The Potential Dangers of Shield Booster Seats
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Accidental Injuries Caused by Automotive Frontal Collision
ORIGINAL ARTICLE Accidental Injuries Caused by Automotive Frontal Collision Karen Viviana Pérez Lujána , Rita de Cassia Silvaa , Alessandro Borges de Souza Oliveiraa , Diego Antonio Legarda Cordobab , Palloma Vieira Muterllea , José Alexander Araújoa , Jorge Luiz de Almeida Ferreiraa , Cosme Roberto Moreira da Silvaa* a Universidade de Brasília, Departamento de Engenharia Mecânica, Brasília, Brasil. E-mails: [email protected], [email protected], [email protected], [email protected], [email protected], [email protected], [email protected] b Corporación Universitaria Unicomfacauca, Popayán, Cauca, Colômbia. E-mail: [email protected] *Corresponding author https://doi.org/10.1590/1679-78256256 ABSTRACT This study aimed to use a simulated vehicle to asses quantitatively the head and neck injuries of the occupants, in a frontal car crash, when the driver has only one hand on the steering wheel, such as while using a cell phone when driving. First, we conducted a survey of NHTSA reports on real laboratory tests of frontal collisions involving sedans. The effects of these collisions on the neck of a Hybrid III 50th percentile male crash test dummy were measured in terms of average head acceleration and force along the X, Z, and Y-axes. These acceleration, force and torque values obtained from the NHTSA database were used to validate the simulated model. The results obtained were compared with case E, the standard dummy position used in frontal collision tests. The results obtained in the simulation of the four cases of driving with only one hand demonstrate a probability of more than 67% that the driver will sustain AIS+2 injuries during a frontal crash. -

Occupant Dynamics in Rollover Crashes: Influence of Roof
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Springer - Publisher Connector Annals of Biomedical Engineering, Vol. 35, No. 11, November 2007 (Ó 2007) pp. 1973–1988 DOI: 10.1007/s10439-007-9355-1 Occupant Dynamics in Rollover Crashes: Influence of Roof Deformation and Seat Belt Performance on Probable Spinal Column Injury 1 2 3 4 MARTHA W. BIDEZ, JOHN E. COCHRAN JR., DOTTIE KING, and DONALD S. BURKE III 1Department of Biomedical Engineering, University of Alabama at Birmingham, 2100 3rd Avenue North, Suite 410, Birmingham, AL 35203, USA; 2Department of Aerospace Engineering, Auburn University, Auburn, AL, USA; 3The King Consulting Group, Inc., Birmingham, AL, USA; and 4Bidez & Associates, Birmingham, AL, USA (Received 20 November 2006; accepted 6 July 2007; published online 20 July 2007) Abstract—Motor vehicle crashes are the leading cause of INTRODUCTION death in the United States for people ages 3–33, and rollover crashes have a higher fatality rate than any other crash mode. Motor vehicle crashes are the leading cause of death At the request and under the sponsorship of Ford Motor in the United States for persons of every age from 3 Company, Autoliv conducted a series of dynamic rollover through 33.18 Rollover crashes, in particular, have a tests on Ford Explorer sport utility vehicles (SUV) during 1998 and 1999. Data from those tests were made available to higher fatality rate than any other crash mode. Of the the public and were analyzed in this study to investigate the 6,159,287 police reported crashes in 2005 in the United magnitude of and the temporal relationship between roof States, only 4.1% involved a rollover. -
Increasing Seat Belt Use Among 8- to 15-Year-Olds Volume II Appendices This Publication Is Distributed by the U.S
Increasing Seat Belt Use Among 8- to 15-Year-Olds Volume II Appendices This publication is distributed by the U.S. Department of Transportation, National Highway Traffic Safety Administration, in the interest of information exchange. The opinions, findings and conclusions expressed in this publication are those of the author(s) and not necessarily those of the Department of Transportation or the National Highway Traffic Safety Administration. The United States Government assumes no liability for its content or use thereof. If trade or manufacturers’ names or products are mentioned, it is because they are considered essential to the object of the publication and should not be construed as an endorsement. The United States Government does not endorse products or manufacturers. 1. Report No. 2. Government Accession No. 3. Recipient's Catalog No. DOT HS 810 966 4. Title and Subtitle 5. Report Date May 2008 Increasing Seat Belt Use Among 8- to 15-Year-Olds: 6. Performing Organization Code Volume II: Appendices 7. Authors 8. Performing Organization Report No. Michelle Kuhn and Jed Lam 9. Performing Organization Name and Address 10. Work Unit No. (TRAIS) Aeffect, Inc. 520 Lake Cook Road, Suite 100 11. Contract or Grant No. Deerfield, IL 60015 DTNH22-03-C-05121 12. Sponsoring Agency Name and Address 13. Type of Report and Period Covered Office of Behavioral Safety Research Summary Research Report National Highway Traffic Safety Administration September, 2003-December, 2006 1200 New Jersey Avenue SE. 14. Sponsoring Agency Code Washington, DC 20590 15. Supplementary Notes 16. Abstract The broad aim of this research project was to determine the nature and causes of non-use of seat belts among 8- to 15- year-olds, and to recommend interventions and strategic approaches to increase usage among this age group. -

The Thor-Advanced Frontal Crash Test Dummy
THOR ADVANCED TEST DUMMY - BIOFIDELITY AND INJURY ASSESSMENT D. Beach R. White, Jr. T. Shams N. Rangarajan GESAC Inc., Boonsboro, MD M. Haffner National Highway Traffic Safety Administration (NHTSA), D.O.T., Washington, DC ABSTRACT This paper will discuss the advances in biofidelity and injury assessment provided by the THOR Frontal Crash Test Dummy, particularly in regard to use by the aircraft safety industry. Following a brief background on the THOR development project, injury data from the Kegworth crash in 1989 will be presented to exemplify the specific types and severity of injuries which may occur in a commercial airline crash. Based on this injury data, five specific regions of the dummy (face, neck, lower abdomen, pelvis - femur, and lower extremities) will be discussed in detail. The biomechanical background, mechanical design and instrumentation will be discussed for each region of the dummy. Additionally, a series of THOR impact test data will be presented to show the biofidelic response of the lower abdomen and femur - pelvis - knee assemblies to impact forces. INTRODUCTION For several years the National Highway Traffic Safety Administration (NHTSA) has actively supported the development of an advanced frontal crash test dummy that incorporates improved biofidelic features and significantly expanded instrumentation. This development program, undertaken by GESAC Inc approximately four years ago, has resulted in the design and development of a test device for whole-body trauma assessment in a variety of occupant restraint environments. Figure #1 shows a picture of the new advanced frontal crash test dummy which has been named THOR (Test Device for Human Occupant Restraint). -

Development of Crash Test Dummies Related
EVALUATION OF THE HYBRID III 5TH from certification, OOP and sled testing. The data FEMALE MODIFIED CHEST JACKET & was analyzed using standard hypothesis test methods SPINE BOX (student t-test) to accept or refute the hypothesis that the jackets are effectively the same. The test matrix Joseph D. McFadden was limited in sample size for both the OOP and sled National Highway Traffic Safety Administration tests. The use of a mandrel to assure that the jackets (NHTSA) are dimensionally correct is a novel approach for Unites States improving quality. James L. Stricklin Transportation Research Center, Inc. (TRC) INTRODUCTION Paper Number 11-0334 th The HIII 5 percentile female is regulated by the Code of Federal Regulations (CFR), Title 49, Part ABSTRACT 572 Subpart O. The Agency owns over 20 dummies mostly of the FTSS brand. There are noticeable The SAE has coordinated development of a new differences in the location and shape of the breast of chest jacket and spine box for the Hybrid III (HIII) the chest flesh assembly between the FTSS and Fifth Percentile Female Crash Test Dummy. The Denton brands that have been resolved by the new proposed modifications intend to correct dimensional jackets. Since 2006 NHTSA has been providing both inconsistencies in the chest jacket drawings, make the brands of dummies to its contracted test sites so that jackets in accordance with the new drawings and NHTSA’s Federal Motor Vehicle Safety Standard eliminate a potential source of mechanical noise in (FMVSS) No. 208 tests, especially the low risk the data. NHTSA procured two new chest jackets, deployment tests can be conducted with the same one from each supplier for evaluation. -

Assessment of a Pre-Crash Seatbelt Technology in Frontal Impacts by Using a New Crash Test Sled System with Controllable Pre-Impact Braking
ASSESSMENT OF A PRE-CRASH SEATBELT TECHNOLOGY IN FRONTAL IMPACTS BY USING A NEW CRASH TEST SLED SYSTEM WITH CONTROLLABLE PRE-IMPACT BRAKING Daisuke Ito Susumu Ejima Yoshihiro Sukegawa Jacobo Antona Hisao Ito Japan Automobile Research Institute Japan Fumihito Komeno Tokai Rika Co., Ltd Japan Paper Number 13-0274 ABSTRACT were measured. In this research, a new pre-crash sled system with the The objective of this study is to develop a new method potential to evaluate pre-crash safety restraint systems and tools required for the evaluation of the potential was developed. Crash tests with dummies were benefits of pre-impact safety restraint systems. conducted in order to examine the effectiveness of a PSB. By controlling the posture change during an A pre-crash sled system that can reproduce controlled emergency braking, the reduction of neck and chest pre-impact braking in combination with a variety of injury risk in front impacts was achieved. This crash pulses was built. The sled can be customized confirms the potential of a PSB to enhance occupant from existing vehicles to examine a variety of restraint protection. systems. In addition, a previously validated 50th percentile male Hybrid III dummy with a modified INTRODUCTION lumbar was employed to reconstruct realistic driver’s posture changes at the pre-impact braking phase. Occupant safety in crashes has commonly been discussed by means of experiments or simulations with In order to evaluate the potential benefits of a 50th percentile male crash test dummies and human pre-crash seatbelt (PSB), the modified dummy was computer models in normal sitting posture. -

Harrington-Sierra-Sam-Crash-Test
‘Sierra Sam’ – The Antediluvian Crash Test Dummy [Type the document subtitle] Approximately 1.2 million people are killed on the world’s roads every year. Much of this appalling loss of life can be attributed to motor vehicles and their errant drivers. Since 1949 when the first crash test dummy - ‘Sierra Sam’ - was ‘invented’, motor vehicles have become safer to drive as car manufacturers include more safety features in their vehicles. With the advent of Euro NCAP in 1997, and in conjunction with car manufacturers, safety features have improved significantly for occupants both inside and for those outside the vehicle. Features such as seatbelts, airbags and other safety developments are estimated to have saved nearly 329,000 lives in the US, whilst it is estimated that more than 15,000 lives have been saved on UK roads since safety tests were first launched. With the advent of autonomous cars, it remains to be seen whether road safety will improve further and the number KSIs that occur annually as a result of vehicle collisions will be reduced dramatically. This article focuses on the role of crash test dummies in preventing KSI’s in vehicle collisions. Tom Harrington LL B F Inst. MTD 4/2/2018 ‘Sierra Sam’ – The Antediluvian Crash Test Dummy Tom Harrington LL B F Inst. MTD (April 2018) “Merriam-Webster 1 defines a crash test dummy simply as: “A life-size model of a person used on tests to see what happens to people when a car gets into an accident”. However, Humanities, 2 a global leader in crash test dummy innovation, more specifically defines a crash dummy as: “A calibrated test instrument used to measure human injury potential in collisions. -

DEVELOPMENT and EVALUATION of the ES-2 SIDE IMPACT DUMMY Michiel Van Ratingen, on Behalf of EEVC WG12 European Enhanced Vehicle-Safety Committee, Europe Paper # 336
DEVELOPMENT AND EVALUATION OF THE ES-2 SIDE IMPACT DUMMY Michiel van Ratingen, on behalf of EEVC WG12 European Enhanced Vehicle-safety Committee, Europe Paper # 336 ABSTRACT different side impact dummies. There is a risk that similar tests with the two different dummies do not The issue of the European Directive 96/27/EC: indicate a common result in terms of improving “Protection of Occupants of Motor Vehicles in the vehicle safety and thus trauma induced injury. Such Event of a Side Impact” in 1998 marked an important diversity causes automotive industry serious concern, step in improving vehicle safety in Europe, but also especially if they sell the same vehicle in different confronted car and restraint manufacturers with the markets. difficulties of having to comply with different ISO has initiated the development of the new side standards in the world. Subsequently, harmonisation impact dummy WorldSID to replace the existing of the side impact test procedures and test devices has dummies such that there will be a more advanced become a key objective for industry and governments world single harmonized side impact test dummy. world-wide. The EEVC WG12 on Adult Crash The realistic time frame for development and Dummies has contributed to this objective by evaluation may be up to 10 years before this dummy assessing the design of the existing European side can go into a legislative test procedure. Starting from impact dummy EUROSID-1. Updates to the design an existing regulated dummy, interim harmonization are proposed to make it acceptable for application in could be reached much quicker. -

37269.0001.001.Pdf
Tuhnical R~portPoturntation Pap= 1. R-rt No 1 Covemmmt Access~mNo. 3. Rec~ptent'rCotoloQ No. UM-HSRI-BI-77-19 ------ 4. T~tloand Subt~~Ie 5. R.port Dote March 31 , 1977 GUIDEBOOK ON ANTHROPOMORPHIC TEST DUMMY USAGE 6. Pufornlng Orgont~attonCode --- Pevfovmmg Otgaarot~onRepart No --- A -- 8. J ~uhor's) UM-HSRI-BI-77-19 H. - ----D. Robbins- -- -- 9 Perform~ngOrgm~rot~on Nome md Address , 10 Work Unet No (TRAIS) Highway Safety Research Institute 01 4764 The Uni versi ty of Michi gan II Contract O, Gront N~. Ann Arbor, Michigan 48109 _ 6-901 1 13. Type of Report and Perood Cor*r*d I?. &sor~ng Agoncr Mcend Address Final Report Office of Housing and Bui 1ding Technology July 1976 - March 1977 National Bureau of Standards U. S. Department of Commerce 14. %onsor~npAgency code D.C. 30334 -Notes 16. Abstract This report addresses the role which may be played by impact test dummies in develo~inqcountermeasures to cope with the high incidence of safety problems relaled to building structures. ~ossible-roles are dis- cussed in safety problem identification, countermeasure development, and in the preparation of s tandardi zed test procedures. The parameters of a test using a dummy are grouped according to: 1. representation of a human victim; 2. representation of the environment in which an injury may occur; 3. the interaction between the victim (dummy) and his environ- ment; and 4. the injuries (transducer or other measurements in the case of the dummy) which occur. Dummies are classified according to sophisti- cation ranging from anthropometric form to impact body blocks and finally to sophisticated anthropomorphic test devices used in automotive safety. -

Frontal Offset Crashworthiness Evaluation
Frontal Offset Crashworthiness Evaluation Guidelines for Rating Injury Measures May 2004 Frontal Offset Crashworthiness Evaluation Guidelines for Rating Injury Measures Injury measures obtained from an instrumented 50th percentile male Hybrid III dummy in the driver seat are used to determine the likelihood that an occupant would have sustained significant injury to various body regions. Twenty-eight different measures are recorded in each of the Institute’s frontal offset crash tests: • head acceleration (three directions from head’s center of gravity) • axial force, anterior-posterior force, and anterior-posterior bending moment acting at the connection between the dummy’s head and neck • thoracic spine acceleration (three directions) • sternum compression • femur axial force (each leg) • tibia-femur displacement (each leg) • tibia transverse bending moments (upper and lower, each leg) • tibia axial force (each leg) • foot acceleration (two directions, each foot) The 28 measures are grouped into four body regions: head and neck, chest, left leg and foot, and right leg and foot. Four injury parameters are used to evaluate protection for the head and neck, three parameters for the chest, and six parameters for each leg and foot. Each body region receives an injury protection rating of good, acceptable, marginal, or poor based on the injury parameters for that region. For any body region to receive a good rating, the scores for all injury parameters in that region must indicate good results. If any parameter indicates an acceptable result, then the rating for that body region is acceptable. If any parameter has a marginal result, then the rating for that body region is marginal. -
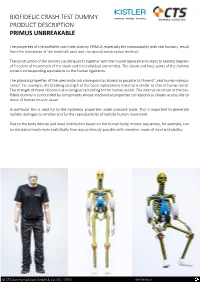
Biofidelic Crash Test Dummy Product Description Primus Unbreakable
BIOFIDELIC CRASH TEST DUMMY PRODUCT DESCRIPTION PRIMUS UNBREAKABLE The properties of the biofidelic crash test dummy PRIMUS, especially the comparability with real humans, result from the interaction of the materials used and the special construction method. The construction of the dummy‘s existing joints together with the muscle replacements leads to realistic degrees of freedom of movement of the trunk and the individual extremities. The elbow and knee joints of the dummy contain corresponding equivalents to the human ligaments. The physical properties of the used materials correspond as closely as possible to those of „real human compo- nents“. For example, the breaking strength of the bone replacement material is similar to that of human bone. The strength of these ribbons is also designed according to the human model. The internal structure of the bio- fidelic dummy is surrounded by components whose mechanical properties correspond as closely as possible to those of human muscle tissue. In particular this is valid for to the hysteresis properties under pressure loads. This is important to gernerate realistic damages to vehicles and for the reproducibility of realistic human movement. Due to the body density and mass distribution based on the human body, motion sequences, for example, can be simulated much more realistically than was previously possible with dummies made of steel and plastics. © CTS dummy-solution GmbH & Co. KG | 2020 003-576e-06.21 BIOFIDELIC CRASH TEST DUMMY PRODUCT DESCRIPTION PRIMUS UNBREAKABLE The biofidelic crash test dummy “PRIMUS breakable” can be used in both sitting and standing positions without any modification. This is a unique construction compared to other crash test dummies. -

Development of a Humanlike Pelvis for a Mid-Sized Male Side Impact Dummy
DEVELOPMENT OF A HUMANLIKE PELVIS FOR A MID-SIZED MALE SIDE IMPACT DUMMY M. van Ratingen, B. Been, H. Boucher TNO Automotive, Crash Safety Centre, The Netherlands S. Compigne, Y. Caire, R. Bouquet, J.P. Verriest INRETS-LBMC Biomechanics and Impact Mechanics Laboratory, France A. Roberts, D. Hynd, A. Sampson, C. Oakley Transport Research Laboratory, United Kingdom OBJECTIVES OF THE RESEARCH response stays low. It was concluded that, in the case of This research was conducted in the frame of the WorldSID PMHS tests, when the greater trochanter is struck, the force [1] and the SID 2000 [2] projects. The objective was to is increased due to the leg inertia. On the contrary, in the develop a physical representation of the human pelvis that tests performed on the dummy, very little increase in force meets the requirements for a mid-sized male side impact is noted at impact corresponding only to the flesh foam crash test dummy acceptable for worldwide harmonisation. compression without contribution of the leg mass. When Compared to existing dummy designs, the pelvis should the flesh foam is completely compressed (bottomed out) better reflect the actual human being in terms of and the impactor contacts the pelvic internal rigid parts, a anthropometry and dynamic behaviour in lateral loading rapid increase of the impactor force is created (figure 1). In conditions. It should also offer enhanced injury assessment that way, the analysis of the human and the current capabilities and durability. EUROSID-1 has permitted a better understanding of the main requirements in terms of the dummy pelvis design.