Assessing the Efficacy and Safety of Eravacycline Vs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Antibacterial Efficacy of Eravacycline in Vivo Against Gram-Positive And
crossmark Antibacterial Efficacy of Eravacycline In Vivo against Gram-Positive and Gram-Negative Organisms Marguerite L. Monogue,a Abrar K. Thabit,a,b Yukihiro Hamada,a,c David P. Nicolaua,d Center for Anti-Infective Research and Development, Hartford Hospital, Hartford, Connecticut, USAa; Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabiab; Aichi Medical University Hospital School of Medicine, Aichi, Japanc; Division of Infectious Diseases, Hartford Hospital, Hartford, Connecticut, USAd Members of the tetracycline class are frequently classified as bacteriostatic. However, recent findings have demonstrated an im- > proved antibacterial killing profile, often achieving 3 log10 bacterial count reduction, when such antibiotics have been given for periods longer than 24 h. We aimed to study this effect with eravacycline, a novel fluorocycline, given in an immunocompetent murine thigh infection model over 72 h against two methicillin-resistant Staphylococcus aureus (MRSA) isolates (eravacycline to 0.25 g/ml). A humanized Downloaded from 0.125 ؍ and 0.25 g/ml) and three Enterobacteriaceae isolates (eravacycline MICs 0.03 ؍ MICs eravacycline regimen, 2.5 mg/kg of body weight given intravenously (i.v.) every 12 h (q12h), demonstrated progressively en- hanced activity over the 72-h study period. A cumulative dose response in which bacterial density was reduced by more than 3 log10 CFU at 72 h was noted over the study period in the two Gram-positive isolates, and eravacycline performed similarly to comparator antibiotics (tigecycline, linezolid, and vancomycin). A cumulative dose response with eravacycline and comparators (tigecycline and meropenem) over the study period was also observed in the Gram-negative isolates, although more variability in bacterial killing was observed for all antibacterial agents. -
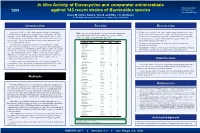
In Vitro Activity of Eravacycline and Comparator Antimicrobials Against
In Vitro Activity of Eravacycline and comparator antimicrobials *Presenting Author: against 143 recent strains of Bacteroides species Diane M. Citron 1209 [email protected] Diane M. Citron, Kerin L. Tyrrell, and Ellie J. C. Goldstein R. M. Alden Research Laboratory, Culver City, CA 90230 Introduction Results Discussion Eravacycline (ERV) is a novel, fully-synthetic fluorocycline antibiotic in Resistance to tetracycline has become common among Bacteroides species and Table 1. In vitro activity (µg/ml) of eravacycline and comparators development for the treatment of serious infections, including those caused by the MIC90 for all of the strains was >32 µg/ml. Eravacycline was four- to eight- multidrug-resistant (MDR) pathogens. ERV recently completed phase 3 clinical against Bacteroides species. All results for the quality control fold more active than tigecycline against these strains with MIC at 1–4 µg/ml. strains were within acceptable CLSI ranges (4). 90 development for the treatment of complicated intra-abdominal infections (cIAI) Eravacycline was active against several strains that showed resistance to and is in phase 3 clinical development for complicated urinary tract infections piperacillin-tazobactam and meropenem. (cUTI), including pyelonephritis. Organism (no.) / Agent Range MIC MIC 50 90 Resistance to clindamycin was also common and all of these strains were ERV has potent activity against a broad range of Gram-positive, Gram- B. caccae (10) Eravacycline 0.25–4 0.5 2 susceptible to eravacycline. negative and anaerobic pathogens. Like other tetracyclines, ERV inhibits protein Tigecycline 0.25–16 4 16 Metronidazole resistance was not encountered in this group of isolates, although, synthesis by binding to the 30S ribosomal subunit. -

Lactamase-Producing Carbapenem-Resistant Enterobacteriaceae (CRE) to Eravacycline
The Journal of Antibiotics (2016) 69, 600–604 & 2016 Japan Antibiotics Research Association All rights reserved 0021-8820/16 www.nature.com/ja ORIGINAL ARTICLE In vitro susceptibility of β-lactamase-producing carbapenem-resistant Enterobacteriaceae (CRE) to eravacycline Yunliang Zhang, Xiaoyan Lin and Karen Bush Eravacycline is a novel, fully synthetic fluorocycline antibiotic of the tetracycline class being developed for the treatment of complicated urinary tract infections and complicated intra-abdominal infections. Eravacycline has activity against many key Gram-negative pathogens, including Enterobacteriaceae resistant to carbapenems, cephalosporins, fluoroquinolones and β-lactam/β-lactamase inhibitor combinations, including strains that are multidrug-resistant. Carbapenem-resistant Enterobacteriaceae (CRE) isolates from 2010 to 2013 (n = 110) were characterized for carbapenemase genes by PCR and sequencing. MICs for eravacycline, tetracycline, tigecycline, amikacin, imipenem, ceftazidime, cefotaxime and levofloxacin were determined in broth microdilution assays. All isolates produced at least one carbapenemase, most frequently KPC-3. Nine isolates produced both a KPC serine carbapenemase and a metallo-β-lactamase, NDM-1 (n = 1) or VIM-1 (n = 8). The 110 isolates were highly resistant to all the β-lactams tested and to levofloxacin, and had MIC50/MIC90 values in the intermediate − 1 − 1 range for tetracycline and amikacin. MIC50/MIC90 values for eravacycline were 1/2 μgml compared with 2/2 μgml for tigecycline. Eravacycline MICs were often twofold lower than for tigecycline, with 64% of the eravacycline MICs o2 μgml− 1 as compared with o4% of tigecycline MICs. Overall, eravacycline demonstrated the lowest cumulative MICs against this panel of recent CRE and may have the potential to treat infections caused by CRE. -

Antibiotics Currently in Clinical Development
A data table from Feb 2018 Antibiotics Currently in Global Clinical Development Note: This data visualization was updated in December 2017 with new data. As of September 2017, approximately 48 new antibiotics1 with the potential to treat serious bacterial infections are in clinical development. The success rate for clinical drug development is low; historical data show that, generally, only 1 in 5 infectious disease products that enter human testing (phase 1 clinical trials) will be approved for patients.* Below is a snapshot of the current antibiotic pipeline, based on publicly available information and informed by external experts. It will be updated periodically, as products advance or are known to drop out of development. Because this list is updated periodically, endnote numbers may not be sequential. In September 2017, the antibiotics pipeline was expanded to include products in development globally. Please contact [email protected] with additions or updates. Expected activity Expected activity against CDC Development against resistant Drug name Company Drug class Target urgent or WHO Potential indication(s)?5 phase2 Gram-negative critical threat ESKAPE pathogens?3 pathogen?4 Approved for: Acute bacterial skin and skin structure infections; other potential Baxdela Approved June 19, Melinta Bacterial type II Fluoroquinolone Possibly No indications: community-acquired bacterial (delafloxacin) 2017 (U.S. FDA) Therapeutics Inc. topoisomerase pneumonia and complicated urinary tract infections6 Approved for: Complicated urinary Rempex tract infections including pyelonephritis; Vabomere Pharmaceuticals β-lactam (carbapenem) other potential indications: complicated Approved Aug. 30, (Meropenem + Inc. (wholly owned + β-lactamase inhibitor PBP; β-lactamase Yes Yes (CRE) intra-abdominal infections, hospital- 2017 (U.S. -
ESAC-Net Reporting Protocol 2019.Docx
TESSy - The European Surveillance System Antimicrobial consumption (AMC) reporting protocol 2019 European Surveillance of Antimicrobial Consumption Network (ESAC-Net) surveillance data for 2018 March 2019 Contents Introduction ............................................................................................................... 4 ESAC-Net ........................................................................................................................... 4 AMC metadata changes 2019 ............................................................................................... 5 Summary of the TESSy AMC data upload and validation process ........................................... 5 Annual ESAC-Net data collection .......................................................................................... 6 Overview of AMC data collection and analysis ....................................................................... 6 How to use this document .................................................................................................... 8 Finding further information .................................................................................................... 8 Reporting to TESSy ................................................................................................... 9 Data collection schedule ....................................................................................................... 9 Preparing data .................................................................................................................... -

Xerava, INN-Eravacycline
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. See section 4.8 for how to report adverse reactions. 1. NAME OF THE MEDICINAL PRODUCT Xerava 50 mg powder for concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each vial contains 50 mg eravacycline. After reconstitution each mL contains 10 mg eravacycline. After further dilution 1 mL contains 0.3 mg eravacycline. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Powder for concentrate for solution for infusion (powder for concentrate). Pale yellow to dark yellow cake. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Xerava is indicated for the treatment of complicated intra-abdominal infections (cIAI) in adults (see sections 4.4 and 5.1). Consideration should be given to official guidance on the appropriate use of antibacterial agents. 4.2 Posology and method of administration Posology The recommended dose regimen is 1 mg/kg eravacycline every 12 hours for 4 to 14 days. Strong CYP3A4 inducers In patients co-administered strong CYP3A4 inducers the recommended dose regimen is 1.5 mg/kg eravacycline every 12 hours for 4 to 14 days (see sections 4.4 and 4.5). Elderly (≥ 65 years old) No dose adjustment is required in elderly patients (see section 5.2). Renal impairment No dose adjustment is necessary in patients with renal impairment or in patients undergoing haemodialysis. Eravacycline may be administered without regard to the timing of haemodialysis (see section 5.2). -

Concept Paper
Concept Paper: Potential Approach for Ranking of Antimicrobial Drugs According to Their Importance in Human Medicine: A Risk Management Tool for Antimicrobial New Animal Drugs Introduction This concept paper discusses a potential approach to considering the human medical importance of antimicrobial drugs when assessing and managing antimicrobial resistance risks associated with the use of antimicrobial drugs in animals. In 2003, FDA established a list ranking antimicrobial drugs according to their relative importance in human medicine primarily for the purpose of supporting a qualitative risk assessment process outlined in agency guidance. It was envisioned by the Agency at the time the current medical importance rankings list was published that it would periodically reassess the rankings to align with contemporary science and current human clinical practices. To that end, this paper describes a potential revised process for ranking antimicrobial drugs according to their relative importance in human medicine, potential revised criteria to determine the medical importance rankings, and the list of antimicrobial drug medical importance rankings that would result if those criteria were to be used. Disclaimer: This concept paper is for discussion purposes only. The intent of this concept paper is to obtain public comment and early input on a potential approach to consider the human medical importance of antimicrobial drugs when assessing and managing antimicrobial resistance risks associated with the use of antimicrobial drugs in animals. This concept paper does not contain recommendations and does not constitute draft or final guidance by the Food and Drug Administration. It should not be used for any purpose other than to facilitate public comment. -

Double Anaerobic Coverage: Role in Clinical Practice Clinical Guideline BACKGROUND
March 2019 Double Anaerobic Coverage: Role in Clinical Practice Clinical Guideline BACKGROUND Anaerobic pathogens are normal flora of the oral cavity and the gastrointestinal tract. While oral anaerobic flora are mostly gram-positive organisms such as Peptococcus and Peptostreptococcus spp., the principal anaerobic intestinal flora are gram-negative bacilli such as Bacteroides fragilis, Prevotella melaninogenica, and Fusobacterium spp. Gram-positive oral anaerobes are widely covered by most of the orally-available agents, including penicillin. However, antibiotic activity against the most common intestinal anaerobic bacteria, Bacteroides spp., is variable. Anaerobic coverage is indicated in a variety of infectious processes, including but not limited to aspiration pneumonia, intra-abdominal infection, gynecologic infection, and diabetic foot ulcer infection. Antimicrobial agents with appreciable anaerobic activity include the following: Amoxicillin/clavulanate Meropenem Ampicillin/sulbactam Metronidazole Cefotetan Moxifloxacin Cefoxitin Piperacillin/tazobactam Clindamycin Eravacycline Ertapenem Tigecycline Imipenem Omadacycline Available treatment guidelines published by the Infectious Diseases Society of America (IDSA) do not recommend the use of double anaerobic coverage in the above mentioned indications. CLINICAL SYNDROMES Aspiration Pneumonia Aspiration pneumonia and pneumonitis are common clinical syndromes. In the case of aspiration pneumonia, oral gram-positive anaerobic flora and gram-negative enteric bacteria are the pathogens -

Using Saccharomyces Cerevisiae for the Biosynthesis of Tetracycline Antibiotics
Using Saccharomyces cerevisiae for the Biosynthesis of Tetracycline Antibiotics Ehud Herbst Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2019 © 2019 Ehud Herbst All rights reserved ABSTRACT Using Saccharomyces cerevisiae for the biosynthesis of tetracycline antibiotics Ehud Herbst Developing treatments for antibiotic resistant bacterial infections is among the most urgent public health challenges worldwide. Tetracyclines are one of the most important classes of antibiotics, but like other antibiotics classes, have fallen prey to antibiotic resistance. Key small changes in the tetracycline structure can lead to major and distinct pharmaceutically essential improvements. Thus, the development of new synthetic capabilities has repeatedly been the enabling tool for powerful new tetracyclines that combatted tetracycline-resistance. Traditionally, tetracycline antibiotics were accessed through bacterial natural products or semisynthetic analogs derived from these products or their intermediates. More recently, total synthesis provided an additional route as well. Importantly however, key promising antibiotic candidates remained inaccessible through existing synthetic approaches. Heterologous biosynthesis is tackling the production of medicinally important and structurally intriguing natural products and their unnatural analogs in tractable hosts such as Saccharomyces cerevisiae. Recently, the heterologous biosynthesis of several tetracyclines was achieved in Streptomyces lividans through the expression of their respective biosynthetic pathways. In addition, the heterologous biosynthesis of fungal anhydrotetracyclines was shown in S. cerevisiae. This dissertation describes the use of Saccharomyces cerevisiae towards the biosynthesis of target tetracyclines that have promising prospects as antibiotics based on the established structure- activity relationship of tetracyclines but have been previously synthetically inaccessible. -

Visão De Futuro Para Produção De Antibióticos: Tendências De Pesquisa, Desenvolvimento E Inovação
UNIVERSIDADE FEDERAL DO RIO DE JANEIRO CRISTINA D’URSO DE SOUZA MENDES SANTOS VISÃO DE FUTURO PARA PRODUÇÃO DE ANTIBIÓTICOS: TENDÊNCIAS DE PESQUISA, DESENVOLVIMENTO E INOVAÇÃO Rio de Janeiro EQ/UFRJ 2014 CRISTINA D ’U RSO DE SOUZA MENDES SANTOS VISÃO DE FUTURO PARA A PRODUÇÃO DE ANTIBIÓTICOS: TENDÊNCIAS DE PESQUISA, DESENVOLVIMENTO E INOVAÇÃO Tese de Doutorado apresentada ao Programa de Pós-Graduação em Tecnologia de Processos Químicos e Bioquímicos, Escola de Química, Universidade Federal do Rio de Janeiro, como requisito parcial à obtenção do título de Doutor em Ciências, D.Sc. Orientadora: Profa. Adelaide Maria de Souza Antunes, D.Sc. Rio de Janeiro 2014 Santos, Cristina d’Urso de Souza Mendes. Visão de futuro para produção de antibióticos: tendências de pesquisa, desenvolvimento e inovação / Cristina d’Urso de Souza Mendes Santos. - Rio de Janeiro, 2014. 216 f.: il.; 29,7 cm. Tese (Doutorado em Ciências) – Universidade Federal do Rio de Janeiro, Escola de Química, Programa de Pós-Graduação em Tecnologia de Processos Químicos e Bioquímicos, Rio de Janeiro, 2014. Orientadora: Adelaide Maria de Souza Antunes. 1. Antibióticos. 2. P&D na Indústria Farmacêutica. 3. Prospecção Tecnológica. 4. Patentes. I. Antunes, Adelaide Maria de Souza. II. Universidade Federal do Rio de Janeiro. Escola de Química. III. Visão de futuro para a produção de antibióticos: tendências de pesquisa, desenvolvimento e inovação. iv v Dedico esta tese à minha mãe querida e amada, que está no céu comemorando esta vitória, que é mais dela do que minha. Dedico também à minha filhinha Malu que sem entender foi a minha maior motivação para concluir esta tese. -

What's Hot in Infectious Diseases
What’s Hot in Infectious Diseases - Clinical Science? Stan Deresinski MD FACP FIDSA Clinical Professor of Medicine Stanford University No Disclosures 1884 Pakistan: Salmonella enterica serovar typhi MDR - XDR • November 2016, Hyderabad Pakistan Integrated transposon • Appearance of a H58 haplotype strain encoding amp, chloro, resistant to antibiotics of 5 classes T/S resistance + gyrA • Resulted from acquisition of single mutation chromosomal and plasmid mediated mechanisms by dominant H58 haplotype IncY plasmid* • Plasmid carrying qnrS, blaCTX-M-15 acquired from E. coli blaCTXM-15 • Susceptible only to imipenem, qnrS azithromycin MDR – chloramphenicolR, T/SR, ampicillinR XDR – MDR plus ceftriaxoneR, fluoroquinoloneR mBio. January/February 2018 Volume 9 Issue 1 e00105-18 XDR Typhoid – Pakistan & Beyond • Rapid increase in case numbers with spread to Karachi WHO prequalified use of conjugate vaccine (Typbar-TCV®) – single dose, immunogenic in children >6 months of age • At least 3 travelers returned with infection - one to UK, 2 to US July 11, 2018 “Novartis joins the Big Pharma exodus out of antibiotics, dumping research, cutting 140 and out-licensing programs” https://endpts.com/novartis-joins-the-big-pharma-exodus-out-of-antibiotics-dumping-research-cutting-140-and-out-licensing-programs/ https://gizmodo.com/novartis-becomes-the-latest-pharma-company-to-give-up-o-1827524081 Selected Antibacterials Expected to Be Submitted to the FDA for Approval by Mid-2019 https://cdn2.hubspot.net/hubfs/498900/Jul2018_DrugPriceForecast_Media_FINAL.pdf Cefiderocol • Siderophore cephalosporin • Panel (N=315) of carbapenemase- producing MDR GNR – MIC <4 mcg/ml: • Enterobacteriaeceae – 87.5% • P. aeruginosa - 100% • A. baumanii - 89% • Activity by carbapenemase type: • A – 91.8% B - 74.8% D – 98.0% IDWeek 2017. -

Antibiotics Against Multidrug-Resistant Gram-Negative Bacteria
Journal of Clinical Medicine Review An Update on Eight “New” Antibiotics against Multidrug-Resistant Gram-Negative Bacteria Erlangga Yusuf * , Hannelore I. Bax, Nelianne J. Verkaik and Mireille van Westreenen Department of Medical Microbiology and Infectious Diseases, Erasmus University Medical Center, 3015 GD Rotterdam, The Netherlands; [email protected] (H.I.B.); [email protected] (N.J.V.); [email protected] (M.v.W.) * Correspondence: [email protected] Abstract: Infections in the ICU are often caused by Gram-negative bacteria. When these microorgan- isms are resistant to third-generation cephalosporines (due to extended-spectrum (ESBL) or AmpC beta-lactamases) or to carbapenems (for example carbapenem producing Enterobacteriales (CPE)), the treatment options become limited. In the last six years, fortunately, there have been new an- tibiotics approved by the U.S. Food and Drug Administration (FDA) with predominant activities against Gram-negative bacteria. We aimed to review these antibiotics: plazomicin, eravacycline, temocillin, cefiderocol, ceftazidime/avibactam, ceftolozane/tazobactam, meropenem/vaborbactam, and imipenem/relebactam. Temocillin is an antibiotic that was only approved in Belgium and the UK several decades ago. We reviewed the in vitro activities of these new antibiotics, especially against ESBL and CPE microorganisms, potential side effects, and clinical studies in complicated urinary tract infections (cUTI), intra-abdominal infections (cIAI), and hospital-acquired pneumonia/ventilator- associatedpneumonia (HAP/VAP). All of these new antibiotics are active against ESBL, and almost all of them are active against CPE caused by KPC beta-lactamase, but only some of them are active against CPE due to MBL or OXA beta-lactamases.