Chapter 13 OCULAR TRAUMA and OCULAR EMERGENCIES
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ocular Injury; Hazard to Society: a Case Series
Quest Journals Journal of Medical and Dental Science Research Volume 7~ Issue 8 (2020) pp: 34-44 ISSN(Online) : 2394-076X ISSN (Print):2394-0751 www.questjournals.org Research Paper Ocular Injury; Hazard to Society: A Case Series Dr Rashmi kujur1, Dr Pallavi. M.P2, Dr Harshita Dubey3, Dr Varsha4 1Dept. of ophthalmology, Madhav dispensary JAH, GRMC, Gwalior, Madhyapradesh. 2Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 3Senior girls hostel, GRMC, Gwalior, Madhyapradesh. 4Senior girls hostel, GRMC, Gwalior,Madhyapradesh. Corresponding Author: Dr.Pallavi.M.P ABSTRACT Purpose: To describe various types of ocular trauma due to different modes of injuryoccured on the same day Design: Prospective interventional study (case series) Materials & Methods: A series of cases of ocular trauma in different age group on the same day. Results: Five patients of ocular trauma were studied & managed. All five patients were males. Out of 5 cases, 3 cases had open globe injury and 2 cases had closed globe injury. Three out of five patients required surgical intervention while 2 patients were managed with medical therapy. Conclusion: This study describes the types and characteristics of ocular trauma presenting in eye department. The frequency of ocular trauma is common in males. Eye injuries resulting from ocular trauma pose a frequent threat to vision the world over. While afocussed history and prompt ocular examination are essential to immediate management, patient educationregarding safety precautions and risk reduction help to prevent future recurrences. KEYWORDS: Ocular morbidity, Ocular Injury, globe rupture, iridodialysis, fire cracker injury, hyphema, Road Traffic accident (RTA), loss of vision. Received 05 December, 2020; Accepted 20 December, 2020 © The author(s) 2020. -

Traumatic Retinal Detachment Br J Ophthalmol: First Published As 10.1136/Bjo.75.1.18 on 1 January 1991
18 BritishJournalofOphthalmology, 1991,75, 18-21 Traumatic retinal detachment Br J Ophthalmol: first published as 10.1136/bjo.75.1.18 on 1 January 1991. Downloaded from P B Johnston Abstract trauma is a well recognised cause of rhegmato- Seventy-seven patients developed retinal genous retinal detachment, which was reported breaks following an episode of ocular con- by Eagling' to affect 4-6% of such injuries. The tusion, and 65 (84.4%) of these developed characteristics of postcontusion retinal detach- rhegmatogenous retinal detachment. Surgical ments were described by Cox et all and the treatment successfully restored or maintained mechanism ofbreak formation was elucidated by retinal apposition in 74 (96-1%) of the eyes. Delori et all who studied the effect of high speed Thirty-six (46-8%) eyes recovered visual acuity projectiles on enucleated pig eyes. Experimental of6/9orbetter. Ofthe retinal breaks recognised evidence indicates that retinal breaks form at the dialysis at the ora serrata was observed in 49 time of ocular impact. However, clinical reports eyes, of which 28 were situated at the lower show considerable delay in the diagnosis of temporal quadrant. Seventeen eyes had post-traumatic retinal detachment. For example, irregular breaks arising within necrotic retina Cox et all reported that only 30% of post- at the site of scleral impact. Twenty-four traumatic retinal detachments were diagnosed (31.2%) patients had retinal break or retinal within one month of injury, and Ross4 found detachment diagnosed within 24 hours ofinjury 40% in a similar period. and 49 (63-6%) within six weeks. Immediate The following study is of a series of patients retinal detachment was a feature of necrotic who developed retinal breaks or retinal detach- retinal breaks, while inferior oral dialyses led ment after ocular contusion. -

Chapter 32 FOREIGN BODIES of the HEAD, NECK, and SKULL BASE
Foreign Bodies of the Head, Neck, and Skull Base Chapter 32 FOREIGN BODIES OF THE HEAD, NECK, AND SKULL BASE RICHARD J. BARNETT, MD* INTRODUCTION PENETRATING NECK TRAUMA Anatomy Emergency Management Clinical Examination Investigations OPERATIVE VERSUS NONOPERATIVE MANAGEMENT Factors in the Deployed Setting Operative Management Postoperative Care PEDIATRIC INJURIES ORBITAL FOREIGN BODIES SUMMARY CASE PRESENTATIONS Case Study 32-1 Case Study 32-2 Case Study 32-3 Case Study 32-4 Case Study 32-5 Case Study 32-6 *Lieutenant Colonel, Medical Corps, US Air Force; Chief of Facial Plastic Surgery/Otolaryngology, Eglin Air Force Base Department of ENT, 307 Boatner Road, Suite 114, Eglin Air Force Base, Florida 32542-9998 423 Otolaryngology/Head and Neck Combat Casualty Care INTRODUCTION The mechanism and extent of war injuries are sig- other military conflicts. In a study done in Croatia with nificantly different from civilian trauma. Many of the 117 patients who sustained penetrating neck injuries, wounds encountered are unique and not experienced about a quarter of the wounds were from gunshots even at Role 1 trauma centers throughout the United while the rest were from shell or bomb shrapnel.1 The States. Deployed head and neck surgeons must be injury patterns resulting from these mechanisms can skilled at performing an array of evaluations and op- vary widely, and treating each injury requires thought- erations that in many cases they have not performed in ful planning to achieve a successful outcome. a prior setting. During a 6-month tour in Afghanistan, This chapter will address penetrating neck injuries all subspecialties of otolaryngology were encountered: in general, followed specifically by foreign body inju- head and neck (15%), facial plastic/reconstructive ries of the head, face, neck, and skull base. -

Vertical Perspective Medical Assistance Program
Kansas Vertical Perspective Medical Assistance Program December 2006 Provider Bulletin Number 688 General Providers Emergent and Nonemergent Diagnosis Code List Attached is a list of diagnosis codes and whether the Kansas Medical Assistance Program (KMAP) considers the code to be emergent or nonemergent. Providers are responsible for validating whether a particular diagnosis code is covered by KMAP under the beneficiary’s benefit plan and that all program requirements are met. This list does not imply or guarantee payment for listed diagnosis codes. Information about the Kansas Medical Assistance Program as well as provider manuals and other publications are on the KMAP Web site at https://www.kmap-state-ks.us. If you have any questions, please contact the KMAP Customer Service Center at 1-800-933-6593 (in-state providers) or (785) 274-5990 between 7:30 a.m. and 5:30 p.m., Monday through Friday. EDS is the fiscal agent and administrator of the Kansas Medical Assistance Program for the Kansas Health Policy Authority. Page 1 of 347 Emergency Indicators as noted by KMAP: N – Never considered emergent S – Sometimes considered emergent (through supporting medical documentation) Y – Always considered emergent Diagnosis Emergency Diagnosis Code Description Code Indicator 0010 Cholera due to Vibrio Cholerae S 0011 Cholera due to Vibrio Cholerae El Tor S 0019 Unspecified Cholera S 019 Late Effects of Tuberculosis N 0020 Typhoid Fever S 0021 Paratyphoid Fever A S 0022 Paratyphoid Fever B S 0023 Paratyphoid Fever C S 024 Glanders Y 025 Melioidosis -

Bruises- Wounds
Henry Shih OD, MD Medical Director Austin Emergency Center- Anderson Mill 13435 US Highway 183 North Suite 311 Austin, TX 78750 512-614-1200 BRUISES- http://austiner.com/ What are bruises? — Bruises happen when blood vessels under the skin break, but the skin isn’t cut. Blood leaks into the tissues under the skin. Bruises start off red in color, and then turn blue or purple. As they heal, bruises can turn green and yellow. Most bruises heal in 1 to 2 weeks, but some take longer. How are bruises treated? — A bruise will get better on its own. But to feel better and help your bruise heal, you can: o Put a cold gel pack, bag of ice, or bag of frozen vegetables on the injured area every 1 to 2 hours, for 15 minutes each time. Put a thin towel between the ice (or other cold object) and your skin. Use the ice (or other cold object) for at least 6 hours after your injury. Some people find it helpful to ice longer, even up to 2 days after their injury. o Raise the area, if possible – Raising the area above the level of your heart helps to reduce swelling. o Take medicine to reduce the pain and swelling – To treat pain, you can take Tylenol. To treat pain and swelling, you can take ibuprofen (sample brand names: Advil, Motrin). But people who have certain conditions or take certain medicines should not take ibuprofen. If you are unsure, ask your doctor or nurse if you can take ibuprofen. -
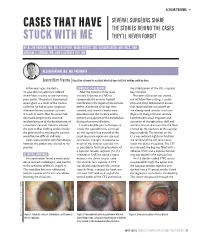
Cases That Have Stuck with Me
OCULAR TRAUMA s SEVERAL SURGEONS SHARE CASES THAT HAVE THE STORIES BEHIND THE CASES STUCK WITH ME THEY’LL NEVER FORGET BY ALLON BARSAM, MD, MA, FRCOPHTH; MARK KONTOS, MD; SOOSAN JACOB, MD, FRCS, DNB; MICHAEL E. SNYDER, MD; AND ELIZABETH YEU, MD ALLON BARSAM, MD, MA, FRCOPHTH Severe Blunt Trauma | A positive outcome for a patient who had been told that nothing could be done. A few years ago, I treated a SURGICAL PROCEDURE the stabilization of the IOL –capsular 41-year-old man who had suffered After the creation of the main bag complex. severe blunt trauma to one eye many incision, I injected an OVD to Phacoemulsification was carried years earlier. The patient experienced tamponade the anterior hyaloid out with low flow settings. I used a severe glare as a result of the trauma, membrane in the region of the zonular stop-and-chop technique to ensure such that he had to wear sunglasses defect. A cohesive OVD was then that minimal force was placed on whenever he was outdoors or even injected, and three iris hooks were the already weak zonular structures in a well-lit room. Also, his vision had placed to keep the iris back and to (Figure 2). Using a Simcoe cannula, decreased progressively since the prevent propagation of the iridodialysis I performed manual irrigation and incident because of the development of during phacoemulsification. aspiration of the epinuclear shell and a traumatic cataract. Doctors advised I used a double-pass technique to soft lens matter to ensure that the force the patient that nothing could remedy create the capsulorhexis, centered exerted on the contents of the capsular the glare and that treating the cataract on the capsular bag instead of the bag was gentle. -

Eleventh Edition
SUPPLEMENT TO April 15, 2009 A JOBSON PUBLICATION www.revoptom.com Eleventh Edition Joseph W. Sowka, O.D., FAAO, Dipl. Andrew S. Gurwood, O.D., FAAO, Dipl. Alan G. Kabat, O.D., FAAO Supported by an unrestricted grant from Alcon, Inc. 001_ro0409_handbook 4/2/09 9:42 AM Page 4 TABLE OF CONTENTS Eyelids & Adnexa Conjunctiva & Sclera Cornea Uvea & Glaucoma Viitreous & Retiina Neuro-Ophthalmic Disease Oculosystemic Disease EYELIDS & ADNEXA VITREOUS & RETINA Blow-Out Fracture................................................ 6 Asteroid Hyalosis ................................................33 Acquired Ptosis ................................................... 7 Retinal Arterial Macroaneurysm............................34 Acquired Entropion ............................................. 9 Retinal Emboli.....................................................36 Verruca & Papilloma............................................11 Hypertensive Retinopathy.....................................37 Idiopathic Juxtafoveal Retinal Telangiectasia...........39 CONJUNCTIVA & SCLERA Ocular Ischemic Syndrome...................................40 Scleral Melt ........................................................13 Retinal Artery Occlusion ......................................42 Giant Papillary Conjunctivitis................................14 Conjunctival Lymphoma .......................................15 NEURO-OPHTHALMIC DISEASE Blue Sclera .........................................................17 Dorsal Midbrain Syndrome ..................................45 -
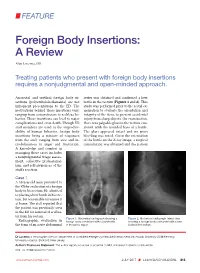
Foreign Body Insertions: a Review
FEATURE Foreign Body Insertions: A Review Alan Lucerna, DO Treating patients who present with foreign body insertions requires a nonjudgmental and open-minded approach. Anorectal and urethral foreign body in- series was obtained and confirmed a beer sertions (polyembolokoilamania) are not bottle in the rectum (Figures 1 and 2). This infrequent presentations to the ED. The study was performed prior to the rectal ex- motivations behind these insertions vary, amination to evaluate the orientation and ranging from autoeroticism to reckless be- integrity of the item, to prevent accidental havior. These insertions can lead to major injury from sharp objects. On examination, complications and even death. Though ED there was palpable glass in the rectum con- staff members are used to the unpredict- sistent with the rounded base of a bottle. ability of human behavior, foreign body The glass appeared intact and no gross insertions bring a mixture of responses bleeding was noted. Given the orientation from the staff, ranging from awe and in- of the bottle on the X-ray image, a surgical credulousness to anger and frustration. consultation was obtained and the patient A knowledge and comfort in managing these cases includes a nonjudgmental triage assess- ment, collective professional- ism, and self-awareness of the staff’s reaction. Case 1 A 58-year-old man presented to the ED for evaluation of a foreign body in his rectum. He admitted to placing a beer bottle in his rec- tum, but was unable to remove it at home. The staff reported that the patient was previously seen in the ED for removal of a vibra- tor from his rectum. -

Foreign Rectal Body – Systematic Review and Meta-Analysis
REVIEW 61 Foreign rectal body – Systematic review and meta-analysis M. Ploner1, A. Gardetto2, F. Ploner3, M. Scharl4, S. Shoap5, H. C. Bäcker5 (1) Department of Anesthesiology and Intensiver Care, Cantonal Spital Lucerne, Lucerne, Switzerland ; (2) Department of Plastic Surgery, Hospital Sterzing, Sterzing, South Tirol, Italy ; (3) Department of Anesthesiology and Emergency Medicine, Hospital Sterzing, South Tirol, Italy ; (4) Department of Gastroenterology and Hepatology, University Hospital Zurich, University of Zurich, Swetzerland ; (5) Department of Orthopaedic Surgery, Columbia University Medical Center, New York, USA. Abstract instrumentation (7). The most common complication is a rectal injury, which can result from a variety of agents and Background : Self-inserted foreign rectal bodies are an objects (8). Often, nonsurgical removal of foreign bodies infrequent occurrence, however they present a serious dilemma to the surgeon, due to the variety of objects, and the difficulty of has been described to be successful – in 11% to 65% – extraction. The purpose of this study is to give a comprehensive (9), however, in many situations, a surgical treatment review of the literature regarding the epidemiology, diagnostic may be essential. There have been a variety of algorithms tools and therapeutic approaches of foreign rectal body insertion. Methods : A comprehensive systematic literature review on introduced for the management of extraction, however, Pubmed/ Medline and Google for ‘foreign bodies’ was performed because of the diversity of foreign bodies, improvisation, on January 14th 2018. A meta-analysis was carried out to evaluate as well creativity of the treating emergency physician the epidemiology, diagnostics and therapeutic techniques. 1,551 abstracts were identified, of which 54 articles were included. -
NEISS Coding Manual January 2018
NNEEIISSSS CCooddiinngg MMaannuuaall JJaannuuaarryy 22001188 NEISS – National Electronic Injury Surveillance System January 2018 Table of Contents Introduction ................................................................................................................................................. 1 General Instructions ................................................................................................................................... 1 General NEISS Reporting Rule .................................................................................................................. 1 Do Report .................................................................................................................................................. 1 Definitions .............................................................................................................................................. 2 Do Not Report ........................................................................................................................................... 3 Specific Coding Instructions ..................................................................................................................... 4 Medical Information Codes ........................................................................................................................ 4 Date of Treatment ..................................................................................................................................... 4 (8 spaces)................................................................................................................................................. -

Injury Description Codes Nature of Injury
Injury Description Codes Nature of Injury Code Narrative Description I. Specific Injury * 01. No Physical Injury i.e., Glasses, contact lenses, artificial appliance, replacement of artificial appliance 02. Amputation Cut off extremity, digit, protruding part of body, usually by surgery, i.e. leg, arm 03. Angina Pectoris Chest pain 04. Burn (Heat) Burns or scald. The effect of contact with hot substances. (Chemical) burns. tissue damage resulting from the corrosive action chemicals, fume, etc., (acids, alkalies) 07. Concussion Brain, cerebral 10. Contusion Bruise - intact skin surface hematoma 13. Crushing To grind, pound or break into small bits 16. Dislocation Pinched nerve, slipped/ruptured disc, herniated disc, sciatica, complete tear, HNP subluxtion, MD dislocation 19. Electric Shock Electrocution 22. Enucleation Removal of organ or tumor 25. Foreign Body * 28. Fracture Breaking of a bone or cartilage 30. Freezing Frostbite and other effects of exposure to low temperature 31. Hearing Loss or Impairment Traumatic only. A separate injury, not the sequelae of another injury 32. Heat Prostration Heat stroke, sun stroke, heat exhaustion, heat cramps and other effects of environmental heat. does not include sunburn 34. Hernia The abnormal protrusion of an organ or part through the containing wall of its cavity 36. Infection The invasion of a host by organisms such as bacteria, fungi, viruses, mold, protozoa or insects, with or without manifest disease. 37. Inflammation The reaction of tissue to injury characterized clinically by heat, swelling, redness and pain *Description intentionally left blank. May 25, 2021 Injury Description Codes Nature of Injury 38. Adverse reaction to a vaccination or * inoculation 40. -

Interesting and Artistic 1 2 3 Grand Prize Winner
s BEST OF 2018: PHOTO CONTEST 1 s SERGEI LUZHETSKIY, MD DANIEL DE SOUZA A Dog’s Cataract COSTA, MD s 2 A Spontaneous Displacement of the Lens WINNER GRAND PRIZE WINNER s PATRIK RAJS Gramophone Record 3 in the Eye INTERESTING AND ARTISTIC YONG s WINNERS OF KAM, MD Anterior CRST’S ANNUAL Segment Dysgenesis 2018 PHOTO CONTEST INTERESTING AND ARTISTIC 1 This is an image of an inherited cataract in a dog. 2 This photo is of the eye of a 46-year-old woman who presented with displacement of the lens into the anterior 4 chamber with no history of ocular trauma. 3 This photo is of the eye of a patient with presbyopia who underwent laser cataract surgery. A multifocal IOL was captured GRAND with a combination of two vintage Zeiss and Pentax lenses. WINNER PRIZE RARE AND UNUSUAL WINNER s This photo shows the eye of a newborn patient with DANIEL 4 increased IOP; a diffusely edematous, hazy, and enlarged DE SOUZA cornea; and an absent Schlemm canal and trabecular COSTA, MD meshwork on surgical exploration, consistent with severe A Prominent anterior segment dysgenesis. Symblepharon 5 The eye of this 5-year-old girl has epidermolysis bullosa and serious ocular manifestations of this condition. Biomicroscopy examination revealed the presence of 5 6 symblepharon in both eyes. The ocular complication was so severe that it deformed the palpebral anatomy. Significant keratoglobus in the eye of this patient with s AARON S. WANG, MD 6 Fish Tank Down Syndrome, who frequently rubs his eyes. This picture RARE AND UNUSUAL was taken just prior to corneal transplantation.