Page 1 of 4 Drug Information Group 8/10/2009
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Federal Register/Vol. 79, No. 39/Thursday, February 27, 2014/Rules and Regulations
Federal Register / Vol. 79, No. 39 / Thursday, February 27, 2014 / Rules and Regulations 10985 (2) Turkeys— Combination in Zoalene in grams/ton grams per ton Indications for use Limitations Sponsor (i) 113.5 to 170.3 ..... ................................. Growing turkeys: For prevention and con- Feed continuously as sole ration. For tur- 054771 trol of coccidiosis. keys grown for meat purposes only. Do not feed to laying birds. (ii) 113.5 to 170.3 .... Bacitracin methylene Growing turkeys: For prevention and con- Feed continuously as sole ration until 14 054771 disalicylate 4 to 50. trol of coccidiosis; and for increased to 16 weeks of age. For turkeys grown rate of weight gain and improved feed for meat purposes only. Do not feed to efficiency. laying birds. Dated: February 3, 2014. Legal Authority initiated by the Attorney General (1) on Bernadette Dunham, The DEA implements and enforces his own motion; (2) at the request of the Director, Center for Veterinary Medicine. titles II and III of the Comprehensive Secretary of the Department of Health 1 [FR Doc. 2014–02617 Filed 2–26–14; 8:45 am] Drug Abuse Prevention and Control Act and Human Services (HHS), or (3) on the petition of any interested party. 21 BILLING CODE 4160–01–P of 1970, as amended. Titles II and III are referred to as the ‘‘Controlled U.S.C. 811(a). This action is based on a Substances Act’’ and the ‘‘Controlled recommendation from the Assistant DEPARTMENT OF JUSTICE Substances Import and Export Act,’’ Secretary of the HHS and on an respectively, and are collectively evaluation of all other relevant data by Drug Enforcement Administration referred to as the ‘‘Controlled the DEA. -

22-244 Biopharmaceutics Review(S)
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 22-244 CLINICAL PHARMACOLOGY AND BIOPHARMACEUTICS REVIEW(S) DEP\RT\IE.'\T OF IIEALTH .\ '\ D Clinical Pharmacology & Biopharmaceutics IH\L\!\ SER\ICES PI HUC IIE\LTH SERVICE (HFD 870) FOOD\'\D DRIG .-\D\""ISTR\TION Tracl"ingl Action Sheet foi' Foi'malllnformai Consults . Iniiii: \rikdllih C. '\dll.lIi_ I'h.I), To: DOCl'\'IENT ROOi\l (LOG-IN and LOC-OlT) Please log-in this consult and review action for the specified IND/NDA submission 1); I I.: II I X::I)I)X ~;\~) :\u.: ND.\ :\u. :::: - ::-1-1 I),\TI 01 DOel "II.NT IIJ' 1:1/::()IJX Sni.11 :\u.: IV-IJIJIJ Class I Resuhiiission '\.\\11.01 imi(, l'I~IORln (()'\ \11)1 R\II ()'\ J).lIC ui' illl,)lli.il.;lmlldl I IJ I Y::()IJX I LlCEDR.\ (Fospropofol) Standanl (ulisLlli: Injection I 1111 :\/\\11 01 \I'O'\\OR: I \1(;1 Pharma I TYPE OF SL InIiSSIO,\ CLI'\I( .\L PIIARMACOI,O(;YIBIOPIL\R\L\CEITlCS RELATED ISSUE o I'I~I.-I:\I) 0 1)IS\OI.11 IO:\I:\-\III~O 1~1I.1 ..\SI. 0 IIN/\1. I'RI1\III) 1..\131 1.1:\( , 0\:\1\ 1\111' III \1\:\ \(\1 IN(i o 1311h \1\11./\131111 Y \ 1(1)11\ ~ L\l31I1NCi RI. VISIO'\ i:\-\iiim \111 ,\HI)I 0 1\\1 0 I "i - \ I \ 0 \\\ I \ I J( i~ Ii)l lSi o (ORRI\I)ONI)IMî o I'R()lI)(.I)1 o Si '1)\( I~II\TII) 0 IWI.(j /\I)VIRTI\I:\( j 01'11\\1. -

Intravenous Anesthetics a Drug That Induces Reversible Anesthesia the State of Loss of Sensations, Or Awareness
DR.MED. ABDELKARIM ALOWEIDI AL-ABBADI ASSOCIATE PROF. FACULTY OF MEDICINE THE UNIVERSITY OF JORDAN Goals of General Anesthesia Hypnosis (unconsciousness) Amnesia Analgesia Immobility/decreased muscle tone (relaxation of skeletal muscle) Reduction of certain autonomic reflexes (gag reflex, tachycardia, vasoconstriction) Intravenous Anesthetics A drug that induces reversible anesthesia The state of loss of sensations, or awareness. Either stimulates an inhibitory neuron, or inhibits an excitatory neuron. Organs are divided according to blood perfusion: High- perfusion organs (vessel-rich); brain takes up disproportionately large amount of drug compared to less perfused areas (muscles, fat, and vessel-poor groups). After IV injection, vessel-rich group takes most of the available drug Drugs bound to plasma proteins are unavailable for uptake by an organ After highly perfused organs are saturated during initial distribution, the greater mass of the less perfused organs continue to take up drug from the bloodstream. As plasma concentration falls, some drug leaves the highly perfused organs to maintain equilibrium. This redistribution from the vessel-rich group is responsible for termination of effect of many anesthetic drugs. Compartment Model Inhibitory channels : GABA-A channels ( the main inhibitory receptor). Glycine channels. Excitatory channels : Neuronal nicotic. NMDA. Rapid onset (mainly unionized at physiological pH) High lipid solubility Rapid recovery, no accumulation during prolonged infusion Analgesic -

124.210 Schedule IV — Substances Included. 1
1 CONTROLLED SUBSTANCES, §124.210 124.210 Schedule IV — substances included. 1. Schedule IV shall consist of the drugs and other substances, by whatever official name, common or usual name, chemical name, or brand name designated, listed in this section. 2. Narcotic drugs. Unless specifically excepted or unless listed in another schedule, any material, compound, mixture, or preparation containing any of the following narcotic drugs, or their salts calculated as the free anhydrous base or alkaloid, in limited quantities as set forth below: a. Not more than one milligram of difenoxin and not less than twenty-five micrograms of atropine sulfate per dosage unit. b. Dextropropoxyphene (alpha-(+)-4-dimethylamino-1,2-diphenyl-3-methyl-2- propionoxybutane). c. 2-[(dimethylamino)methyl]-1-(3-methoxyphenyl)cyclohexanol, its salts, optical and geometric isomers and salts of these isomers (including tramadol). 3. Depressants. Unless specifically excepted or unless listed in another schedule, any material, compound, mixture, or preparation which contains any quantity of the following substances, including its salts, isomers, and salts of isomers whenever the existence of such salts, isomers, and salts of isomers is possible within the specific chemical designation: a. Alprazolam. b. Barbital. c. Bromazepam. d. Camazepam. e. Carisoprodol. f. Chloral betaine. g. Chloral hydrate. h. Chlordiazepoxide. i. Clobazam. j. Clonazepam. k. Clorazepate. l. Clotiazepam. m. Cloxazolam. n. Delorazepam. o. Diazepam. p. Dichloralphenazone. q. Estazolam. r. Ethchlorvynol. s. Ethinamate. t. Ethyl Loflazepate. u. Fludiazepam. v. Flunitrazepam. w. Flurazepam. x. Halazepam. y. Haloxazolam. z. Ketazolam. aa. Loprazolam. ab. Lorazepam. ac. Lormetazepam. ad. Mebutamate. ae. Medazepam. af. Meprobamate. ag. Methohexital. ah. Methylphenobarbital (mephobarbital). -

A Phase 3 Randomized, Double-Blind, Dose-Contro
Clinical Review Lex Schultheis M.D., Ph.D. NDA 22-244 (000) Fospropofol Disodium Injection 10.1.3 Protocol 3000-524 A dose-controlled study in bronchoscopy patients Title: A Phase 3 randomized, double-blind, dose-controlled study to assess the efficacy and safety ofFospropofol (fospropofol disodium) injection for minimal-to-moderate sedation in patients undergoing flexible bronchoscopy Indication: minimal-to-moderate sedation Objectives: 1. demonstrate that Fospropofol is effective in providing minimal-to-moderate sedation 2. demonstrate clinical benefit of Fospropofol to patients 3. Evaluate safety ofFospropofol Study Design: Patients are to be administered 50 mcg offentanyl intravenously before beginning the procedure and before administering sedation. One additional dose of25 mcg of fentanyl may be administered after an interval of 10 minutes if the patient appears to be in pain. Randomized, double-blinded, dose-control with patients assigned 1: 1 to one of two initial sedation doses ofFospropofol: either 2 mg/kg (range 120 mg to 180 mg) or 6.5 mg/kg (range 390 to 585 mg). The initial dose offospropofol is to be administered 5 minutes after administration of the initial dose of fentanyl. The initial dose ofFospropofol and up to two additional supplemental doses may be administered at four minute intervals to achieve an OAA/S score of not more than 4/5. The supplemental doses ofFospropofol are 0.5 mg/kg (range 30-45 mg) for the patients treated with an initial dose of2 mg/kg and 1.63 mg/kg (range 97.5-146 mg) for patients treated with an initial dose of 6.5 mg/kg. -
![Chapter 329 [New] Uniform Controlled Substances Act](https://docslib.b-cdn.net/cover/1442/chapter-329-new-uniform-controlled-substances-act-1221442.webp)
Chapter 329 [New] Uniform Controlled Substances Act
CHAPTER 329 [NEW] UNIFORM CONTROLLED SUBSTANCES ACT Part I. General Provisions Section 329-1 Definitions 329-2 Hawaii advisory commission on drug abuse and controlled substances; number; appointment 329-3 Annual report 329-4 Duties of the commission Part II. Standards and Schedules 329-11 Authority to schedule controlled substances 329-12 Nomenclature 329-13 Schedule I tests 329-14 Schedule I 329-15 Schedule II tests 329-16 Schedule II 329-17 Schedule III Tests 329-18 Schedule III 329-19 Schedule IV tests 329-20 Schedule IV 329-21 Schedule V tests 329-22 Schedule V 329-23 Republishing and distribution of schedules Part III. Regulation of Manufacture, Distribution, Prescription, and Dispensing of Controlled Substances 329-31 Rules 329-31.5 Clinics 329-32 Registration requirements 329-33 Registration 329-34 Revocation and suspension of registration 329-35 Order to show cause 329-36 Records of registrants 329-37 Filing requirements 329-38 Prescriptions 329-39 Labels 329-40 Methadone treatment programs Part IV. Offenses and Penalties 329-41 Prohibited acts B-penalties 329-42 Prohibited acts C-penalties 329-43 Penalties under other laws 329-43.5 Prohibited acts related to drug paraphernalia Amended 0612 1 329-44 Notice of conviction to be sent to licensing board, department of commerce and consumer affairs 329-45 Repealed 329-46 Prohibited acts related to visits to more than one practitioner to obtain controlled substance prescriptions 329-49 Administrative penalties 329-50 Injunctive relief Part V. Enforcement and Administrative Provisions 329-51 Powers of enforcement personnel 329-52 Administrative inspections 329-53 Injunctions 329-54 Cooperative arrangements and confidentiality 329-55 Forfeitures 329-56 Burden of proof; liabilities 329-57 Judicial review 329-58 Education and research 329-59 Controlled substance registration revolving fund; established Part VI. -

Bolus-Dose Fospropofol Disodium (Lusedra®)
a & hesi C st lin e ic n a A l f R o e l s Journal of Anesthesia & Clinical e a a n r r c u h o Leslie et al., J Anesth Clin Res 2015, 6:8 J ISSN: 2155-6148 Research DOI: 10.4172/2155-6148.1000552 Research Article Open Access Bolus-Dose Fospropofol Disodium (Lusedra®): Is 10 mg/Kg Superior To 6.5 mg/Kg for Sedation in Patients Undergoing Regional Anesthesia Blocks Prior to Orthopedic Surgery? John B Leslie1*, Terrence L Trentman1, Lopa Misra1, David M Rosenfeld1, David P Seamans1, Renee E Caswell1, André R Watkins1, Joseph G Hentz1 and Ryan Buckley2 1Mayo Medical School – Phoenix Campus, Mayo Clinic Arizona, Scottsdale, Arizona, USA 2University of Arizona School of Medicine – Tucson Campus, Tucson, Arizona, USA *Corresponding author: John B Leslie, MD, MBA, Department of Anesthesiology, Mayo Clinic Hospital; 5777 East Mayo Boulevard, Phoenix, AZ 85054-4502, USA, Tel: 480-342-1800; Fax: 480-342-2319; E-mail: [email protected] Received date: February 27, 2015, Accepted date: August 11, 2015, Published date: August 18, 2015 Copyright: © 2015 Leslie JB, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Objective: Fospropofol disodium (Lusedra®) is a pro-drug propofol for Monitored Anesthesia Care. The FDA- approved dose regimen is minimally effective with a slow onset often requiring supplemental doses at 4 minutes to achieve adequate sedation and frequently requires early re-dosing. -

Capítulo 30 Anestesia Intravenosa
Capítulo 30 Anestesia intravenosa JAAP VUYK • ELSKE SITSEN • MARIJE REEKERS Agradecimientos. Los redactores y el editor desean agradecer a los Dres. J. G. Reves, Peter Glass, David A. Lubarsky, Matthew D. McEvoy y Ricardo Martinez-Ruiz la aportación de un capítulo sobre el mismo tema en la edición previa de este tratado, que ha servido de base para el presente capítulo. P UNTOS CLAVE • La introducción de tiopental en la práctica clínica en 1934 supuso el comienzo de la era de la anestesia intravenosa (i.v.) moderna. Hoy en día, los anestésicos i.v. forman parte de la inducción y el mantenimiento de la anestesia y la sedación en un amplio abanico de situaciones. • El anestésico i.v. más utilizado es el propofol, un alquilfenol formulado en emulsión lipídica. Se trata de un fármaco que ofrece rapidez de inicio y finalización de acción, así como tiempos decrecientes concordantes con el contexto de unos 10 min en infusiones de duración menor de 3 h e inferior a 40 min en aquellas de hasta 8 h. Su mecanismo de acción podría corresponder a la potenciación de las corrientes de cloro inducidas por el ácido g-aminobutírico (GABA). El propofol induce una disminución dependiente de la dosis de la presión arterial media por sendas reducciones del gasto cardíaco y la resistencia vascular periférica, y ocasiona una depresión respiratoria moderada. El efecto antiemético constituye un rasgo exclusivo de este compuesto incluso a concentraciones menores de las que producen sedación. • Los barbitúricos constituían los fármacos i.v. más utilizados en la inducción de la anestesia con anterioridad a la introducción del propofol. -

Recent Advances in Intravenous Anesthesia and Anesthetics
Recent advances in intravenous anesthesia and anesthetics The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Mahmoud, Mohamed, and Keira P. Mason. 2018. “Recent advances in intravenous anesthesia and anesthetics.” F1000Research 7 (1): F1000 Faculty Rev-470. doi:10.12688/f1000research.13357.1. http:// dx.doi.org/10.12688/f1000research.13357.1. Published Version doi:10.12688/f1000research.13357.1 Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:37160088 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA F1000Research 2018, 7(F1000 Faculty Rev):470 Last updated: 17 APR 2018 REVIEW Recent advances in intravenous anesthesia and anesthetics [version 1; referees: 2 approved] Mohamed Mahmoud1, Keira P. Mason 2 1Department of Anesthesiology, Cincinnati Children’s Hospital Medical Center, University of Cincinnati, 3333 Burnet Avenue, Cincinnati, OH, 45229, USA 2Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children’s Hospital and Harvard Medical School, 300 Longwood Avenue, Boston, MA, 02115, USA First published: 17 Apr 2018, 7(F1000 Faculty Rev):470 (doi: Open Peer Review v1 10.12688/f1000research.13357.1) Latest published: 17 Apr 2018, 7(F1000 Faculty Rev):470 (doi: 10.12688/f1000research.13357.1) Referee Status: Abstract Invited Referees Anesthesiology, as a field, has made promising advances in the discovery of 1 2 novel, safe, effective, and efficient methods to deliver care. -

Chapter 8 Intravenous Anesthetics Which Accounts for Their Rapid Onset of Action
Chapter INTRAVENOUS 8 ANESTHETICS Michael P. Bokoch and Helge Eilers PROPOFOL Physicochemical Characteristics Pharmacokinetics Pharmacodynamics Intravenous nonopioid anesthetics have an important Clinical Uses role in modern anesthesia practice (Box 8.1).1-7 They are widely used to facilitate a rapid induction of gen- FOSPROPOFOL eral anesthesia and provide sedation during monitored Physicochemical Characteristics anesthesia care (MAC) and for patients in intensive care Pharmacokinetics settings (also see Chapter 41). With the introduction of Pharmacodynamics propofol, intravenous techniques are increasingly being Clinical Uses used for maintenance of anesthesia. However, similar to BARBITURATES inhaled anesthetics, the currently available intravenous Physicochemical Characteristics drugs do not produce only desirable effects (hypnosis, Pharmacokinetics amnesia, analgesia, immobility). Therefore, the concept Pharmacodynamics of “balanced anesthesia” evolved by using smaller doses Side Effects of multiple drugs rather than using larger doses with one Clinical Uses or two drugs. The fundamental drugs used with “balanced anesthesia” include inhaled anesthetics, sedative/hypnot- BENZODIAZEPINES ics, opioids, and neuromuscular blocking drugs (also see Physicochemical Characteristics Chapters 7, 9, and 11). Pharmacokinetics The intravenous anesthetics used for induction of gen- Pharmacodynamics eral anesthesia are lipophilic and preferentially partition Side Effects into highly perfused lipid-rich tissues (brain, spinal cord), Clinical Uses -
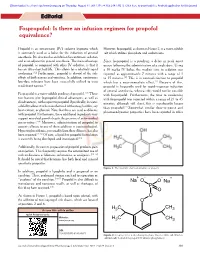
Fospropofol: Is There an Infusion Regimen for Propofol Equivalence?
[Downloaded free from http://www.joacp.org on Thursday, August 11, 2011, IP: 74.105.214.131] || Click here to download free Android application for this journal Editorial Fospropofol: Is there an infusion regimen for propofol equivalence? Propofol is an intravenous (IV) sedative hypnotic which However, fospropofol, as shown in Figure 2, is a water-soluble is commonly used as a bolus for the induction of general salt which utilizes phosphate and sodium ions. anesthesia. It is also used as an infusion for continuous sedation and as an adjunct for general anesthesia. The main advantage Since fospropofol is a prodrug, a delay in peak onset of propofol, as compared with other IV sedatives, is that it occurs following the administration of a single dose. Using has an ultra-short half-life. This allows for a relatively rapid a 10 mg/kg IV bolus, the median time to sedation was awakening.[1,2] Furthermore, propofol is devoid of the side reported as approximately 7 minutes with a range of 1 effects of both nausea and vomiting. In addition, continuous to 15 minutes.[4] This is in contradistinction to propofol low-dose infusions have been successfully utilized to treat which has a near-immediate effect.[2] Because of this, recalcitrant nausea.[3] propofol is frequently used for rapid-sequence induction of general anesthesia, whereas this would not be possible [4,5] Fospropofol is a water-soluble prodrug of propofol. These with fospropofol. Furthermore, the time to awakening two features give fospropofol clinical advantages, as well as with fospropofol was reported within a range of 21 to 45 disadvantages, with respect to propofol. -

Laws 2021, LB236, § 4
LB236 LB236 2021 2021 LEGISLATIVE BILL 236 Approved by the Governor May 26, 2021 Introduced by Brewer, 43; Clements, 2; Erdman, 47; Slama, 1; Lindstrom, 18; Murman, 38; Halloran, 33; Hansen, B., 16; McDonnell, 5; Briese, 41; Lowe, 37; Groene, 42; Sanders, 45; Bostelman, 23; Albrecht, 17; Dorn, 30; Linehan, 39; Friesen, 34; Aguilar, 35; Gragert, 40; Kolterman, 24; Williams, 36; Brandt, 32. A BILL FOR AN ACT relating to law; to amend sections 28-1202 and 69-2436, Reissue Revised Statutes of Nebraska, and sections 28-401 and 28-405, Revised Statutes Cumulative Supplement, 2020; to redefine terms, change drug schedules, and adopt federal drug provisions under the Uniform Controlled Substances Act; to provide an exception to the offense of carrying a concealed weapon as prescribed; to define a term; to change provisions relating to renewal of a permit to carry a concealed handgun; to provide a duty for the Nebraska State Patrol; to eliminate an obsolete provision; to harmonize provisions; and to repeal the original sections. Be it enacted by the people of the State of Nebraska, Section 1. Section 28-401, Revised Statutes Cumulative Supplement, 2020, is amended to read: 28-401 As used in the Uniform Controlled Substances Act, unless the context otherwise requires: (1) Administer means to directly apply a controlled substance by injection, inhalation, ingestion, or any other means to the body of a patient or research subject; (2) Agent means an authorized person who acts on behalf of or at the direction of another person but does not include a common or contract carrier, public warehouse keeper, or employee of a carrier or warehouse keeper; (3) Administration means the Drug Enforcement Administration of the United States Department of Justice; (4) Controlled substance means a drug, biological, substance, or immediate precursor in Schedules I through V of section 28-405.