Progress of Partial Integration of Malaria Control with Other Vector Borne Diseases Control in Northern Thailand
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Comparative Assessment of Resource and Market Access of the Poor in Upland Zones of the Greater Mekong Region
Comparative assessment of resource and market access of the poor in upland zones of the Greater Mekong Region Yangtze Irrawaddy Pearl Red Salween Chao Mekong Phraya David E. Thomas Benchaphun Ekasingh Methi Ekasingh Louis Lebel Hoang Minh Ha Laura Ediger Sithong Thongmanivong Xu Jianchu Chanchai Sangchyoswat Ylva Nyberg Rockefeller Foundation Grant No. 2004 SE 024 2008 Citation: Title: Comparative assessment of resource and market access of the poor in upland zones of the Greater Mekong Region Authors: David E. Thomas, Ph.D. World Agroforestry Centre, Chiang Mai. Benchaphun Ekasingh, Ph.D. Chiang Mai University Methi Ekasingh, Ph.D. Chiang Mai University Louis Lebel, Ph.D. Chiang Mai University Hoang Minh Ha, Ph.D. World Agroforestry Centre, Hanoi & Swedish Agric. University, Uppsala Laura Ediger, Ph.D. World Agroforestry Centre, Kunming (consultant) Sithong Thongmanivong, Ph.D. National University of Laos Xu Jianchu, Ph.D. World Agroforestry Centre, China Chanchai Sangchyoswat, Ph.D. Chiang Mai University Ylva Nyberg, M.Sc. World Agroforestry Center, Hanoi Copyright 2008 World Agroforestry Centre ICRAF Chiang Mai P.O. Box 267, CMU Post Office Chiang Mai, Thailand 50202 [email protected] Submitted to the Rockefeller Foundation as the final product under Grant No. 2004 SE 024 Acknowledgements This volume reports on research conducted during 2004 to 2007 under a research project entitled Comparative assessment of resource and market access of the poor in upland zones of the Greater Mekong Region, organized by the World Agroforestry Centre and Chiang Mai University. The project was made possible by financial support provided under a grant from the Rockefeller Foundation, through its office in Bangkok, Thailand. -

Die Karen: Ideologie, Interessen Und Kultur
Die Karen: Ideologie, Interessen und Kultur Eine Analyse der Feldforschungsberichte und Theorienbildung Magisterarbeit zur Erlangung der Würde des Magister Artium der Philosophischen Fakultäten der Albert-Ludwigs-Universität zu Freiburg i. Br. 1992 vorgelegt von Reiner Buergin aus Weil am Rhein (Ausdruck vom Februar 2000) Inhaltsverzeichnis: Einleitung 1 Thema, Ziele, Vorgehensweise 5 2 Übersicht über die Literatur 6 I Die Karen in Südostasien/Einführung 9 1 Bezeichnungen und Sprache 9 2 Verbreitung der verschiedenen Gruppen und Demographie 10 3 Wirtschaftliche Verhältnisse 12 a) Brandrodungsfeldbau 12 b) Naßreisanbau 13 c) Sonstige wirtschaftliche Tätigkeiten und ökomische Krise 14 4 Soziale und politische Organisation 15 a) Entwicklung der Siedlungsform 15 b) Familie und Haushalt 16 c) Verwandtschaftsstrukturen und -gruppen 17 d) Die Dorfgemeinschaft 17 e) Die Territorialgemeinschaft 18 f) Nationalstaatliche Integration 19 5 Religion und Weltbild 20 a) Traditionelle Religionsformen 20 b) Religiöser Wandel, Buddhismus und Christentum 21 c) Mythologie, Weltbild und Werthaltung 22 II Geschichte der verschiedenen Gruppen 1 Ursprung und Einwanderung nach Hinterindien 24 a) Ursprung der Karen 24 b) Einwanderung nach Hinterindien 25 2 Karen in Hinterindien von ca. 1200 - 1800 25 a) Sgaw und Pwo in Burma 25 b) Die Kayah 27 c) Karen in Thailand 28 3 Karen in Burma und Thailand im 19. Jh. 29 a) Sgaw und Pwo in Burma 29 b) Sgaw und Pwo in Siam 31 c) Sgaw und Pwo in Nordthailand 32 d) Die Kayah im 19. Jahrhundert 33 2 4 Karen in Burma und Thailand -

Maejo University SDG Report 2020
Maejo University SDG Report 2020 Sustainable Development Report 2020 I 1 Contents 03 05 17 22 25 President’s Message No Poverty Zero Hunger Good Health and Well- Quality Education Being 28 30 34 40 42 Gender Equality Clean Water and Affordable and Decent Work and Industrial Innovation Sanitation Clean Energy Economic Growth and Infrastructure 44 46 48 50 53 Reduced Sustainable Cities and Responsible Consumption Climate Action Life Below Water Inequalities Communities and Production 56 64 67 73 74 Life on Land Peace, Justice and Partnerships for the About the Report University Impact Strong Institutions Goals Rankings for the SDGs 2 President’s Message Key role of Maejo University during the crisis of COVID-19 pandemic in the previous two years up to the present is to cope up with various problems disrupting university development. Nevertheless, this dramatic crisis makes us unite to make a dream come true and overcome these obstacles. One achievement which we are proud of Maejo University is the result of the world university ranking by Times Higher Education Impact Ranking of the year 2021. This is on the basis of roles of the university under Sustainable Development Goals: SDGs, and Maejo University is ranked in the range 301- 400 in the world (Ranked fifth of the country). Notably, Maejo University ranks 39th in the world in terms of the contribution to push forward hunger-poverty alleviation, food security, and nutrition of people of all ages. On behalf of the President of Maejo University, I am genuinely grateful to all university executives, personnel, students, and alumni for the glorious success of the country's excellence in agriculture university. -

Forbidden Songs of the Pgaz K'nyau
Forbidden Songs of the Pgaz K’Nyau Suwichan Phattanaphraiwan (“Chi”) / Bodhivijjalaya College (Srinakharinwirot University), Tak, Thailand Translated by Benjamin Fairfield in consultation with Dr. Yuphaphann Hoonchamlong / University of Hawai‘i at Mānoa, Honolulu, Hawai‘i Peer Reviewer: Amporn Jirattikorn / Chiang Mai University, Thailand Manuscript Editor and General Editor: Richard K. Wolf / Harvard University Editorial Assistant: Kelly Bosworth / Indiana University Bloomington Abstract The “forbidden” songs of the Pkaz K’Nyau (Karen), part of a larger oral tradition (called tha), are on the decline due to lowland Thai moderniZation campaigns, internaliZed Baptist missionary attitudes, and the taboo nature of the music itself. Traditionally only heard at funerals and deeply intertwined with the spiritual world, these 7-syllable, 2-stanza poetic couplets housing vast repositories of oral tradition and knowledge have become increasingly feared, banned, and nearly forgotten among Karen populations in Thailand. With the disappearance of the music comes a loss of cosmology, ecological sustainability, and cultural knowledge and identity. Forbidden Songs is an autoethnographic work by Chi Suwichan Phattanaphraiwan, himself an artist and composer working to revive the music’s place in Karen society, that offers an inside glimpse into the many ways in which Karen tradition is regulated, barred, enforced, reworked, interpreted, and denounced. This informative account, rich in ethnographic data, speaks to the multivalent responses to internal and external factors driving moderniZation in an indigenous and stateless community in northern Thailand. Citation: Phattanaphraiwan, Suwichan (“Chi”). Forbidden Songs of the Pgaz K’Nyau. Translated by Benjamin Fairfield. Ethnomusicology Translations, no. 8. Bloomington, IN: Society for Ethnomusicology, 2018. DOI: https://doi.org/10.14434/emt.v0i8.25921 Originally published in Thai as เพลงต้องห้ามของปกาเกอะญอ. -

Exploring Spatial Patterns and Hotspots of Diarrhea in Chiang Mai, Thailand Nakarin Chaikaew*1, Nitin K Tripathi1 and Marc Souris1,2,3
International Journal of Health Geographics BioMed Central Research Open Access Exploring spatial patterns and hotspots of diarrhea in Chiang Mai, Thailand Nakarin Chaikaew*1, Nitin K Tripathi1 and Marc Souris1,2,3 Address: 1Remote Sensing and GIS field of study, Asian Institute of Technology, Pathumthani, Thailand, 2Center for Vector and Vector Borne Diseases, Faculty of Science, Mahidol University, Nakhonpathom, Thailand and 3Institut de Recherche pour le Développement (IRD), Marseille, France Email: Nakarin Chaikaew* - [email protected]; Nitin K Tripathi - [email protected]; Marc Souris - [email protected] * Corresponding author Published: 24 June 2009 Received: 4 March 2009 Accepted: 24 June 2009 International Journal of Health Geographics 2009, 8:36 doi:10.1186/1476-072X-8-36 This article is available from: http://www.ij-healthgeographics.com/content/8/1/36 © 2009 Chaikaew et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: Diarrhea is a major public health problem in Thailand. The Ministry of Public Health, Thailand, has been trying to monitor and control this disease for many years. The methodology and the results from this study could be useful for public health officers to develop a system to monitor and prevent diarrhea outbreaks. Methods: The objective of this study was to analyse the epidemic outbreak patterns of diarrhea in Chiang Mai province, Northern Thailand, in terms of their geographical distributions and hotspot identification. -

Supplementary Materials Anti-Infectious Plants of The
Supplementary Materials Anti‐infectious plants of the Thai Karen: A meta‐analysis Methee Phumthum and Henrik Balslev List of data sources 1. Anderson EF. Plants and people of the Golden Triangle ethnobotany of the hill tribes of northern Thailand. Southwest Portland: Timber Press, Inc.,; 1993. 2. Junkhonkaen J. Ethnobotany of Ban Bowee, Amphoe Suan Phueng, Changwat Ratchaburi. Master thesis. Bangkok: Kasetsart University Library; 2012. 3. Junsongduang A. Roles and importance of sacred Forest in biodiversity conservation in Mae Chaem District, Chiang Mai Province. PhD thesis. Chiang Mai: Chiang Mai University. 2014. 4. Kaewsangsai S. Ethnobotany of Karen in Khun Tuen Noi Village, Mae Tuen Sub‐district, Omkoi District, Chiang Mai Province. Master thesis. Chiang Mai: Chiang Mai University; 2017. 5. Kamwong K. Ethnobotany of Karens at Ban Mai Sawan and Ban Huay Pu Ling, Ban Luang Sub‐District, Chom Thong District, Chiang Mai Province. Master thesis. Chiang Mai: Chiang Mai University; 2010. 6. Kantasrila, R. Ethnobotany fo Karen at Ban Wa Do Kro, Mae Song Sub‐district, Tha Song Yang District, Tak Province. Master thesis. Chiang Mai: Chiang Mai University Library. 2016. 7. Klibai, A. Self‐care with indigenous medicine of long‐eared Karen ethnic group: Case study Ban Mae Sin, Ban Kang Pinjai, Ban Slok, Wang Chin district, Phrae province. Master thesis. Surin: Surin Rajabhat University. 2013. 8. Mahawongsanan, A., Change of herbal plants utilization of the Pgn Kʹnyau : A case study of Ban Huay Som Poy, Mae Tia Watershed, Chom Thong District, Chiang Mai Province. Master thesis. Chiang Mai: Chiang Mai University Library. 2008. 9. Prachuabaree L. Medicinal plants of Karang hill tribe in Baan Pong‐lueg, Kaeng Krachan District, Phetchaburi Province. -

Information to Users
INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type o f computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. Each original is also photographed in one exposure and is included in reduced form at the back of the book. Photographs included in the original manuscript have been reproduced xerographically in this copy. Higher quality 6” x 9” black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order. UMI A Bell & Howell Information Company 300 North Zeeb Road, Aim Arbor Ml 48106-1346 USA 313/761-4700 800/521-0600 Highland Cash Crop Development and Biodiversity Conservation: The Hmong in Northern Thailand by Waranoot Tungittiplakorn B.Sc., Chulalongkorn University, 1988 M..Sc., Asian Institute of Technology, 1991 A Dissertation Submitted in Partial Fulfillment o f the Requirements for the Degree of DOCTOR OF PHILOSOPHY in the Department of Geography We accept this dissertation as conforming to the required standard Dr. -

Zoologische Verhandelingen
1 !\ia h IMOUM^AA^^ f m J t \j ci (p^Y'ti ZOOLOGISCHE VERHANDELINGEN New and recently described freshwater crabs (Crustacea: Decapoda: Brachyura: Potamidae, Gecarcinucidae and Parathelphusidae) from Thailand P.K.L. Ng & P. Naiyanetr C. van Achterberg Nationaal Natuurhistorisch Museum P.O. Box 9517, 2300 RA Leiden The Netherlands C. van Achterberg M.R.R.B. Best J.C. den Hartog R. de Jong M.J.P. van Oijen R.W.R.J. Dekker C.H.J.M. Fransen E. Gittenberger P.J. van Helsdingen M.S. Hoogmoed J. Krikken J. van der Land E.J. van Nieukerken C. Smeenk J. van Toi The Zoologische Verhandelingen, Leiden are published by the Nationaal Natuurhistorisch Museum, Leiden at irregular intervals, usually five to ten times a year —--"/ *-v ><3 O iMew ar io recently ciesi bribed n> crabs ( 'Crystaeea: Dec apocla Potanrt"i CJI *o§ <£$ %J$. '%z >- P.K.L. Ng & P. Naiyanetr O CO 5CHE VERHANDELINGEN O-i i o- 1 An international series of monographs on zoological research published by the Nationaal Natuurhistorisch Museum, Leiden -o CO Jl |# CIP-gegevens Koninklijke Bibliotheek, Den Haag Ng, P.K.L. New and recently described freshwater crabs (Crustacea: Decapoda: Brachyura: Potamidae, Gecarcinucidae and Parathelphusidae) from Thailand/P.K.L. Ng & P. Naiyanetr [ed. C.H.J.M. Fransen]. - Leiden: Nationaal Natuurhistorisch Museum. - 111., figs., tab. - (Zoologische Verhandelingen, ISSN 0024-1652; no. 284). With ref. - ISBN 90-73239-16-8 Subject headings: Crustacea; Decapoda; Thailand. © Nationaal Natuurhistorisch Museum, Leiden Reproduction authorized for non-commercial purposes, providing that acknowledgement is given The Zoologische Verhandelingen may be obtained on an exchange basis. -
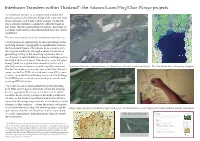
Interbasin Transfers Within Thailand*: the Salween/Luam/Ping/Chao Phraya Projects
Interbasin Transfers within Thailand*: the Salween/Luam/Ping/Chao Phraya projects An interbasin transfer is an engineering scheme that diverts some or all of the discharge from a discrete river basin (or from a sub-basin within a larger catchment) LQWRDVWUHDPGUDLQLQJDFRPSOHWHO\GLͿHUHQWEDVLQRU sub-basin, thereby agumenting the latters’ discharge by a volume equivalent to that diminished from the source catchment. The two main motivations for interbasin transfers are: LQK\GURSRZHUHQJLQHHULQJWRWDNHDGYDQWDJHRIWKH UHFHLYLQJVWUHDPV·WRSRJUDSK\WRVLJQLÀFDQWO\LQFUHDVH the hydrostatic head of the release from a reservoir in the original catchment, through a canal or tunnel to a generating facility in the receiving catchment that is much lower in relative elevation than would be practica- ble within the source basin. The result is a much higher energy yield, for a given dam+reservoir, with only a relatively minor increase in overall capital investment. 7KH6DOZHHQ 7KDQOZLQLQ%XUPHVH HVWXDU\DW0\DZODPD\Q0\DQPDUDQLPDWHGÁ\WKURXJK The Chao Phraya delta at Krungthep (Bangkok) The best example in our study area is the Nam Theun 2 project in the Lao PDR, which diverts some 300 cumecs of water from the Theun-Kading basin into the Xe Bang Fai (XBF) basin, via both excavated new canals and existing XBF tributaries. LQZDWHUUHVRXUFHVPDQDJHPHQWIRUEHWWHUPHHWLQJ both M&I and irrigation demands; where the existing EDVLQ·VDJJUHJDWHGLVFKDUJHLVLQVXFLHQWWRIXOÀO essential needs in dry-season or drought conditions. As seen in the instant case (the Salween-Chao Phraya proposal), the energy requirements of interbasin transfer schemes of this category —where the source catchment is at a lower elevation than the receiving basin may be Oblique space imagery and schematic speed-drDwing of Thanlwin/Salween-Luam-Ping/Chao Phraya interbasin transfer components TXLWHH[WUHPHEXWWKHFRVWEHQHÀWHFRQRPLFVRISXPSLQJ Coordinates: 17°4955N 97°4131E Yuam River From Wikipedia, the free encyclopedia vs. -

Factors Influencing People's Five Precepts Observance, a Case
44 Vol. 1 No. 1 (January – June 2015) Factors Influencing People’s Five Precepts Observance, A Case Study of Pgaz-Koen-Yau Community in Ban Mae Ka Nai, Mae Ho Sub-District, Mae Sariang District, Mae Hong Son Province Uten Laping ,Sangad Chienjuntuk, Kittikoon Phoolaiyao, Kittikoon Phoolaiyao , Pradit Kammungkun and Monthri Wichaiwong Mahamakut Buddhist University Lanna Campus Abstract The purposes of this research are 1) to study the factors influencing people’s observance of the five precepts 2) to identity the advantages of observing the five precepts and 3) to recommends methods for observing the five precepts for people in Pgaz-koen-yau Community in Ban Mae KaNai, Mae Ho Sub-District, Mae Sariang District, Mae Hong Son Province. Ten samples included the abbot, monks, community leader, teacher and residents of Pgaz-koen-yau Community in Ban Mae KaNai, Mae Ho Sub-District, Mae Sariang District, Mae Hong Son Province. Data were collected by interviewed and the descriptive analysis was used to analyze data in order to present quantitative descriptions of the data. The research found that 1) Temples, schools and community have supported the Buddhist activities. The traditional beliefs have conformed to Buddhist teaching and this has encouraged people in the community to observe the five precepts. 2) Observance of the five precepts has led to happy and harmonious community with generous people. Villagers have engaged in the community activates. 3) Village community should be set up. Adults should be the good role models for the youngsters. Keywords : Factors, observance of the five precepts, Pgaz-koen-yau people Introduction Buddhism is considered as an official religion of Thailand as the majority practices Buddhism. -

Lygosoma Haroldyoungi
Check List 9(1): 118–120, 2013 © 2013 Check List and Authors Chec List ISSN 1809-127X (available at www.checklist.org.br) Journal of species lists and distribution N Lygosoma haroldyoungi ISTRIBUTIO Reptilia, Squamata, Scincidae, 1,4 2,3* 4 4 D and (Taylor, 1962): 4 New distribution records Yodchaiy Chuaynkern , Prateep Duengkae , Chantip Chuaynkern , Alongklod Tanomtong RAPHIC G Isara Patawang EO G 1 Thailand Natural History Museum, National Science Museum, Technopolis, Khlong 5, Khlong Luang, Pathum Thani, 12120 Thailand. N O 2 Department of Forest Biology, Faculty of Forestry, Kasetsart University, Chatuchak, Bangkok, 10900 Thailand. 3 Center for Advanced Studies [email protected] Tropical Natural Resources, Kasetsart University, Chatuchak, Bangkok, 10900 Thailand. 4 Department of Biology, Faculty of Science, Khon Kaen University, Mueang, Khon Kaen, 40002 Thailand. OTES * Corresponding author. E-mail: N Abstract: Three newly recorded localities for Lygosoma haroldyoungi (Taylor, 1962) in Thailand are presented, which L. haroldyoungi represent first sightings for Khon Kaen, Sakhon Nakhon and Mukdaharn provinces. An updated compilation of the known geographical distribution of is provided. Lygosoma haroldyoungi Riopa haroldyoungi Lygosoma haroldyoungi was described as a new species photographs were presented to the senior author and are to science, namely , on the basis of now included in the present work. a single specimen (holotype, FMNH 178213) collected had never been recorded from Mukdaharn Province and from the “Base of Doi Suthep near Chiang Mai”, Chiang no voucher specimen from Mukdaharn L.Province haroldyoungi is so Mai Province, northern Thailand (see Taylor, 1962). Very far available, but the identification by photos leaves no few records of that species were subsequently made, doubt on its identity. -

Refugee Camps on the Thailand-Myanmar Border: Potential Places for Expanding Connections Among Karen Baptists Boonsong Thansrithong and Kwanchewan Buadaeng*
ASR: CMU Journal of Social Sciences and Humanities (2017) Vol. 4 No.2 89 Refugee Camps on the Thailand-Myanmar Border: Potential Places for Expanding Connections among Karen Baptists Boonsong Thansrithong and Kwanchewan Buadaeng* Faculty of Social Sciences, Chiang Mai University, Chiang Mai 50200, Thailand *Corresponding author. E-mail: [email protected] https://doi.org/10.12982/CMUJASR.2017.0006 ABSTRACT Since the 1980s, the Burmese army has increasingly seized the Karen National Union (KNU)’s camps and strongholds along the Thailand-Myanmar borderland. Hundreds of thousands of Karen people affected by the war have fled to the Thai side of the border. Since then, ten refugee camps have existed along the border, from Mae Hong Son province in the North to Ratchaburi province in the South. This paper focuses on the operation of the Kawthoolei Karen Baptist Bible School and College (KKBBSC) in the Bae Klaw camp, which is the largest with almost 40,000 residents in 2016. Since 1990, the KKBBSC has produced around 1,000 Bachelor of Theology graduates, thereby increasing the strength of the Karen Baptist church. This paper argues that the refugee camps on the Thailand-Myanmar border are not marginally isolated, but are potential nodes of connection with other places and organiza- tions. Two factors contribute to the potentialities of the camps. First, the camp is an exceptional zone, ruled not by a single government but a liminal contested space of many actors. The second is the camp’s high level of technological development which facilitates transportation and communication for the Karen Baptists.