome 3 more than 50 million Americans afflicted with at A Duchenne Muscular Dystrophy 6 least one of the 100 different musculoskeletal disorders, Fibromyalgia 9 including arthritis. All of the medicines are either in Gout 7 clinical trials or awaiting review by the U.S. Food and Lupus 19 Muscle Disorders 11 Drug Administration. Osteoarthritis 19 Osteoporosis 23 Arthritis is the most common cause of disability in the Pain 15 United States. Each year, it is responsible for 44 million Psoriatic Arthritis 7 outpatient doctor visits, nearly 1 million hospitalizations, Raynaud’s Disease 4 and nearly 10,000 deaths. And it costs the American Rheumatoid Arthritis 67 Scleroderma 6 economy nearly $128 billion annually in direct medical Spondylitis 7 costs and indirect costs, such as lost wages and Other 22 productivity. * Some medicines are listed in more than one category. -

Promising Therapeutic Targets for Treatment of Rheumatoid Arthritis
REVIEW published: 09 July 2021 doi: 10.3389/fimmu.2021.686155 Promising Therapeutic Targets for Treatment of Rheumatoid Arthritis † † Jie Huang 1 , Xuekun Fu 1 , Xinxin Chen 1, Zheng Li 1, Yuhong Huang 1 and Chao Liang 1,2* 1 Department of Biology, Southern University of Science and Technology, Shenzhen, China, 2 Institute of Integrated Bioinfomedicine and Translational Science (IBTS), School of Chinese Medicine, Hong Kong Baptist University, Hong Kong, China Rheumatoid arthritis (RA) is a systemic poly-articular chronic autoimmune joint disease that mainly damages the hands and feet, which affects 0.5% to 1.0% of the population worldwide. With the sustained development of disease-modifying antirheumatic drugs (DMARDs), significant success has been achieved for preventing and relieving disease activity in RA patients. Unfortunately, some patients still show limited response to DMARDs, which puts forward new requirements for special targets and novel therapies. Understanding the pathogenetic roles of the various molecules in RA could facilitate discovery of potential therapeutic targets and approaches. In this review, both Edited by: existing and emerging targets, including the proteins, small molecular metabolites, and Trine N. Jorgensen, epigenetic regulators related to RA, are discussed, with a focus on the mechanisms that Case Western Reserve University, result in inflammation and the development of new drugs for blocking the various United States modulators in RA. Reviewed by: Åsa Andersson, Keywords: rheumatoid arthritis, targets, proteins, small molecular metabolites, epigenetic regulators Halmstad University, Sweden Abdurrahman Tufan, Gazi University, Turkey *Correspondence: INTRODUCTION Chao Liang [email protected] Rheumatoid arthritis (RA) is classified as a systemic poly-articular chronic autoimmune joint † disease that primarily affects hands and feet. -

Looking for Therapeutic Antibodies in Next Generation Sequencing Repositories
bioRxiv preprint doi: https://doi.org/10.1101/572958; this version posted March 10, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Title: Looking for Therapeutic Antibodies in Next Generation Sequencing Repositories. Authors: Konrad Krawczyk1*, Matthew Raybould2, Aleksandr Kovaltsuk2, Charlotte M. Deane2 1 NaturalAntibody, Hamburg, Germany 2 Oxford University Department of Statistics, Oxford, UK *Correspondence to [email protected] Abstract: Recently it has become possible to query the great diversity of natural antibody repertoires using Next Generation Sequencing (NGS). These methods are capable of producing millions of sequences in a single experiment. Here we compare Clinical Stage Therapeutic antibodies to the ~1b sequences from 60 independent sequencing studies in the Observed Antibody Space Database. Of the 242 post Phase I antibodies, we find 16 with sequence identity matches of 95% or better for both heavy and light chains. There are also 54 perfect matches to therapeutic CDR-H3 regions in the NGS outputs, suggesting a nontrivial amount of convergence between naturally observed sequences and those developed artificially. This has potential implications for both the discovery of antibody therapeutics and the legal protection of commercial antibodies. Introduction Antibodies are proteins in jawed vertebrates that recognize noxious molecules (antigens) for elimination. An organism expresses millions of diverse antibodies to increase the chances that some of them will be able to bind the foreign antigen, initiating the adaptive immune response. -

Modifications to the Harmonized Tariff Schedule of the United States To
U.S. International Trade Commission COMMISSIONERS Shara L. Aranoff, Chairman Daniel R. Pearson, Vice Chairman Deanna Tanner Okun Charlotte R. Lane Irving A. Williamson Dean A. Pinkert Address all communications to Secretary to the Commission United States International Trade Commission Washington, DC 20436 U.S. International Trade Commission Washington, DC 20436 www.usitc.gov Modifications to the Harmonized Tariff Schedule of the United States to Implement the Dominican Republic- Central America-United States Free Trade Agreement With Respect to Costa Rica Publication 4038 December 2008 (This page is intentionally blank) Pursuant to the letter of request from the United States Trade Representative of December 18, 2008, set forth in the Appendix hereto, and pursuant to section 1207(a) of the Omnibus Trade and Competitiveness Act, the Commission is publishing the following modifications to the Harmonized Tariff Schedule of the United States (HTS) to implement the Dominican Republic- Central America-United States Free Trade Agreement, as approved in the Dominican Republic-Central America- United States Free Trade Agreement Implementation Act, with respect to Costa Rica. (This page is intentionally blank) Annex I Effective with respect to goods that are entered, or withdrawn from warehouse for consumption, on or after January 1, 2009, the Harmonized Tariff Schedule of the United States (HTS) is modified as provided herein, with bracketed matter included to assist in the understanding of proclaimed modifications. The following supersedes matter now in the HTS. (1). General note 4 is modified as follows: (a). by deleting from subdivision (a) the following country from the enumeration of independent beneficiary developing countries: Costa Rica (b). -
![Insulin Is Necessary but Not Sufficient: Changing the Therapeutic Paradigm in Type 1 Diabetes [Version 1; Peer Review: 5 Approved] Sandra Lord , Carla J](https://docslib.b-cdn.net/cover/5644/insulin-is-necessary-but-not-sufficient-changing-the-therapeutic-paradigm-in-type-1-diabetes-version-1-peer-review-5-approved-sandra-lord-carla-j-1015644.webp)
Insulin Is Necessary but Not Sufficient: Changing the Therapeutic Paradigm in Type 1 Diabetes [Version 1; Peer Review: 5 Approved] Sandra Lord , Carla J
F1000Research 2020, 9(Faculty Rev):827 Last updated: 30 JUL 2020 REVIEW Insulin is necessary but not sufficient: changing the therapeutic paradigm in type 1 diabetes [version 1; peer review: 5 approved] Sandra Lord , Carla J. Greenbaum Benaroya Research Institute at Virginia Mason, Seattle, WA, 98101, USA First published: 30 Jul 2020, 9(Faculty Rev):827 Open Peer Review v1 https://doi.org/10.12688/f1000research.21801.1 Latest published: 30 Jul 2020, 9(Faculty Rev):827 https://doi.org/10.12688/f1000research.21801.1 Reviewer Status Abstract Invited Reviewers Despite the clear evidence that type 1 diabetes (T1D) begins well before 1 2 3 4 5 hyperglycemia is evident, there are no clinically available disease-modifying therapies for early-stage disease. However, following the exciting results of version 1 the Teplizumab Prevention Study, the first study to demonstrate that overt 30 Jul 2020 T1D can be delayed with immunotherapy, there is renewed optimism that in the future, T1D will be treated before hyperglycemia develops. A different treatment paradigm is needed, as a majority of people with T1D do not meet the glycemic targets that are associated with a lower risk of T1D Faculty Reviews are review articles written by the complications and therefore remain vulnerable to complications and prestigious Members of Faculty Opinions. The shortened life expectancy. The following review will outline the history and articles are commissioned and peer reviewed before current status of immunotherapy for T1D and highlight some challenges publication to ensure that the final, published version and ideas for the future. Although such efforts have been worldwide, we will focus particularly on the activities of Diabetes TrialNet, a National Institutes is comprehensive and accessible. -

Modulating Igg Effector Function by FC Engineering and Glycoengineering Andy Racher † & Olga Obrezanova ‡
Modulating IgG effector function by FC engineering and glycoengineering Andy Racher † & Olga Obrezanova ‡ Lonza Biologics, 228 Bath Road, Slough, Berkshire, SL1 4DX, UK † Corresponding author: [email protected] ‡ Current address: AstraZeneca, Cambridge, UK 2 Summary several Fc engineered and glycoengineered antibodies in late stage clinical trials. Several proprietary technologies were Antibodies are the fastest growing group of biotherapeutics. In developed for glycoengineering of monoclonal antibodies early 2020 more than 100 antibody-based molecules, including including Potelligent® technology (KHK / BioWa), GlycoMAb® biosimilars, had been approved globally. Oncology and (GlycArt / Roche), EMABLing® (LFB), GlycoExpress™ (Glycotope) inflammatory disorders remain the major therapeutic areas for and GlymaxX® (ProBioGen). antibody-based molecules but there is a growing interest in using mAbs for treating infectious disease. During the last 10 Encouraging clinical results and prospects in multiple disease years antibody engineering focussed on development of “fit- areas make it likely that more Fc engineered and for-purpose” antibodies with modulated effector functions glycoengineered antibodies will enter clinical trials and such as increased or muted antibody-dependent cell-mediated subsequently be approved. According to market research cytotoxicity (ADCC), antibody-dependent cellular phagocytosis studies, the glycoengineered antibodies are likely to emerge as (ADCP), complement dependent cytotoxicity (CDC), and to the forerunner in the short term (84% of the market share by increase half-life. This paper summarises approaches for 2021) and, subsequently, the Fc protein engineered antibodies modulating antibody effector functions and pharmacokinetics, are likely to gain a higher proportion (55% by 2026). and provides examples of antibodies in clinical studies Glycoengineering strategies focussing on enhancing ADCC employing such approaches.