(FY) 2020 ICD-10-CM Official Guidelines for Coding and Reporting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Section “F” – Para Athletes Championship Competition
Section “F” – Para Athletes Championship Competition These rules are to be read in conjunction with Section ”A" Competition General Rules, Section “B” – Track Events and Section “C” – Field Events. 1. Para Athletes 1.1 General Conditions i. Athletes with a disability qualifying in any able body event at the State Track & Field Championships will not be allowed to compete in the equivalent Para event conducted on the same program. ii. Implements shall comply with the specifications as defined by LANSW for Para events. iii. In Para field events only three trials will be allowed. iv. All LANSW and IAAF (where applicable) rules of competition shall apply except in the following instances. 1.2 Classification i. Athletes with a disability have to be formerly classified by a recognised organisation, prior to competing at the State Track & Field Championships. ii. Classification is a way of grouping athletes of similar function or ability for the purpose of competition. 1.3 Competition i. All events will be conducted as multi-disability events. Competitors will compete against a multi- disability standard (MDS) as determined by the Australian Paralympic Committee. Placings will be determined by the competitor’s time/distance calculated against a percentage of the multi-disability standard (MDS). ii. In all competitions involving throwing events athletes must use the implement weight specified for their classification/ age group, (refer Para Athletes Implement Specification Table). Note: At competition events where combined age group are conducted the competitor’s will throw the weight specified for their age group. This could result in different weight implements being used in the same event. -

Athletics Classification Rules and Regulations 2
IPC ATHLETICS International Paralympic Committee Athletics Classifi cation Rules and Regulations January 2016 O cial IPC Athletics Partner www.paralympic.org/athleticswww.ipc-athletics.org @IPCAthletics ParalympicSport.TV /IPCAthletics Recognition Page IPC Athletics.indd 1 11/12/2013 10:12:43 Purpose and Organisation of these Rules ................................................................................. 4 Purpose ............................................................................................................................... 4 Organisation ........................................................................................................................ 4 1 Article One - Scope and Application .................................................................................. 6 International Classification ................................................................................................... 6 Interpretation, Commencement and Amendment ................................................................. 6 2 Article Two – Classification Personnel .............................................................................. 8 Classification Personnel ....................................................................................................... 8 Classifier Competencies, Qualifications and Responsibilities ................................................ 9 3 Article Three - Classification Panels ................................................................................ 11 4 Article Four -

Classification Report
World Para Athletics Classification Master List Summer Season 2017 Classification Report created by IPC Sport Data Management System Sport: Athletics | Season: Summer Season 2017 | Region: Oceania Region | NPC: Australia | Found Athletes: 114 Australia SDMS ID Family Name Given Name Gender Birth T Status F Status P Status Reason MASH 14982 Anderson Rae W 1997 T37 R F37 R-2024 10627 Arkley Natheniel M 1994 T54 C 33205 Ault-Connell Eliza W 1981 T54 C 1756 Ballard Angela W 1982 T53 C 26871 Barty Chris M 1988 T35 R F34 R MRR 1778 Beattie Carlee W 1982 T47 C F46 C 26763 Bertalli James M 1998 T37 R F37 R 17624 Blake Torita W 1995 T38 R-2022 32691 Bounty Daniel M 2001 T38 R-2022 13801 Burrows Thomas M 1990 T20 [TaR] R 29097 Byrt Eliesha W 1988 T20 [TaR] C 32689 Carr Blake M 1994 T20 [HozJ] C F20 N 10538 Carter Samuel M 1991 T54 C 1882 Cartwright Kelly W 1989 T63 C F63 C 29947 Charlton Julie W 1999 T54 C F57 C 1899 Chatman Aaron M 1987 T47 C 29944 Christiansen Mitchell M 1997 T37 R-2025 26224 Cleaver Erin W 2000 T38 R-2022 19971 Clifford Jaryd M 1999 T12 R-2023 F12 R-2023 29945 Colley Tamsin W 2002 T36 R-2023 F36 R-2020 1941 Colman Richard M 1984 T53 C 26990 Coop Brianna W 1998 T35 R-2022 19721 Copas Stacey W 1978 T51 R F52 C 32680 Crees Dayna W 2002 F34 R-2022 29973 Crombie Cameron M 1986 F38 R-2022 19964 Cronje Jessica W 1998 T37 R F37 R IPC Sport Data Management System Page 1 of 4 6 October 2021 at 07:08:42 CEST World Para Athletics Classification Master List Summer Season 2017 19546 Davidson Brayden M 1997 T36 R-2022 1978 Dawes Christie W -

TSM Proficiency Testing Statistical Summary
ANDREW M. CUOMO HOWARD A. ZUCKER, M.D., J.D. SALLY DRESLIN, M.S., R.N. Governor Commissioner Executive Deputy Commissioner Therapeutic Substance Monitoring/Quantitative Toxicology Proficiency Test Program Statistical Summary - August 2016 (Event 16-3) This statistical report summarizes participant data for the five Therapeutic Substance Monitoring proficiency survey specimens shipped 29 August 2016. Test samples (Vials T36, T37, T38, T39, T40) were prepared by the quantitative transfer of constituents to pooled human serum. The material was subsequently sterile filtered, dispensed into aliquots, stored at -80oC, and distributed to participants for analysis. Results for individual instrument and reagent systems where the number of laboratories using those systems is three or greater are provided. Mean and Standard Deviation (± 1 SD) values are calculated by a robust statistical technique that does not assume a Gaussian distribution. Disclaimer: Note: The use of brand and/or trade names in this report does not constitute an endorsement of the products on the part of the Wadsworth Center or the New York State Department of Health Should you have any questions regarding this report, please contact the Therapeutic Substance Monitoring Section at (518) 474-0005. Empire State Plaza, Corning Tower, Albany, NY 12237 │ health.ny.gov New York State Department of Health – Wadsworth Center Therapeutic Substance Monitoring Proficiency Testing – August 29, 2016 Summary of Participant Performance (Mean and Standard Deviation) Acetaminophen (mg/L) Specimen: -

(VA) Veteran Monthly Assistance Allowance for Disabled Veterans
Revised May 23, 2019 U.S. Department of Veterans Affairs (VA) Veteran Monthly Assistance Allowance for Disabled Veterans Training in Paralympic and Olympic Sports Program (VMAA) In partnership with the United States Olympic Committee and other Olympic and Paralympic entities within the United States, VA supports eligible service and non-service-connected military Veterans in their efforts to represent the USA at the Paralympic Games, Olympic Games and other international sport competitions. The VA Office of National Veterans Sports Programs & Special Events provides a monthly assistance allowance for disabled Veterans training in Paralympic sports, as well as certain disabled Veterans selected for or competing with the national Olympic Team, as authorized by 38 U.S.C. 322(d) and Section 703 of the Veterans’ Benefits Improvement Act of 2008. Through the program, VA will pay a monthly allowance to a Veteran with either a service-connected or non-service-connected disability if the Veteran meets the minimum military standards or higher (i.e. Emerging Athlete or National Team) in his or her respective Paralympic sport at a recognized competition. In addition to making the VMAA standard, an athlete must also be nationally or internationally classified by his or her respective Paralympic sport federation as eligible for Paralympic competition. VA will also pay a monthly allowance to a Veteran with a service-connected disability rated 30 percent or greater by VA who is selected for a national Olympic Team for any month in which the Veteran is competing in any event sanctioned by the National Governing Bodies of the Olympic Sport in the United State, in accordance with P.L. -
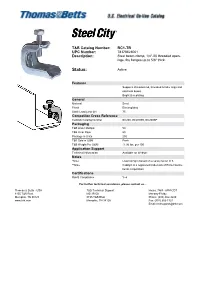
Status: Active
T&B Catalog Number: BC1-TB UPC Number: 78378623001 Description: Steel beam clamp, 1/4"-20 threaded open- ings, fits flanges up to 5/8" thick. Status: Active Features Supports threaded rod, threaded brindle rings and electrical boxes. Bright zinc plating. General Material Steel Finish Electroplated Static Load Limit (lb) 75 Competitor Cross Reference Caddy® Catalog Number BC200, BC200SS, BC200BP Packaging T&B Order Multiple 50 T&B Inner Pack 50 Package in Units 250 T&B Sold in UOM Each T&B Weight Per UOM 11.96 lbs. per 100 Application Support Technical Information Available on Website Notes *Note Load rating is based on a safety factor of 3. **Note Caddy® is a registered trademark of Erico Interna- tional Corporation Certifications RoHS Compliance Yes For further technical assistance, please contact us... Thomas & Betts - USA T&B Technical Support Hours: 7AM - 6PM CDT 8155 T&B Blvd. MS 3B-50 Monday-Friday Memphis, TN 38125 8155 T&B Blvd. Phone: (888) 862-3289 www.tnb.com Memphis, TN 38125 Fax: (901) 252-1321 Email:[email protected] Form 7, Form 8, and red•dot® Conduit Outlet Bodies C Form 7 Dimensions (in.) Cat. No. Size A B C D E CI C17 d 5.45 1.40 1.45 .95 3.20 4.0 C27 f 6.05 1.60 1.65 1.15 3.80 6.6 1 6.75 1.90 1.80 1.35 4.55 10.6 D C C37 C47 1b 7.30 2.30 2.20 1.80 5.00 18.8 C57 1d 8.60 2.60 2.45 2.05 5.45 26.4 C67 2 9.50 3.20 3.05 2.45 6.40 51.0 E C77-TB 2d 12.10 3.65 4.25 3.60 8.40 102.0 C87 3 12.10 4.40 4.25 3.60 8.40 132.0 B ® ® A C Form 8 Dimensions (in.) C Form 7 and Form 8 Cat. -

English Federation of Disability Sport National Junior Athletics Information and Standards
English Federation of Disability Sport National Junior Athletics Information and standards 1 Contents Introduction 3 EFDS track groupings 4 EFDS field groupings 5 Events available 6 National field weights 8 National standards track 11 National standard field 13 2 Introduction This booklet has been produced with the intention of enabling athletes, coaches, teachers and parents to compare EFDS Profiles and Athletics Groupings with IPC Athletics Classes, the enclosed information is a guide for EFDS Events and IS NOT AN IPC CLASSIFICATION. You can find out further information on classification using the following links: www.englandathletics.org/disability-athletics/eligibility-and-classification UK Classification will allow athletes to: - Enter Parallel Success events across UK - Register times on the UK Rankings (www.thepowerof10.info) - Be eligible for Sainsbury’s School Games selection - Receive monthly Paralympic newsletter from British Athletics For athletes interested in joining an athletics club and seeking a UK Classification please contact. - Shelley Holroyd (England North & East) [email protected] - Job King (England Midlands & South) [email protected] Or complete the following online form. www.englandathletics.org/parallelsuccess The document contains information regarding the events available to athletes, the specific weights for throwing implements relevant to the EFDS Field and Age Groups as well as the qualifying standards for the National Junior Athletics Championships. Our aim is to provide as much information and support as possible so that athletes, regardless of their ability can continue to participate within the sport of athletics. We are committed to delivering multi- disability events that cater for both the needs of the disability community and the relevant NGB pathway for talented athletes. -

Tokyo 2020 Paralympic Games Qualification Regulations
Tokyo 2020 Paralympic Games Qualification Regulations August 2019 International Paralympic Committee Adenauerallee 212-214 Tel. +49 228 2097-200 www.paralympic.org 53113 Bonn, Germany Fax +49 228 2097-209 [email protected] CONTENTS 1. Introduction 2. Tokyo 2020 Paralympic Games Programme Overview 3. General IPC Regulations on Eligibility 4. IPC Redistribution Policy of Vacant Qualification Slots 5. Universality Wild Cards 6. Key Dates 7. Archery 8. Athletics 9. Badminton 10. Boccia 11. Canoe 12. Cycling (Track and Road) 13. Equestrian 14. Football 5-a-side 15. Goalball 16. Judo 17. Powerlifting 18. Rowing 19. Shooting 20. Swimming 21. Table Tennis 22. Taekwondo 23. Triathlon 24. Volleyball (Sitting) 25. Wheelchair Basketball 26. Wheelchair Fencing 27. Wheelchair Rugby 28. Wheelchair Tennis 29. Glossary 30. Register of Updates Tokyo 2020 Paralympic Games – Qualification Regulations 2 INTRODUCTION These Qualification Regulations (Regulations) describe in detail how athletes and teams can qualify for the Tokyo 2020 Paralympic Games in each of the twenty-two (22) sports on the Tokyo 2020 Paralympic Games Programme (Games Programme). It provides to the National Paralympic Committees (NPCs), to National Federations (NFs), to sports administrators, coaches and to the athletes themselves the conditions that allow participation in the signature event of the Paralympic Movement. These Regulations present: . an overview of the Games Programme; . the general IPC regulations on eligibility; . the specific qualification criteria for each sport (in alphabetical order); and . a glossary of the terminology used throughout the Regulations. Structure of sport-specific qualification criteria Each sport-specific section in these Regulations follows a standardised format. Readers can quickly locate information or cross-reference it between sports. -

Towards Evidence-Based Classification for Paralympic
TOWARDSEVIDENCE-BASEDCLASSIFICATIONFORPARALYMPIC RUNNINGANDTHROWINGEVENTS jemima grace spathis A thesis submitted for the degree of Doctor of Philosophy at The University of Queensland in 2015 School of Human Movement and Nutrition Sciences ABSTRACT Classification in Paralympic athletics aims to promote participation by people with disabili- ties by minimising the impact of impairment on the outcome of competition. Achieving this aim will ensure successful athletes are those who have the most favourable physiological, anthropometric and psychological attributes and not simply those who are less impaired than their competitors. The aim of this program of research is to make a scientific con- tribution to the development of evidence-based methods of classification for Paralympic running and throwing events. Section 1 describes the key concepts of Paralympic classification. Evidence-based meth- ods of classification require research that evaluates the relative strength of association be- tween valid measures of the impairment performance. A valid measure of impairment requires several measurement properties, one being that it should be resistant to training. Unfortunately it is likely that available measures of impaired strength and coordination will improve in response to athletic training, creating the possibility that well-trained athletes may improve their impairment profile and subsequently be competitively disadvantaged by being placed into a class with athletes with less severe impairments than themselves. Therefore a second research requirement for evidence-based methods of classification is the development of tests that will permit classifiers to determine the extent to which an athlete may have positively influenced their impairment profile through athletic training. These are referred to as Training Assessment Tests (TAT) which should be highly responsive to training and have a significant relationship to performance. -

931 Brain Imaging CPT, HCPCS and Diagnoses Codes
Medical Policy Brain Imaging CPT, HCPCS and Diagnoses Codes Policy Number: 931 BCBSA Reference Number: N/A NCD/LCD: N/A Related Policies • Medicare Advantage: Advanced Imaging/Radiology and Sleep Disorder Management Clinical and Utilization Guidance Redirect, #923 • Advanced Imaging/Radiology CPT and HCPCS Codes, #900 • Advanced Imaging/Radiology, #968 • Oncologic Imaging CPT, HCPCS and Diagnoses Codes, #929 • Abdomen and Pelvic Imaging CPT, HCPCS and Diagnoses Codes, #930 • Chest Imaging CPT, HCPCS and Diagnoses Codes, #932 • Extremity Imaging CPT, HCPCS and Diagnoses Codes, #933 • Head and Neck Imaging CPT, HCPCS and Diagnoses Codes, #934 • Spine Imaging CPT, HCPCS and Diagnoses Codes, #935 • Vascular Imaging CPT, HCPCS and Diagnoses Codes, #936 Table of Contents Commercial Products .................................................................................................................................... 1 Medicare Advantage Products ...................................................................................................................... 2 CPT Codes / HCPCS Codes / ICD Codes .................................................................................................... 2 CPT Codes: 70450, 70460, 70470 CT head/brain ....................................................................................... 2 CPT codes: 70551, 70552, 70553 MRI brain............................................................................................ 115 CPT codes: 70554, 70555 MRI brain functional ...................................................................................... -

1/24 Eliminations / 2020-08-03 Archery Yumenoshima Park Archery Field 2021-08-28 09:00 14:55 Changed the Time from "14:00" to "14:55"
Competition Schedule: The Event Line-up for Each Session of the Tokyo 2020 Paralympic Games change log Change date SPORT(DISCIPLINE) VENUE DATE START TIME END TIME EVENT Change log Men's Individual Compound Open: 1/24 Eliminations / 2020-08-03 Archery Yumenoshima Park Archery Field 2021-08-28 09:00 14:55 Changed the time from "14:00" to "14:55". Men's Individual Compound Open: 1/16 Eliminations Mixed Team W1: 1/8 Eliminations / Mixed Team W1: Quarterfinals / Mixed Team W1: Semifinals / Changed the time from "17:00-21:25" to "17:30- 2020-08-03 Archery Yumenoshima Park Archery Field 2021-08-28 17:30 21:55 Mixed Team W1: Bronze Medal Match / 21:55". Mixed Team W1: Gold Medal Match / Mixed Team W1: Victory Ceremony Women's Individual Compound Open: 1/16 Eliminations / 2020-08-03 Archery Yumenoshima Park Archery Field 2021-08-29 09:00 14:10 Changed the time from "13:55" to "14:10". Mixed Team Compound Open: 1/8 Eliminations Mixed Team Compound Open: Quarterfinals / Mixed Team Compound Open: Semifinals / Changed the time from "17:00-21:25" to "17:30- 2020-08-03 Archery Yumenoshima Park Archery Field 2021-08-29 17:30 20:35 Mixed Team Compound Open: Bronze Medal Match / 20:35". Mixed Team Compound Open: Gold Medal Match / Mixed Team Compound Open: Victory Ceremony Women's Individual Compound Open: 1/8 Eliminations / Women's Individual Compound Open: Quarterfinals / Women's Individual Compound Open: Semifinals / 2020-08-03 Archery Yumenoshima Park Archery Field 2021-08-30 09:00 14:15 Changed the time from "13:25" to "14:15". -
2018 Multi-Class Athletes Competition Handbook
LAQ Multi-Class Athletes Competition Handbook July 2018 LAQ Multi-Class Athletes - Competition Handbook Introduction In 2013, classified Multi-Class (athletes with disabilities) were endorsed to compete in limited events under their own classification at Little Athletics Queensland conducted competitions up to State-level, as determine by the Competition Committee. The following rules are to be read in conjunction the LAQ Competition Handbook. Where applicable, all LAQ and IAAF rules of competition shall apply unless specified in this document. The Association recognises that events as detailed in this handbook may not be offered at weekly Centre meets. However, wherever feasible and appropriate the conditions and rules detailed in this handbook should be adhered to. Centre Committees may offer additional modified events not detailed in this handbook provided the event / equipment specifications are not greater than those detailed in the LAQ Competition Handbook and the Implement Weights for Para athletics “Open & Underage” athletes with a Disability document. Rules and events pertaining to the Multi-Class athletes at LAQ competitions will be reviewed every two years. July 2018 LAQ Multi-Class Athletes - Competition Handbook 1. CLASSIFICATION 1.1. Classification is a way of grouping athletes of similar function or ability for the purpose of competition. 1.2. Athletes with a disability have to be formerly classified by a recognised organisation, prior to competing in LAQ Carnivals and the Winter, Regional and State Championships i. Intellectual Impairment (T/F 20) - through Sports Inclusion Australia (previously AUSRAPID) or Australian Paralympic Committee ii. Physical Impairment (T/F 31-38, 40-47, 51-57) - through Athletics Australia – Provisional PI is acceptable for Regional and Carnival competitions iii.