Management Cadre for Department of Health Sindh 2014
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

46377-002: Khyber to Sangar Road
Initial Environmental Examination P46377-PAK TA 8406-PAK July 2015 PAK: Provincial Road Improvement Program: Rehabilitation of the Khyber to Sangar Road Prepared by the Engineering Consultant International Pvt. Ltd. (ECIL) for the Sindh Works and Services Department and the Asian Development Bank. This initial environmental examination is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Sindh Provincial Road Improvement Project (RRP PAK 46377) Initial Environmental Examination March 2015 TA 8406-PAK: Provincial Road Improvement Program: Rehabilitation of the Khyber to Sanghar Road No. 6 Prepared by the Engineering Consultant International Pvt. Ltd (ECIL) for the Sindh Works and Services Department and Asian Development Bank. Draft Report I. INTRODUCTION ................................................................................................................. 4 A. The Project ...................................................................................................................... 4 B. Purpose and Scope of the IEE ........................................................................................ -

Organizational Presence in Union Councils of Sindh - ER - Floods 2011
Organizational presence in Union Councils of Sindh - ER - Floods 2011 Gilgit Baltistan China ! ! ! ! ! ! ! ! ! !! ! ! !! Khyber Pakhtun! khwa !! ! ! Azad Kashmi!r! Disputed Territory Afghanistan Fata ! 4 Punjab Tangwani Kashmore Thul Balochistan Kashmore India Jacobabad Jacobabad Iran Ubauro Kanhdkot Sindh Shikarpur Garhi Khairo Khanpur (Shikarpur) Ghotki Arabian sea Shahdadkot Shikarpur Qubo Saeed Khan Lakhi Daharki Garhi Yasin Pano Aqil Miro Khan Ghotki Ratodero Sukkur Mirpur Mathelo Kingri Qambar Shahdadkot Rohri Kambar Ali Khan Larkana Khairpur Khangarh Larkana Gambat Warah Bakrani Sukkur Kot Diji Salehpat Dokri Sobodhero Mehar Khairpur Nathan Shah Kandiaro Mirwah Ghulam Shah Bagrani Saeedpur Bhiria Naushahro Feroze Dadu Dadu Naushahro Feroze Faiz Ganj Khairpur Moro Nara Johi Kazi Ahmed Daur Shaheed Benazirabad Nawabshah Sehwan Sinjhoro Barhoon Sakrand Shahdadpur Sanghar Ashgarabad Sinjhoro Sindh Jaffar Khan Laghari Kurkali Jhatia Jhol Khipro Hala Manik ThaheemSyes Sughatullah Shaheed Manjhand Khori Tando Adam Sanghar Hatungo Matiari Jan Nawaz Ali Jamshoro Jhando Mari Matiari Dassori Khahi Mirabad Mirpur Khas Pithoro Thano Bula Khan Kotri Shadi pali Pithoro Saabho Qasimabad Tando Allah Yar Tando Allah Yar Umerkot Hyderabad City Hyderabad Sanjar Chang Dengan Dad Jarwar Samaro Umerkot Hyderabad Kot Ghulam Muhammad Latifabad MMirir pImuamr B uKx Hhadai Bsux Burgury padhario Tando Muhammad Khan Saeed Khan Lund Digri Chachro Matli Sufan Shah Kunri Mulakatyar Mir Khuda Buksh Saeed Matto Lakhat Tando Jan Mohammad Karachi City Thatta Malir -
Jamshoro Blockwise
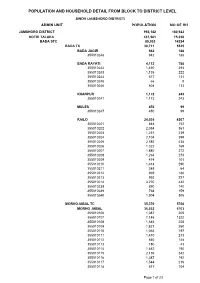
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (JAMSHORO DISTRICT) ADMIN UNIT POPULATION NO OF HH JAMSHORO DISTRICT 993,142 180,922 KOTRI TALUKA 437,561 75,038 BADA STC 85,033 14234 BADA TC 30,711 5525 BADA JAGIR 942 188 355010248 942 188 BADA RAYATI 4,112 788 355010242 1,430 294 355010243 1,135 222 355010244 677 131 355010245 66 8 355010246 804 133 KHANPUR 1,173 243 355010241 1,173 243 MULES 450 99 355010247 450 99 RAILO 24,034 4207 355010201 844 152 355010202 2,054 361 355010203 1,251 239 355010204 2,104 399 355010205 2,585 438 355010206 1,022 169 355010207 1,880 272 355010208 1,264 273 355010209 474 101 355010210 1,414 290 355010211 348 64 355010212 969 186 355010213 993 227 355010214 3,270 432 355010238 890 140 355010239 768 159 355010240 1,904 305 MORHOJABAL TC 35,370 5768 MORHO JABAL 35,032 5703 355010106 1,087 205 355010107 7,146 1322 355010108 1,646 228 355010109 1,821 260 355010110 1,065 197 355010111 1,410 213 355010112 840 148 355010113 180 43 355010114 1,462 190 355010115 2,136 342 355010116 1,387 192 355010117 1,544 216 355010118 617 104 Page 1 of 23 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (JAMSHORO DISTRICT) ADMIN UNIT POPULATION NO OF HH 355010119 79 15 355010120 3,665 538 355010121 951 129 355010122 2,161 343 355010123 2,169 355 355010124 1,468 261 355010125 2,198 402 TARBAND 338 65 355010126 338 65 PETARO TC 18,952 2941 ANDHEJI-KASI 1,541 292 355010306 1,541 292 BELO GHUGH 665 134 355010311 665 134 MANJHO JAGIR 659 123 355010307 659 123 MANJHO RAYATI 1,619 306 355010310 1,619 -

Sindh Province - Flood Analysis (Flood Extent from 27 August 2010 to 07 September 2010)
Pakistan Floods: Sindh Province - Flood Analysis (Flood Extent from 27 August 2010 to 07 September 2010) Kashmore Taluka Thul Taluka Kashmore PUNJAB Jacobabad Taluka Kandhkot Taluka BALOCHISTAN Jaccobabad Ubauro Taluka Shikarpur Taluka Garhi Khairo Taluka Khanpur Taluka Ghotki Taluka Shikarpur Lakhi Taluka Garhi Yasin Taluka Shahdad Kot Taluka Pano Aqil Taluka Ghotki Daharki Taluka Miro Khan Taluka Sukkur Taluka Ratodero Taluka Kambar Ali Khan Taluka Mirpur Mathelo Taluka Kingri Taluka Rohri Taluka Qambar Shahdad kot Larkana Taluka Khairpur Taluka Khangarh Taluka Larkana Gambat Taluka Hamal Lake Warah Taluka Sukkur Dokri Taluka Kot Diji Taluka Salehpat Taluka Sobho Dero Taluka Mehar Taluka An estimated 7 million people are affected Khairpur Nathan Shah Taluka Kandiaro Taluka Mirwah Taluka 19 districts and 7,277 villages are affected. 1,098,720 houses are damaged Bhiria Taluka 199 deaths and 1,072 injuries are reported Naushahro Feroze (Source: NDMA, PDMA, GBDMA, FDMA as of 13092010) Dadu Khairpur Faiz Ganj Taluka Naushahro Feroze Taluka Dadu Taluka Moro Taluka Nara Taluka Johi Taluka Manchar Lake Daulat Pur Taluka Nawabshah Taluka Flood Water entered Jhanagar ! ! S.Banazirabad and Bajara towns as Manchar lake brusted as of 13 Sep 2010 Sehwan Taluka SINDH (UNOCHA Sit Rep # 24) Sakrand Taluka Shahdadpur Taluka Sanghar Taluka Water Supplies to Shewan tehsil I N D I A was cut down due to possible Sinjhoro Taluka contamination as of 13 Sep 2010 Sanghar Hala Taluka (UNOCHA Sit Rep # 24). Khipro Taluka Tando Adam Taluka Matiari Jam Nawaz -
Schools List for Teach for Change 2Nd Batch
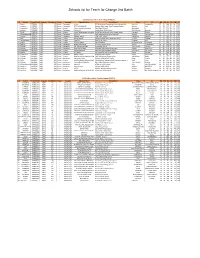
Schools list for Teach for Change 2nd Batch ESSP Schools List For Teach for Change (PHASE-II) S # District School Code Program Enrollment Phase Category Operator Name School Name Taluka UC ND NM NS ED EM ES 1 Sukkur ESSP0041 ESSP 435 Phase I Elementary Ali Bux REHMAN Model Computrized School Mubrak Pur. Pano Akil Mubarak Pur 27 40 288 69 19 729 2 Jamshoro ESSP0046 ESSP 363 Phase I Elementary RAZA MUHAMMAD Shaheed Rajib Anmol Free Education System Sehwan Arazi 26 28 132 67 47 667 3 Hyderabad ESSP0053 ESSP 450 Phase I Primary Free Journalist Foundation Zakia Model School Qasimabad 4 25 25 730 68 20 212 4 Khairpur ESSP0089 ESSP 476 Phase I Elementary Zulfiqar Ali Sachal Model Public School Thari Mirwah Kharirah 27 01 926 68 31 711 5 Ghotki ESSP0108 ESSP 491 Phase I Primary Lanjari Development foundation Sachal Sarmast model school dargahi arbani Khangarh Behtoor 27 49 553 69 20 705 6 ShaheedbenazirabaESSP0156 ESSP 201 Phase I Elementary Amir Bux Saath welfare public school (mashaik) Sakrand Gohram Mari 26 15 244 68 08 968 7 Khairpur ESSP0181 ESSP 294 Phase I Elementary Naseem Begum Faiza Public School Sobhodero Meerakh 27 15 283 68 20 911 8 Dadu ESSP0207 ESSP 338 Phase I Primary ghulam sarwar Danish Paradise New Elementary School Kn Shah Chandan 27 03 006 67 34 229 9 TandoAllahyar ESSP0306 ESSP 274 Phase I Primary Himat Ali New Vision School Chumber Jarki 25 24 009 68 49 275 10 Karachi ESSP0336 ESSP 303 Phase I Primary Kishwar Jabeen Mazin Academy Bin Qasim Twon Chowkandi 24 51 388 67 14 679 11 Sanghar ESSP0442 ESSP 589 Phase I Elementary -
Sanghar Blockwise
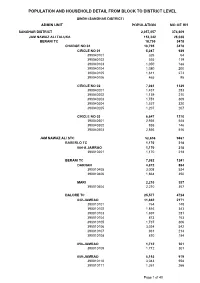
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (SANGHAR DISTRICT) ADMIN UNIT POPULATION NO OF HH SANGHAR DISTRICT 2,057,057 374,609 JAM NAWAZ ALI TALUKA 153,342 28,038 BERANI TC 18,795 3478 CHARGE NO 04 18,795 3478 CIRCLE NO 01 5,087 939 390040101 326 64 390040102 555 119 390040103 1,050 188 390040104 1,080 200 390040105 1,611 273 390040106 465 95 CIRCLE NO 02 7,061 1329 390040201 1,437 283 390040202 1,139 210 390040203 1,751 309 390040204 1,527 320 390040205 1,207 207 CIRCLE NO 03 6,647 1210 390040301 2,936 548 390040302 855 146 390040303 2,856 516 JAM NAWAZ ALI STC 52,656 9467 BABERLO TC 1,170 218 084-A JAMRAO 1,170 218 390010201 1,170 218 BERANI TC 7,082 1241 DARHAN 4,872 884 390010405 3,008 534 390010406 1,864 350 MARI 2,210 357 390010404 2,210 357 DALORE TC 25,577 4724 042-JAMRAO 11,662 2171 390010101 764 148 390010102 1,816 343 390010103 1,697 281 390010104 873 153 390010105 1,737 306 390010106 3,034 542 390010107 931 214 390010108 810 184 058-JAMRAO 1,712 301 390010109 1,712 301 059-JAMRAO 5,192 979 390010110 3,043 558 390010111 1,267 266 Page 1 of 40 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL SINDH (SANGHAR DISTRICT) ADMIN UNIT POPULATION NO OF HH 390010112 882 155 060-JAMRAO 3,062 548 390010113 888 142 390010117 1,622 310 390010118 552 96 061-JAMRAO 2,079 364 390010114 2,079 364 062-JAMRAO 1,149 232 390010115 1,149 232 063-JAMRAO 721 129 390010116 721 129 JAMPUR TC 9,347 1634 BHADAR 7,357 1235 390010301 3,715 625 390010303 3,642 610 JAMPUR 1,990 399 390010302 1,990 399 MASHAIKH ODHO TC 9,480 -

District Wise Status of Villages Under Khushal Pakistan Programme During the Year 2003-2004
DISTRICT WISE STATUS OF VILLAGES UNDER KHUSHAL PAKISTAN PROGRAMME DURING THE YEAR 2003-2004 Sr. Est: Amount %age of No. Name of Village Taluka District Comp: U/Prog: Work Remarks 1 Jan Muhammad Moosa Kotri Dadu 0.672 100%, 02-2004 Completed 2 Manthar Khoso Kotri Dadu 0.413 100%, 02-2004 Completed 3 Muhammad Ali Khaskheli T.B.Khan Dadu 1.182 100%, 01-2004 Completed 4 Haji Nisar Palari T.B.Khan Dadu 1.320 100%, 02-2004 Completed 5 Detha T.B.Khan Dadu 1.470 Total 3.587 1.470 DISTRICT WISE STATUS OF VILLAGES UNDER KHUSHAL PAKISTAN PROGRAMME DURING THE YEAR 2003-2004 Sr. Est: Amount %age of No. Name of Village Taluka District Comp: U/Prog: Work Remarks 1 Khuda Bux Mahar Mirpur Mathelo Ghotki 0.585 100%, 08-2004 Received on 17-05-2004 Total 0.585 0.000 DISTRICT WISE STATUS OF VILLAGES UNDER KHUSHAL PAKISTAN PROGRAMME DURING THE YEAR 2003-2004 Sr. Est: Amount %age of No. Name of Village Taluka District Comp: U/Prog: Work Remarks 1 Muhammad Qasim Tunio Sobho Dero Khairpur 0.370 100%, 05-2004 Completed 2 Ahmed Ali Khaskheli Sobho Dero Khairpur 0.367 100%, 05-2004 Completed 3 Nooh Pota Sobho Dero Khairpur 0.307 100%, 05-2004 Completed 4 Pholri (Two Parts) Faiz Gunj Khairpur 1.573 100%, 05-2004 Completed 5 Maldesi Solangi Sobho Dero Khairpur 0.472 100%, 06-2004 Completed 6 Karam Ali Sial Sobho Dero Khairpur 0.112 100%, 06-2004 Completed 7 Abu Bakar Pato & Khair Muhammad Faiz Gunj Khairpur 1.859 100%, 07-2004 Completed 8 Barkat Ali Arain Sobho Dero Khairpur 0.098 100%, 06-2004 Completed 9 Rab Parto Khairpur Khairpur 0.237 100%, 06-2004 Completed -

List of Dehs in Sindh
List of Dehs in Sindh S.No District Taluka Deh's 1 Badin Badin 1 Abri 2 Badin Badin 2 Achh 3 Badin Badin 3 Achhro 4 Badin Badin 4 Akro 5 Badin Badin 5 Aminariro 6 Badin Badin 6 Andhalo 7 Badin Badin 7 Angri 8 Badin Badin 8 Babralo-under sea 9 Badin Badin 9 Badin 10 Badin Badin 10 Baghar 11 Badin Badin 11 Bagreji 12 Badin Badin 12 Bakho Khudi 13 Badin Badin 13 Bandho 14 Badin Badin 14 Bano 15 Badin Badin 15 Behdmi 16 Badin Badin 16 Bhambhki 17 Badin Badin 17 Bhaneri 18 Badin Badin 18 Bidhadi 19 Badin Badin 19 Bijoriro 20 Badin Badin 20 Bokhi 21 Badin Badin 21 Booharki 22 Badin Badin 22 Borandi 23 Badin Badin 23 Buxa 24 Badin Badin 24 Chandhadi 25 Badin Badin 25 Chanesri 26 Badin Badin 26 Charo 27 Badin Badin 27 Cheerandi 28 Badin Badin 28 Chhel 29 Badin Badin 29 Chobandi 30 Badin Badin 30 Chorhadi 31 Badin Badin 31 Chorhalo 32 Badin Badin 32 Daleji 33 Badin Badin 33 Dandhi 34 Badin Badin 34 Daphri 35 Badin Badin 35 Dasti 36 Badin Badin 36 Dhandh 37 Badin Badin 37 Dharan 38 Badin Badin 38 Dheenghar 39 Badin Badin 39 Doonghadi 40 Badin Badin 40 Gabarlo 41 Badin Badin 41 Gad 42 Badin Badin 42 Gagro 43 Badin Badin 43 Ghurbi Page 1 of 142 List of Dehs in Sindh S.No District Taluka Deh's 44 Badin Badin 44 Githo 45 Badin Badin 45 Gujjo 46 Badin Badin 46 Gurho 47 Badin Badin 47 Jakhralo 48 Badin Badin 48 Jakhri 49 Badin Badin 49 janath 50 Badin Badin 50 Janjhli 51 Badin Badin 51 Janki 52 Badin Badin 52 Jhagri 53 Badin Badin 53 Jhalar 54 Badin Badin 54 Jhol khasi 55 Badin Badin 55 Jhurkandi 56 Badin Badin 56 Kadhan 57 Badin Badin 57 Kadi kazia -

Initial Environmental Examination
Initial Environmental Examination July 2017 PAK: Multitranche Financing Facility Central Asia Regional Economic Cooperation Corridor Development Investment Program Section 1 to 6 (Main Report) Prepared by Sambo Engineering Co., Ltd., Korea and Associated Consultancy Center (PVT) Ltd., Pakistan for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 20 June 2017) Currency Unit –Pakistan Rupee/s (PRs) PRs 1.00 USD $0.00954 USD $1.00 PRs 104.8 ABBREVIATIONS ADB Asian Development Bank ADF Asian Development Fund ACW Additional Carriage Way CAPE Country Assessment Program Evaluation CAREC Central Asia Regional Economic Cooperation CBE Construction Business Expenses CPEC China-Pakistan Economic Corridor DFID Department for International Development EA Executing Agency ECW Existing Carriageway EIA Environmental Impact Assessment EIRR Economic Internal Rate of Return EMP Environmental Management Plan FFA Framework Financing Agreement FIRR Financial Internal Rate of Return GDP Gross Domestic Product GoP Government of Pakistan IA Implementing Agency HDM Highway Development & Management IEE Initial Environmental Examination IP Indigenous People IPP Indigenous People Plan IRR Internal Rate of Return IRI International Roughness Index JBIC Japan Bank for International Cooperation LARP Land Acquisition and Resettlement Plan LARF Land Acquisition and Resettlement Framework LIBOR London Interbank Offered Rate MFF Multi-tranche Financing Facility MTDF Medium-Term Development Framework NHA National Highway Authority NHDSIP National Highway Development -

KARACHI RANGE 01 Sadar S/N Police Station Name Complete
KARACHI RANGE 01 Sadar S/N Police Station Name Complete Address of PS 01 Preedy Preedy Stret Temple road Karachi 02 City Court City Court near Karachi post office Tahir Saifuddin Road Karachi 03 Artillery Maidan Near Art Councial Pakistan near M.R.Kyani Road Karachi 04 Garden Heera Nund Khaim Sing Road Garden 05 Nabi Bux Heera Nand Cam Singh Road Karachi 06 Eidgah Inside Risala PS Nishtar road Karachi 07 Kharader Kharadar Police Station M.A.Jinnah Road Karachi 08 Mithadar M.A.Jinnah road Karachi 09 Risala Nishtar Road near Juna Market Karachi 10 City Court 02 Clifton S/N Police Station Name Complete Address of PS 11 Darakshan Plot No.1270 Street No.31 Khayaban Roomi Phase No.8 12 Gizri Plot No.P-38,11 Commercial Street Phase No.4 DHA Karachi Plot No.PS-1 Khyaban-e-Razwan Phase No.7 Ext DHA Main 13 Defence Korangi Road Karachi 14 Clifton Near Pak Tawar PTC Telephone Exchange Karachi Plot No.PS-1 Khyaban-e-Razwan Phase No.7 Ext DHA Main 15 Boat Basin Korangi Road Karachi 16 Frere Khaliq uz Zaman Road near Lully Bridge Karachi 03 Gulshan S/N Police Station Name Complete Address of PS 17 Gulshan-e-Igbal 18 Madina Main University Road Saforah Goth Chowrangi Kacchi Abadi 19 Sacahal Karachi 20 New 21 PIB Colony 22 Aziz Bhatti 23 Gulista-e-Jauhar 24 Bahadurabad 04 Kemari S/N Police Station Name Complete Address of PS 25 Jackson 26 KPT 27 Docks 28 Maripur 29 Sher Shah 30 DSP KESC 31 Women PS Gora Qabrastan Main Shahra-e-Faisal Karachi 32 N.A.B PS 33 SHO KESC 05 Liaquat Abad S/N Police Station Name Complete Address of PS 34 Liaquatabad Block 5 -
PAKISTAN, YEAR 2017: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 18 June 2018
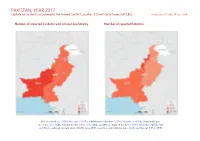
PAKISTAN, YEAR 2017: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 18 June 2018 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; China/India bor- der status: CIA, 2006; Kashmir border status: CIA, 2004; geodata of disputed borders: GADM, November 2015a; Nat- ural Earth, undated; incident data: ACLED, June 2018; coastlines and inland waters: Smith and Wessel, 1 May 2015 PAKISTAN, YEAR 2017: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 18 JUNE 2018 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Riots/protests 3644 6 7 Conflict incidents by category 2 Battles 325 249 915 Development of conflict incidents in 2017 2 Remote violence 169 74 388 Violence against civilians 124 85 291 Methodology 3 Strategic developments 67 0 0 Conflict incidents per province 4 Total 4329 414 1601 This table is based on data from ACLED (datasets used: ACLED, June 2018). Localization of conflict incidents 4 Disclaimer 6 Development of conflict incidents in 2017 This graph is based on data from ACLED (datasets used: ACLED, June 2018). 2 PAKISTAN, YEAR 2017: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 18 JUNE 2018 Methodology an incident occured, or the provincial capital may be used if only the province is known. -

Land Acquisition and Resettlement Plan
MFF Central Asia Regional Economic Cooperation Corridor Development Investment Program (RRP PAK 48404) Resettlement Plan July 2017 PAK: Multitranche Financing Facility Central Asia Regional Economic Cooperation Corridor Development Investment Program Petaro–Sehwan Additional Carriageway–Section I Prepared by the National Highway Authority, Pakistan for the Asian Development Bank. Petaro-Sehwan Additional Carriageway Section-1 LARP CURRENCY EQUIVALENTS (as of 30 May 2017) Currency Unit – Pakistan Rupee/s (PRs) PRs 1.00 = USD $0.00953 USD $1.00 = PRs 104.919 ACRONYM AD Assistant Director ADB Asian Development Bank DH displaced household DPs displaced persons COI Corridor of Impact CBO Community Based Organization DCR District Census Report DD Deputy Director DO(R) District Officer (Revenue) EDO Executive District Officer EIA Environmental Impact Assessment EMP Environmental Management Plan ft feet GM General Manager GOP Government of Pakistan IP Indigenous People km kilometres LAA Land Acquisition Act 1894 LAR Land Acquisition and Resettlement LARP Land Acquisition and Resettlement Plan M&E Monitoring and Evaluation MFF Multi-Tranche Financial Facility NGO Non-Governmental Organization NHA National Highway Authority PMU Project Management Unit ROW Right-of-Way r.ft. running feet s.ft. square feet SPS Safeguard Policy Statement 2009 Page ii Petaro-Sehwan Additional Carriageway Section-1 LARP GLOSSARY compensation payment in cash/voucher or kind offered to the displaced persons (DPs) against the replacement of the lost asset, resource and income. cut-off-date eligibility for entitlements by a cut-off date, determined at the time of social impacts assessment (SIA) survey, census of displaced persons (DPs), inventory of losses (IOL) and socioeconomic baseline survey.