Analysis of the Social Feasibility of Hiv and Aids Programs in Kenya
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Livestock Herd Structures and Dynamics in Garissa County, Kenya Patrick Mwambi Mwanyumba1*, Raphael Wahome Wahome2, Laban Macopiyo3 and Paul Kanyari4
Mwanyumba et al. Pastoralism: Research, Policy and Practice (2015) 5:26 DOI 10.1186/s13570-015-0045-6 SHORT REPORT Open Access Livestock herd structures and dynamics in Garissa County, Kenya Patrick Mwambi Mwanyumba1*, Raphael Wahome Wahome2, Laban MacOpiyo3 and Paul Kanyari4 Abstract In Kenya’s Northeastern Province, pastoralism is the main livestock production system and means of livelihood. However, pastoralists are facing increasing risks such as drought, insecurity, animal diseases, increasing human populations and land fragmentation. This study sought to evaluate household livestock herd structures and dynamics in view of such risks and subsistence and market demands. The study was conducted in Garissa County of Kenya, using a cross-sectional household survey. The data was analysed for descriptive statistics of household livestock status, dynamics and demographic parameters. The results showed that females of reproductive age formed over 50 % of all livestock species. Cattle had the highest turnover and all species’ mortalities accounted for the greater proportion of exits. Cattle had the highest multiplication and growth rates, but also the highest mortality, offtake, commercial offtake and intake rates. Goats had the lowest mortalities, offtake, commercial offtake and intake rates. Overall, the herds were structured to provide for both immediate and future needs in terms of milk, sales and herd replacement as well as for rapid recovery after disasters. The livestock herd dynamics indicate efforts at culling, restocking, retention of valuable categories of animals, and natural events. Livestock populations would be annihilated over time if the trends in end balances and negative growth rates were to continue and not be interrupted by the upward phases of the livestock cycles. -

Baseline Review and Ecosystem Services Assessment of the Tana River Basin, Kenya
IWMI Working Paper Baseline Review and Ecosystem Services Assessment of the Tana 165 River Basin, Kenya Tracy Baker, Jeremiah Kiptala, Lydia Olaka, Naomi Oates, Asghar Hussain and Matthew McCartney Working Papers The publications in this series record the work and thinking of IWMI researchers, and knowledge that the Institute’s scientific management feels is worthy of documenting. This series will ensure that scientific data and other information gathered or prepared as a part of the research work of the Institute are recorded and referenced. Working Papers could include project reports, case studies, conference or workshop proceedings, discussion papers or reports on progress of research, country-specific research reports, monographs, etc. Working Papers may be copublished, by IWMI and partner organizations. Although most of the reports are published by IWMI staff and their collaborators, we welcome contributions from others. Each report is reviewed internally by IWMI staff. The reports are published and distributed both in hard copy and electronically (www.iwmi.org) and where possible all data and analyses will be available as separate downloadable files. Reports may be copied freely and cited with due acknowledgment. About IWMI IWMI’s mission is to provide evidence-based solutions to sustainably manage water and land resources for food security, people’s livelihoods and the environment. IWMI works in partnership with governments, civil society and the private sector to develop scalable agricultural water management solutions that have -
Flash Update
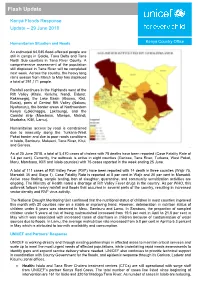
Flash Update Kenya Floods Response Update – 29 June 2018 Humanitarian Situation and Needs Kenya Country Office An estimated 64,045 flood-affected people are still in camps in Galole, Tana Delta and Tana North Sub counties in Tana River County. A comprehensive assessment of the population still displaced in Tana River will be completed next week. Across the country, the heavy long rains season from March to May has displaced a total of 291,171 people. Rainfall continues in the Highlands west of the Rift Valley (Kitale, Kericho, Nandi, Eldoret, Kakamega), the Lake Basin (Kisumu, Kisii, Busia), parts of Central Rift Valley (Nakuru, Nyahururu), the border areas of Northwestern Kenya (Lokichoggio, Lokitaung), and the Coastal strip (Mombasa, Mtwapa, Malindi, Msabaha, Kilifi, Lamu). Humanitarian access by road is constrained due to insecurity along the Turkana-West Pokot border and due to poor roads conditions in Isiolo, Samburu, Makueni, Tana River, Kitui, and Garissa. As of 25 June 2018, a total of 5,470 cases of cholera with 78 deaths have been reported (Case Fatality Rate of 1.4 per cent). Currently, the outbreak is active in eight counties (Garissa, Tana River, Turkana, West Pokot, Meru, Mombasa, Kilifi and Isiolo counties) with 75 cases reported in the week ending 25 June. A total of 111 cases of Rift Valley Fever (RVF) have been reported with 14 death in three counties (Wajir 75, Marsabit 35 and Siaya 1). Case Fatality Rate is reported at 8 per cent in Wajir and 20 per cent in Marsabit. Active case finding, sample testing, ban of slaughter, quarantine, and community sensitization activities are ongoing. -

National Drought Early Warning Bulletin June 2021
NATIONAL DROUGHT MANAGEMENT AUTHORITY National Drought Early Warning Bulletin June 2021 1 Drought indicators Rainfall Performance The month of May 2021 marks the cessation of the Long- Rains over most parts of the country except for the western and Coastal regions according to Kenya Metrological Department. During the month of May 2021, most ASAL counties received over 70 percent of average rainfall except Wajir, Garissa, Kilifi, Lamu, Kwale, Taita Taveta and Tana River that received between 25-50 percent of average amounts of rainfall during the month of May as shown in Figure 1. Spatio-temporal rainfall distribution was generally uneven and poor across the ASAL counties. Figure 1 indicates rainfall performance during the month of May as Figure 1.May Rainfall Performance percentage of long term mean(LTM). Rainfall Forecast According to Kenya Metrological Department (KMD), several parts of the country will be generally dry and sunny during the month of June 2021. Counties in Northwestern Region including Turkana, West Pokot and Samburu are likely to be sunny and dry with occasional rainfall expected from the third week of the month. The expected total rainfall is likely to be near the long-term average amounts for June. Counties in the Coastal strip including Tana River, Kilifi, Lamu and Kwale will likely receive occasional rainfall that is expected throughout the month. The expected total rainfall is likely to be below the long-term average amounts for June. The Highlands East of the Rift Valley counties including Nyeri, Meru, Embu and Tharaka Nithi are expected to experience occasional cool and cloudy Figure 2.Rainfall forecast (overcast skies) conditions with occasional light morning rains/drizzles. -

KENYA POPULATION SITUATION ANALYSIS Kenya Population Situation Analysis
REPUBLIC OF KENYA KENYA POPULATION SITUATION ANALYSIS Kenya Population Situation Analysis Published by the Government of Kenya supported by United Nations Population Fund (UNFPA) Kenya Country Oce National Council for Population and Development (NCPD) P.O. Box 48994 – 00100, Nairobi, Kenya Tel: +254-20-271-1600/01 Fax: +254-20-271-6058 Email: [email protected] Website: www.ncpd-ke.org United Nations Population Fund (UNFPA) Kenya Country Oce P.O. Box 30218 – 00100, Nairobi, Kenya Tel: +254-20-76244023/01/04 Fax: +254-20-7624422 Website: http://kenya.unfpa.org © NCPD July 2013 The views and opinions expressed in this report are those of the contributors. Any part of this document may be freely reviewed, quoted, reproduced or translated in full or in part, provided the source is acknowledged. It may not be sold or used inconjunction with commercial purposes or for prot. KENYA POPULATION SITUATION ANALYSIS JULY 2013 KENYA POPULATION SITUATION ANALYSIS i ii KENYA POPULATION SITUATION ANALYSIS TABLE OF CONTENTS LIST OF ACRONYMS AND ABBREVIATIONS ........................................................................................iv FOREWORD ..........................................................................................................................................ix ACKNOWLEDGEMENT ..........................................................................................................................x EXECUTIVE SUMMARY ........................................................................................................................xi -

Marsabit County Disease Surveillance and Response
ACCESS TO TREATMENT FOR NEGLECTED DISEASES – Experiences In Marsabit County Presented by: Abduba Liban CDSC, Marsabit County 0n 9th February 2016 at the ASTMH Conference OUTLINE 1. Brief county profile 2. Status of kala-azar marsabit county 3. Diagnosis and Treatment of Kala azar in Marsabit 4. Challenges of Accessing Treatment 5. Addressing the challenges at County Level 6. Way forward Marsabit County County Profile County Population • Visceral leishmaniasis VL (Kala azar) . Kala azar a systemic parasitic disease . It is transmitted through infected female sand fly. There are three forms of leishmaniasis; Visceral leishmanaisis (VL), Cutaneous, Muco-cutaneous . There are three endemic foci in kenya o Northwest Kenya - West Pokot, Baringo and Turkana o Eastern Province - Machakos, Kitui, Mwingi and kyuso o North-eastern Province - along the Somali border Visceral Leishmaniasis in Marsabit . VL is the common form leishmania in Marsabit . VL is a new problem in Marsabit county . There is only one treatment centre for kala azar in Marsabit – Marsabit Hospital . Distance from the furthest endemic region to the centre is 500km Kala-azar Cases by Months Kala-azar Cases by Locations Diagnosis & Treatment of Kala-azar in Marsabit Diagnosis and treatment is based on the Kenyan VL guidelines Diagnosis . A patient should be suspected in a patient from, or visiting, an endemic area who presents with: o Fever > 2 weeks o Splenomegaly o Weight loss o Diagnosis through rapid test kits – rK39 Diagnosis & Treatment of Kala-azar in Marsabit Diagnosis and treatment is based on the Kenyan VL guidelines Treatment If patient is found positive after all differentials are ruled out, they are: . -

The 2015 Al-Shabaab's Attack in Garissa, Kenya. an Immersion Into
SIT Graduate Institute/SIT Study Abroad SIT Digital Collections Capstone Collection SIT Graduate Institute Winter 12-2016 The 2015 al-Shabaab's attack in Garissa, Kenya. An immersion into the structural, socio-political and psychological roots of violence Mathilde Simon SIT Graduate Institute Follow this and additional works at: https://digitalcollections.sit.edu/capstones Part of the African Studies Commons Recommended Citation Simon, Mathilde, "The 2015 al-Shabaab's attack in Garissa, Kenya. An immersion into the structural, socio-political and psychological roots of violence" (2016). Capstone Collection. 2954. https://digitalcollections.sit.edu/capstones/2954 This Thesis (Open Access) is brought to you for free and open access by the SIT Graduate Institute at SIT Digital Collections. It has been accepted for inclusion in Capstone Collection by an authorized administrator of SIT Digital Collections. For more information, please contact [email protected]. Running Head: THE 2015 AL-SHABAAB’S ATTACK IN GARISSA, KENYA 1 The 2015 al-Shabaab’s attack in Garissa, Kenya An immersion into the structural, socio-political and psychological roots of violence Mathilde Simon PIM-73 A capstone paper submitted in partial fulfillment of the requirements of a Masters of Art in Peacebuilding and Conflict Transformation at SIT Graduate Institute, Vermont, USA. Advisor: Teresa Healy THE 2015 AL-SHABAAB’S ATTACK IN GARISSA, KENYA 2 Consent to Use of Capstone I hereby grant permission for World Learning to publish my capstone on its websites and in any of its digital/electronic collections, and to reproduce and transmit my CAPSTONE ELECTRONICALLY. I understand that World Learning’s websites and digital collections are publicly available via the Internet. -

Kenya Tana River Basin Road Construction Projects (I) and (II)
Kenya Tana River Basin Road Construction Projects (I) and (II) Report Date: October 2002 Field Survey: July-August 2001 1. Project Profile and Japan’s ODA Loan Site Map Project Site (Near Garsen) 1.1. Background Kenya’s economy remains largely dependent on exports of its main agricultural products such as coffee and tea . The largest constraint on the country’s agricultural sector was insufficient rain, making land less productive. It was therefore necessary to develop an irrigation system using water resources from the Tana River, the longest river in Kenya. The Tana River Development Agency was founded in 1974 to promote the Tana River Area Development Program, with a focus on irrigation. Especially, in downstream of Tana River, large scaled irrigation plan had been implemented. For the successful development of Tana River area including the irrigation plan, the development of road network was inevitable. The conditions of roads in downstream areas deteriorated so badly that the roads were inaccessible during the rainy season, and even during the dry season, the road traffic was not easy. Given this situation, the Government of Kenya decided to implement the Tana River Basin Road Construction Project (hereinafter referred to as “Project I”) and requested for Japan’s ODA Loan in 1980. During the implementation of Project I, however, financial constraints of the Government of Kenya in appropriating local-cost materials caused significant delays in the road construction. The situation in Kenya at that time, attributed to various factors including deterioration of its economy, caused such financial constraints, which had not been foreseeable at the time of appraisal. -

Inside Kenya's War on Terror: Breaking the Cycle of Violence in Garissa
Inside Kenya’s war on terror: breaking the cycle of violence in Garissa Christopher Wakube, Thomas Nyagah, James Mwangi and Larry Attree Inside Kenyas war on terror: The name of Garissa county in Kenya was heard all over the world after al-Shabaab shot breaking the cycle of violence dead 148 people – 142 of them students – at Garissa University College in April 2015. But the in Garissa story of the mounting violence leading up to that horrific attack, of how and why it happened, I. Attacks in Garissa: towards and of how local communities, leaders and the government came together in the aftermath the precipice to improve the security situation, is less well known. II. Marginalisation and division But when you ask around, it quickly becomes clear that Garissa is a place where divisions and in Garissa dangers persist – connected to its historic marginalisation, local and national political rivalries III. “This is about all of us” – in Kenya, and the ebb and flow of conflict in neighbouring Somalia. Since the attack, the local perceptions of violence security situation has improved in Garissa county, yet this may offer no more than a short IV. Rebuilding trust and unity window for action to solve the challenges and divisions that matter to local people – before other forces and agendas reassert their grip. V. CVE job done – or a peacebuilding moment to grasp? This article by Saferworld tells Garissa’s story as we heard it from people living there. Because Garissa stepped back from the brink of terror-induced polarisation and division, it is in some Read more Saferworld analysis ways a positive story with global policy implications. -

County Name County Code Location
COUNTY NAME COUNTY CODE LOCATION MOMBASA COUNTY 001 BANDARI COLLEGE KWALE COUNTY 002 KENYA SCHOOL OF GOVERNMENT MATUGA KILIFI COUNTY 003 PWANI UNIVERSITY TANA RIVER COUNTY 004 MAU MAU MEMORIAL HIGH SCHOOL LAMU COUNTY 005 LAMU FORT HALL TAITA TAVETA 006 TAITA ACADEMY GARISSA COUNTY 007 KENYA NATIONAL LIBRARY WAJIR COUNTY 008 RED CROSS HALL MANDERA COUNTY 009 MANDERA ARIDLANDS MARSABIT COUNTY 010 ST. STEPHENS TRAINING CENTRE ISIOLO COUNTY 011 CATHOLIC MISSION HALL, ISIOLO MERU COUNTY 012 MERU SCHOOL THARAKA-NITHI 013 CHIAKARIGA GIRLS HIGH SCHOOL EMBU COUNTY 014 KANGARU GIRLS HIGH SCHOOL KITUI COUNTY 015 MULTIPURPOSE HALL KITUI MACHAKOS COUNTY 016 MACHAKOS TEACHERS TRAINING COLLEGE MAKUENI COUNTY 017 WOTE TECHNICAL TRAINING INSTITUTE NYANDARUA COUNTY 018 ACK CHURCH HALL, OL KALAU TOWN NYERI COUNTY 019 NYERI PRIMARY SCHOOL KIRINYAGA COUNTY 020 ST.MICHAEL GIRLS BOARDING MURANGA COUNTY 021 MURANG'A UNIVERSITY COLLEGE KIAMBU COUNTY 022 KIAMBU INSTITUTE OF SCIENCE & TECHNOLOGY TURKANA COUNTY 023 LODWAR YOUTH POLYTECHNIC WEST POKOT COUNTY 024 MTELO HALL KAPENGURIA SAMBURU COUNTY 025 ALLAMANO HALL PASTORAL CENTRE, MARALAL TRANSZOIA COUNTY 026 KITALE MUSEUM UASIN GISHU 027 ELDORET POLYTECHNIC ELGEYO MARAKWET 028 IEBC CONSTITUENCY OFFICE - ITEN NANDI COUNTY 029 KAPSABET BOYS HIGH SCHOOL BARINGO COUNTY 030 KENYA SCHOOL OF GOVERNMENT, KABARNET LAIKIPIA COUNTY 031 NANYUKI HIGH SCHOOL NAKURU COUNTY 032 NAKURU HIGH SCHOOL NAROK COUNTY 033 MAASAI MARA UNIVERSITY KAJIADO COUNTY 034 MASAI TECHNICAL TRAINING INSTITUTE KERICHO COUNTY 035 KERICHO TEA SEC. SCHOOL -

North Eastern - Wagalla Massacre (Nairobi) - RTJRC14.06 (NHIF Auditorium) (Benson Kaaria Testimony)
Seattle University School of Law Seattle University School of Law Digital Commons The Truth, Justice and Reconciliation I. Core TJRC Related Documents Commission of Kenya 6-14-2011 Public Hearing Transcripts - North Eastern - Wagalla Massacre (Nairobi) - RTJRC14.06 (NHIF Auditorium) (Benson Kaaria Testimony) Truth, Justice, and Reconciliation Commission Follow this and additional works at: https://digitalcommons.law.seattleu.edu/tjrc-core Recommended Citation Truth, Justice, and Reconciliation Commission, "Public Hearing Transcripts - North Eastern - Wagalla Massacre (Nairobi) - RTJRC14.06 (NHIF Auditorium) (Benson Kaaria Testimony)" (2011). I. Core TJRC Related Documents. 78. https://digitalcommons.law.seattleu.edu/tjrc-core/78 This Report is brought to you for free and open access by the The Truth, Justice and Reconciliation Commission of Kenya at Seattle University School of Law Digital Commons. It has been accepted for inclusion in I. Core TJRC Related Documents by an authorized administrator of Seattle University School of Law Digital Commons. For more information, please contact [email protected]. ORAL SUBMISSIONS MADE TO THE TRUTH, JUSTICE AND RECONCILIATION COMMISSION ON TUESDAY, 14 TH JUNE, 2011 AT THE NHIF AUDITORIUM, NAIROBI PRESENT Tecla Namachanja Wanjala - The Acting Chair, Kenya Gertrude Chawatama - Commissioner, Zambia Berhanu Dinka - Commissioner, Ethiopia Ahmed Sheikh Farah - Commissioner, Kenya Tom Ojienda - Commissioner, Kenya Margret Wambui Shava - Commissioner, Kenya Ronald Slye - Commissioner, USA (The Commission commenced at 10.00 a.m.) (The Acting Chair (Ms. Namachanja) introduced herself and the other TJRC Commissioners) (Opening Prayers) The Acting Chair (Ms. Namachanja): Hearing Clerk, could we have the witness in? Welcome to today’s hearing of the Truth, Justice and Reconciliation Commission, today being the 14 th day of June, 2011. -

Missionaries, the State
DEVELOPMENT AT THE MARGINS: MISSIONARIES, THE STATE, AND THE TRANSFORMATION OF MARSABIT, KENYA IN THE TWENTIETH CENTURY By Jonathan M. Hansen Dissertation Submitted to the Faculty of the Graduate School of Vanderbilt University in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY in History May, 2015 Nashville, Tennessee Dennis C. Dickerson, Ph.D. Moses E. Ochonu, Ph.D. Michael D. Bess, Ph.D. Gregory Melchor-Barz, Ph.D. To my mom and dad ii ACKNOWLEDGEMENTS The path to completing this dissertation was much longer than I expected, and there were many days I felt like giving up on the whole project. The fact that I did not throw in the towel is largely due to my friends, family, and Vanderbilt community who encouraged me along the way, or just spent time listening to my frustrations. I would like to thank my advisor, Dennis Dickerson, and the other members of my committee: Moses Ochonu, Michael Bess, and Gregory Melchor-Barz. For a few years I had a regular lunch crew that made the graduate school experience fun, meaningful, and full of sarcasm. Though I may have actually been more productive if our lunches did not last so long. Thank you to Adam, Cory, Elizabeth, Katie, Rachel, and Will, along with the others who joined us from time to time. Thank you to my cohort: Bill, Kevin, and Will. Also, thank you to Jane Anderson and Heidi Welch, who answered so many of my questions through the years with grace and generosity, and made the department office an enjoyable place to me.