Emergency Physicians and Ity Needed for Our Everyday Lives
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cesarean Section Rates from the 2015 Leapfrog Hospital Survey
Cesarean Section Rates from the 2015 Leapfrog Hospital Survey Results reflect submissions received by December 31, 2015 Hospital City State Rate Performance Alaska Regional Hospital Anchorage AK 33.5% Willing to Report Bartlett Regional Hospital Juneau AK Declined to Respond Central Peninsula General Hospital Soldotna AK Declined to Respond Fairbanks Memorial Hospital Fairbanks AK 15.3% Fully Meets Standard Mat‐Su Regional Medical Center Palmer AK Declined to Respond Providence Alaska Medical Center Anchorage AK 20.0% Fully Meets Standard Andalusia Regional Hospital Andalusia AL 22.1% Fully Meets Standard Athens‐Limestone Hospital Athens AL Declined to Respond Atmore Community Hospital Atmore AL Declined to Respond Baptist Medical Center East Montgomery AL Declined to Respond Baptist Medical Center South Montgomery AL Declined to Respond Bibb Medical Center Centreville AL Declined to Respond Brookwood Medical Center Birmingham AL 31.9% Some Progress Bryan W. Whitfield Memorial Hospital Demopolis AL Declined to Respond Bullock County Hospital Union Springs AL Declined to Respond Cherokee Medical Center Centre AL Declined to Respond Citizens Baptist Medical Center Talladega AL Declined to Respond Clay County Hospital Ashland AL Declined to Respond Community Hospital of Tallassee Tallassee AL Declined to Respond Coosa Valley Medical Center Sylacauga AL Declined to Respond Crenshaw Community Hospital Luverne AL Declined to Respond Crestwood Medical Center Huntsville AL Declined to Respond Cullman Regional Medical Center Cullman AL Declined -

Hospital Assessment - Amount Paid SFY 2020 (July 2019- June 2020)
Hospital Assessment - Amount Paid SFY 2020 (July 2019- June 2020) Hospital Name Provider Type Hospital System SFY 2020 Paid Assessment Amount ABRAZO ARROWHEAD CAMPUS Urban Acute Hospitals Abrazo Health Care$ 8,277,304 ABRAZO CENTRAL CAMPUS Urban Acute Hospitals Abrazo Health Care$ 5,988,200 ABRAZO SCOTTSDALE CAMPUS Urban Acute Hospitals Abrazo Health Care$ 3,705,416 ABRAZO WEST CAMPUS Urban Acute Hospitals Abrazo Health Care$ 6,919,768 ARIZONA GENERAL HOSPITAL Urban Acute Hospitals Dignity$ 233,840 AURORA BEHAVIORAL HEALTH Large Psychiatric Hospitals Aurora Behavioral Health System$ 648,432 AURORA BEHAVIORAL HEALTH - TEMPE Large Psychiatric Hospitals Aurora Behavioral Health System$ 472,420 BANNER - UNIVERSITY MEDICAL CENTER PHOENIX Urban Acute Hospitals Banner Health$ 15,279,028 BANNER - UNIVERSITY MEDICAL CENTER SOUTH Urban Acute Hospitals Banner Health$ 4,454,810 BANNER - UNIVERSITY MEDICAL CENTER TUCSON Pediatric-Intensive General Acute Hospitals Banner Health$ 11,791,293 BANNER BAYWOOD MEDICAL CENTER Urban Acute Hospitals Banner Health$ 10,143,600 BANNER BEHAVORIAL HEALTH MEDICAL CENTER Large Psychiatric Hospitals Banner Health$ 472,736 BANNER BOSWELL MEDICAL CENTER Urban Acute Hospitals Banner Health$ 8,121,200 BANNER CASA GRANDE MEDICAL CENTER Non-CAH Rural Acute Hospitals Banner Health$ 3,354,024 BANNER DEL E WEBB MEDICAL CENTER Urban Acute Hospitals Banner Health$ 9,183,908 BANNER DESERT MEDICAL CENTER Pediatric-Intensive General Acute Hospitals Banner Health$ 12,579,857 BANNER ESTRELLA MEDICAL CENTER Urban Acute Hospitals Banner -

Maternal Mortalities and Severe Maternal Morbidity in Arizona Report
Maternal Mortalities and Severe Maternal Morbidity in Arizona December 2020 Table of Contents Executive Summary ................................................................ 6 Section 1: Overview of Maternal Health ............................... 22 Section 2: Maternal Mortality, 2016-2017 ............................ 30 Section 3: Severe Maternal Morbidity, 2016-2019 ............... 48 Section 4: Recommendations for Preventing Maternal Mortality and Severe Maternal Morbidity in Arizona ............ 75 Section 5: Discussion ............................................................. 85 Section 6: Limitations ............................................................ 87 Section 7: Appendices ........................................................... 90 Section 8: References .......................................................... 121 Dedication Dedicated to Arianna Dodde and to all the women that have been lost during pregnancy, delivery, or postpartum; whose stories inspire us to continue fighting for the health of all mothers in Arizona. Acknowledgements The Arizona Department of Health Services (ADHS) would like to acknowledge Dr. Robert Johnson, MD, who is a founding member and Chair of the Arizona Maternal Mortality Review Committee (MMRC); his time and commitment to this committee has supported ADHS in initiating the Maternal Mortality Review Program (MMRP) and conducting ongoing reviews of maternal mortalities in Arizona. ADHS would also like to acknowledge the 33 members of the Arizona MMRC who completed the 134 case -

The Interdisciplinary Journal of Health, Ethics, & Policy
TUFTSCOPE THE INTERDISCIPLINARY JOURNAL OF HEALTH, ETHICS, & POLICY A DISCUSSION WITH LYDIA X. Z. BROWN: DISABILITY JUSTICE POTENTIAL FOR WORLD’S FIRST HUMAN HEAD TRANSPLANT d 23AndMe: AT-HOME GENETIC Fall 2017 • Volume 17 Issue I TESTING JOURNAL HISTORY EDITORIAL BOARD INSIDE THIS ISSUE Since 2001, TuftScope: The Interdisciplinary Journal of Health, Ethics, & Policy has provided an academic forum for discus- Editor-in-Chief TuftScope | Fall 2017 • Volume 17, Issue I sion of pertinent healthcare and biosocial issues in today’s Neeki Parsa world. The journal addresses different aspects of health- LETTER FROM THE EDITOR care, bioethics, public health, policy, and active citizen- Managing Editor Moving Forward.....................................................................................5 ship. It is operated and edited by undergraduate students of Tufts University and is advised by an Editorial Board Michael Seleman Neeki Parsa composed of Tufts undergraduates and faculty. Today the journal is one of the few peer-reviewed, undergraduate- Senior Financial Officer Ursula Biba NEWS BRIEFS published journals in the country. Selections From Our News Analysis Blog.....................................6 Faculty Advisors TuftScope Staff PUBLISHER AND PRINTER Harry Bernheim, PhD TuftScope is published by the TuftScope Journal organiza- Alexander Queen, PhD FEATURE INTERVIEW tion at Tufts University. The journal is printed by Puritan A Discussion with Lydia X. Z. Brown ..............................................8 Press, NH (http://www.puritanpress.com). Junior Financial Officer Michael Seleman Akari Miki COPYRIGHT TUFTSCOPE 2016 News & Analysis Editor BOOK REVIEW TuftScope is an open-access journal distributed under the Ted Midthun A Book Review of Mark Wolynn’s It Didn’t Start with You......12 terms of the Creative Commons Attribution License, which Neeki Parsa permits use, distribution, and reproduction in any medium, Research Highlights Editor provided the original author and source are credited. -

Tenet Healthcare Annual Report 2021
Tenet Healthcare Annual Report 2021 Form 10-K (NYSE:THC) Published: February 19th, 2021 PDF generated by stocklight.com UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, DC 20549 Form 10-K ☒ Annual report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the fiscal year endedD ecember 31, 2020 OR ☐ Transition report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the transition period from to Commission File Number 1-7293 ________________________________________ TENET HEALTHCARE CORPORATION (Exact name of Registrant as specified in its charter) Nevada 95-2557091 (State of Incorporation) (IRS Employer Identification No.) 14201 Dallas Parkway Dallas, TX 75254 (Address of principal executive offices, including zip code) (469) 893-2200 (Registrant’s telephone number, including area code) ________________________________________________________ Securities registered pursuant to Section 12(b) of the Act: Title of each class Trading symbol Name of each exchange on which registered Common stock, $0.05 par value THC New York Stock Exchange 6.875% Senior Notes due 2031 THC31 New York Stock Exchange Securities registered pursuant to Section 12(g) of the Act: None ________________________________________________________ Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes x No ¨ Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No x Indicate by check mark whether the Registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months, and (2) has been subject to such filing requirements for the past 90 days. -
Find a Hospital with In-Network Providers
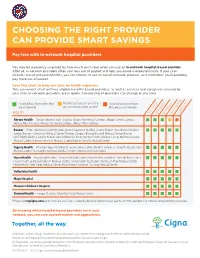
CHOOSING THE RIGHT PROVIDER CAN PROVIDE SMART SAVINGS Pay less with in-network hospital providers You may be pleasantly surprised by how much you’ll save when you use an in-network hospital-based provider. After all, in-network providers often cost less out of pocket and help you avoid unexpected costs. If your plan includes out-of-network benefits, you can choose to use an out-of-network provider. Just remember, you’ll probably pay more out of pocket. Save this chart to help you save on health expenses. This convenient chart outlines eligible hospital-based providers, as well as services and caregivers covered by your plan. In-network providers are in green. Contracting of providers can change at any time. Hospital-based providers that Most hospital-based providers Hospital-based providers are in-network are in-network; some are not* that are out-of-network FACILITY ANESTHESIAPATHOLOGYRADIOLOGYER PHYSICIANSHOSPITALIST Abrazo Health – Abrazo Arizona Heart Hospital, Abrazo Arrowhead Campus, Abrazo Central Campus, Abrazo Mesa Hospital, Abrazo Scottsdale Campus, Abrazo West Campus Banner – Banner Baywood Heart Hospital, Banner Baywood Medical Center, Banner Thunderbird Medical Center, Banner – University Medical Center Phoenix Campus, Banner Boswell Medical Center, Banner Del E Webb Medical Center, Banner Desert Medical Center, Banner Estrella Medical Center, Banner Gateway Medical Center, Banner Ironwood Medical Center, Banner Ocotillo Medical Center Dignity Health – Chandler Regional Medical Center, Mercy Gilbert Medical Center, St. Joseph’s Hospital and Medical Center, St. Joseph’s Westgate Medical Center, Arizona General Hospital HonorHealth – HonorHealth John C. Lincoln Medical Center, HonorHealth Scottsdale Shea Medical Center, HonorHealth Scottsdale Osborn Medical Center, HonorHealth Scottsdale Thompson Peak Medical Center, HonorHealth Deer Valley Medical Center, HonorHealth Sonoran Crossing Medical Center Valleywise Health Mayo Hospital Phoenix Children’s Hospital Steward Health – Tempe St. -

Hospital Facilities
Cigna uses hospitalist(s) at the following hospital facilities. For information on Cigna’s participating hospitalists, please call the Member Services number on the back of your Cigna ID card. ABRAZO ARROWHEAD CAMPUS MAYO CLINIC ARIZONA ABRAZO CENTRAL CAMPUS MAYO CLINIC HOSPITAL ABRAZO SCOTTSDALE CAMPUS MERCY GILBERT MEDICAL CENTER ABRAZO WEST CAMPUS MOUNT GRAHAM REGIONAL MEDICAL CENTER BANNER BAYWOOD MEDICAL CENTER MOUNTAIN VISTA MEDICAL CENTER BANNER BAYWOOD RHODES REHAB NORTHERN COCHISE COMMUNITY HOSPITAL BANNER BOSWELL MEDICAL CENTER NORTHWEST MEDICAL CENTER BANNER CASA GRANDE MEDICAL CENTER NORTHWEST MEDICAL CENTER SAHUARITA BANNER CHILDRENS AT DESERT OASIS HOSPITAL BANNER DEL WEBB MEDICAL CENTER PAGE HOSPITAL BANNER DESERT MEDICAL CENTER PHOENIX CHILDRENS HOSPITAL BANNER ESTRELLA MEDICAL CENTER SAN JUAN REGIONAL MEDICAL CENTER BANNER GATEWAY MEDICAL CENTER SCOTTSDALE HEALTHCARE OSBORN BANNER GOLDFIELD MEDICAL CENTER SCOTTSDALE HEALTHCARE SHEA MEDICAL CENTER BANNER HEART HOSPITAL SCOTTSDALE HEALTHCARE THOMPSON PEAK BANNER IRONWOOD MEDICAL CENTER SELECT SPECIALTY HOSPITAL BANNER OCOTILLO MEDICAL CENTER ST JOSEPHS HOSPITAL & MEDICAL CENTER BANNER THUNDERBIRD MEDICAL CENTER ST LUKES MEDICAL CENTER BANNER UNIVERSITY MEDICAL CENTER PHOENIX CAMPUS SUMMIT HEALTHCARE BANNER UNIVERSITY MEDICAL CENTER SOUTH CAMPUS TEMPE ST LUKES HOSPITAL BANNER UNIVERSITY MEDICAL CENTER TUCSON CAMPUS TUCSON MEDICAL CENTER CANCER TREATMENT CENTERS OF AMERICA VALLEYWISE HEALTH CANYON VISTA MEDICAL CENTER VERDE VALLEY MEDICAL CENTER CARONDELET HOLY CROSS HOSPITAL -
2019 List of Crcs.Xlsx
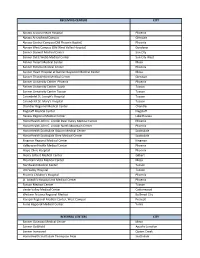
RECEIVING CENTERS CITY Abrazo Arizona Heart Hospital Phoenix Abrazo Arrowhead Campus Glendale Abrazo Central Campus (Old Phoenix Baptist) Phoenix Abrazo West Campus (Old West Valley Hospital) Goodyear Banner Boswell Medical Center Sun City Banner Del E Webb Medical Center Sun City West Banner Desert Medical Center Mesa Banner Estrella Medical Center Phoenix Banner Heart Hospital at Banner Baywood Medical Center Mesa Banner Thunderbird Medical Center Glendale Banner University Center Phoenix Phoenix Banner University Center South Tucson Banner University Center Tucson Tucson Carondelet St. Joseph's Hospital Tucson Carondelet St. Mary's Hospital Tucson Chandler Regional Medical Center Chandler Flagstaff Medical Center Flagstaff Havasu Regional Medical Center Lake Havasu HonorHealth John C. Lincoln Deer Valley Medical Center Phoenix HonorHealth John C. Lincoln North Mountain Center Phoenix HonorHealth Scottsdale Osborn Medical Center Scottsdale HonorHealth Scottsdale Shea Medical Center Scottsdale Kingman Regional Medical Center Kingman Valleywise Health Medical Center Phoenix Mayo Clinic Hospital Phoenix Mercy Gilbert Medical Center Gilbert Mountain Vista Medical Center Mesa Northwest Medical Center Tucson Oro Valley Hospital Tucson Phoenix Children's Hospital Phoenix St. Joseph's Hospital and Medical Center Phoenix Tucson Medical Center Tucson Verde Valley Medical Center Cottonwood Western Arizona Regional Medical Bullhead City Yavapai Regional Medical Center, West Campus Prescott Yuma Regional Medical Center Yuma REFERRAL CENTERS CITY Banner Gateway Medical Center Mesa Banner Goldfield Apache Junction Banner Ironwood Queen Creek HonorHealth Scottsdale Thompson Peak Scottsdale Tempe St. Lukes Hospital Tempe. -

Hospital Address City State ZIP Code FY2013 Readmission Penalty
FY2013 FY2014 FY2015 FY2016 ZIP Hospital Address City State Readmission Readmission Readmission Readmission Code Penalty Penalty Penalty Penalty 4315 ALASKA NATIVE MEDICAL CENTER DIPLOMACY ANCHORAGE AK 99508 0.2300% 0.4500% 0.4900% 0.3400% DR 2801 ALASKA REGIONAL HOSPITAL DEBARR ANCHORAGE AK 99508 0% 0.0100% 0% 0.5700% ROAD 3260 BARTLETT REGIONAL HOSPITAL JUNEAU AK 99801 0% 0% 1.2700% 0.4500% HOSPITAL DR 250 CENTRAL PENINSULA GENERAL HOSPITAL HOSPITAL SOLDOTNA AK 99669 0.0700% 0.0900% 1.4100% 1.0200% PLACE PO BOX 160 - CORDOVA COMMUNITY MEDICAL CENTER 602 CHASE CORDOVA AK 99574 Not Assessed Not Assessed Not Assessed Not Assessed AVENUE 1650 FAIRBANKS MEMORIAL HOSPITAL COWLES FAIRBANKS AK 99701 0% 0% 0.0700% 0.1300% STREET KANAKANAK HOSPITAL P O BOX 130 DILLINGHAM AK 99576 Not Assessed Not Assessed Not Assessed Not Assessed 2500 SOUTH MAT-SU REGIONAL MEDICAL CENTER WOODWORT PALMER AK 99645 0.100% 0.0100% 0.9200% 0.4800% H LOOP 222 MT EDGECUMBE HOSPITAL SITKA AK 99835 0% 0% 0% 0% TONGASS DR 1000 GREG KRUSCHEK NORTON SOUND REGIONAL HOSPITAL NOME AK 99762 Not Assessed Not Assessed Not Assessed Not Assessed AVENUE (P O BOX 966) 3100 PEACEHEALTH KETCHIKAN MEDICAL CENTER TONGASS KETCHIKAN AK 99901 Not Assessed Not Assessed Not Assessed Not Assessed AVENUE PETERSBURG MEDICAL CENTER PO BOX 589 PETERSBURG AK 99833 Not Assessed Not Assessed Not Assessed Not Assessed PROVIDENCE ALASKA MEDICAL CENTER BOX 196604 ANCHORAGE AK 99508 0% 0% 0% 0.1200% 1915 EAST PROVIDENCE KODIAK ISLAND MEDICAL CTR REZANOF KODIAK AK 99615 Not Assessed Not Assessed Not Assessed -

ARIZONA FAH MEMBER FACILITIES Federation of American Hospitals Represents America’S Tax-Paying Community Hospitals and SENATE Health Systems
ARIZONA FAH MEMBER FACILITIES Federation of American Hospitals represents America’s tax-paying community hospitals and SENATE health systems. Sen. Mark Kelly (D) Sen. Kyrsten Sinema (D) HOUSE (Click name to view the district) Rep. Tom O’Halleran (D) / Arizona 1st Rep. Ann Kirkpatrick (D) / Arizona 2nd Rep. Raúl Grijalva (D) / Arizona 3rd Rep. Paul Gosar (R) / Arizona 4th Rep. Andy Biggs (R) / Arizona 5th Rep. David Schweikert (R) / Arizona 6th TOTAL Rep. Ruben Gallego (D) / Arizona 7th FACILITIES Rep. Debbie Lesko (R) / Arizona 8th Rep. Greg Stanton (D) / Arizona 9th 25 TOTAL HOSPITAL BEDS 3,482 TOTAL EMPLOYEES 13,145 FEDERATION OF AMERICAN HOSPITALS® 750 9th Street, N.W. Suite 600, Washington, DC 20001 fah.org ARIZONA FAH MEMBER FACILITIES Beds Employees REP. TOM O'HALLERAN (D) / ARIZONA 1ST 1 HOSPITAL Oro Valley Hospital Oro Valley Community Health Systems 144 612 REP. ANN KIRKPATRICK (D) / ARIZONA 2ND 6 HOSPITALS Canyon Vista Medical Center Sierra Vista LifePoint Health 100 779 Carondelet St. Joseph’s Hospital Tucson Tenet Healthcare Corporation 486 1,451 Encompass Health Rehabilitation Hospital of Northwest Tucson Encompass Health 60 171 Tucson Encompass Health Rehabilitation Institute of Tucson Tucson Encompass Health 80 241 Northwest Medical Center Tucson Community Health Systems 300 1,696 Palo Verde Hospital Tucson Universal Health Services, Inc. 84 200 REP. RAÚL GRIJALVA (D) / ARIZONA 3RD 3 HOSPITALS Carondelet Holy Cross Hospital Nogales Tenet Healthcare Corporation 25 174 Carondelet St. Mary’s Hospital Tucson Tenet Healthcare Corporation 400 1,407 Yuma Rehabilitation Hospital, a Partnership of Encompass Yuma Encompass Health 51 163 Health & YRMC REP. -

Hospital Centers of Excellence (Coe)
HOSPITAL CENTERS OF EXCELLENCE (COE) Cigna Health Care – National Centers of Excellence by state and MSA Report 2018–2019 States in blue represent where these COE hospitals WA MT ME are located. ND OR MN VT ID NH SD WI NY MA WY MI CT RI NE IA PA NJ NV OH IN MD IL DE UT CO WV DC CA KS MO VA KY NC TN AZ OK NM AR SC NEW MEXICO GA MS AL LA + TX AK TEX FL HI HI Report as of 01/09/19 and is subject to change. Please see the myCigna.com provider directory for the most current listing and look for the COE icon. Center of Excellence 904780 b 02/19 Metropolitan State Hospital Name Statistical Area Abdominal Hysterectomy Surgery Bariatric Conditions Cancer and Cath Cardiac Angioplasty Surgery Colon Deliveries Laparoscopic Gallbladder Removal Heart Surgery Joint Replacement Orthopedic Back Surgery Pulmonology Medical Total Grand AK Anchorage, AK ALASka NATIVE MEDICAL CENTER X 1 AL Albertville, AL MARSHALL MEDICAL CENTER NORTH X 1 MARSHALL MEDICAL CENTER SOUTH X 1 Alexander City, AL RUSSELL HOSPITAL X X 2 RUSSELL MEDICAL CENTER X X 2 Anniston-Oxford, AL NORTHEAST ALABAMA REGIONAL MEDICAL CENTER X X 2 Auburn-Opelika, AL EAST ALABAMA MEDICAL CENTER X X 2 Birmingham-Hoover, AL GRANDVIEW MEDICAL CENTER X X 2 ST. VINCENt’s BIRMINGHAM X 1 ST. VINCENt’s EAST X X 2 Columbus, GA-AL JACK HUGHSTON MEMORIAL HOSPITAL X 1 Cullman, AL CULLMAN REGIONAL MEDICAL CENTER X 1 Daphne-Fairhope-Foley, AL THOMAS HOSPITAL X X 2 Decatur, AL DECATUR MORGAN HOSPITAL X X X 3 Dothan, AL FLOWERS HOSPITAL X 1 Florence-Muscle Shoals, AL HELEN KELLER HOSPITAL X 1 Mobile, AL MOBILE INFIRMARY MEDICAL CENTER X 1 PROVIDENCE HOSPITAL X X X 3 SPRINGHILL MEMORIAL HOSPITAL X X X 3 Montgomery, AL COMMUNITY HOSPITAL INC. -

Tenet Healthcare Corporation Annual Report 2020
Tenet Healthcare Corporation Annual Report 2020 Form 10-K (NYSE:THC) Published: February 24th, 2020 PDF generated by stocklight.com UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, DC 20549 Form 10-K ☒ Annual report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the fiscal year endedD ecember 31, 2019 OR ☐ Transition report pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 for the transition period from to Commission File Number 1-7293 ________________________________________ TENET HEALTHCARE CORPORATION (Exact name of Registrant as specified in its charter) Nevada 95-2557091 (State of Incorporation) (IRS Employer Identification No.) 14201 Dallas Parkway Dallas, TX 75254 (Address of principal executive offices, including zip code) (469) 893-2200 (Registrant’s telephone number, including area code) ________________________________________________________ Securities registered pursuant to Section 12(b) of the Act: Title of each class Trading symbol Name of each exchange on which registered Common stock, $0.05 par value THC New York Stock Exchange 6.875% Senior Notes due 2031 THC31 New York Stock Exchange Securities registered pursuant to Section 12(g) of the Act: None ________________________________________________________ Indicate by check mark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes x No ¨ Indicate by check mark if the Registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No x Indicate by check mark whether the Registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months, and (2) has been subject to such filing requirements for the past 90 days.