Board of Directors 25 November 2015
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

USEFUL WEALDEN TELEPHONE Nos
FREE SMOKE ALARMS Published jointly by St Thomas à Becket Church Your local Fire Service personnel are happy to make an and Framfield Parish Council appointment to visit your home and discuss fire safety issues that are specific to you. They will also ensure that you have working smoke alarm(s) within your home and where you do not, they will supply and fit 10 year smoke alarms. To request a FREE visit call 0800 1777 069 (call is free). USEFUL WEALDEN TELEPHONE NOs. General Enquiries: 01273 481000 Adult Education: 01273 481497 Bins and Recycling: 01323 443322 or 01892 653311 Education, general 01273 481000 Leisure centres, swimming pools and parks: 01323 443322 Planning, development, building control: 01323 443322 Road maintenance: 0845 6080193 Recycling sites: 01273 481000 Street Lighting: 0845 6080193 Trading standards (consumer issues): 01323 418200 Crimestoppers, report crime anonymously 0800 555111 Police, non-emergency: 0845 6070999 East Sussex Fire and Rescue Service: 0845 130 8855 Home Safety Visit Helpline: 0800 1777 069 THE ADVERTISEMENTS IN THIS MAGAZINE ARE PUBLISHED IN GOOD FAITH. THE PUBLISHERS DO NOT, F r a m f i e l d, B l a c k b o y s HOWEVER, ENDORSE ANY PRODUCTS OR SERVICES and SPECIFIED P a l e h o u s e C o m m o n O C T O B E R / N O V E M B E R 2 0 0 9 - 32 - HOW TO GET IN TOUCH WITH YOUR LOCAL CHURCH WHO'S WHO AT THE St THOMAS À BECKET NEWSLETTER Priest-in-Charge : Revd Chris Lawrence 01825 891090 (after hours 01825 890365) Joint Chair - For the Church: Rev. -

51 Bus Time Schedule & Line Route
51 bus time schedule & line map 51 Eastbourne - Heathƒeld View In Website Mode The 51 bus line (Eastbourne - Heathƒeld) has 5 routes. For regular weekdays, their operation hours are: (1) Eastbourne Town Centre: 5:46 AM - 10:44 PM (2) Hailsham: 2:23 PM - 11:10 PM (3) Heathƒeld: 6:52 AM - 6:28 PM (4) Hellingly: 7:38 AM (5) Roselands: 5:20 PM Use the Moovit App to ƒnd the closest 51 bus station near you and ƒnd out when is the next 51 bus arriving. Direction: Eastbourne Town Centre 51 bus Time Schedule 61 stops Eastbourne Town Centre Route Timetable: VIEW LINE SCHEDULE Sunday 8:40 AM - 9:44 PM Monday 5:46 AM - 10:44 PM Streatƒeld Road, Heathƒeld 80 High Street, Heathƒeld And Waldron Civil Parish Tuesday 5:46 AM - 10:44 PM Marshlands Lane, Heathƒeld Wednesday 5:46 AM - 10:44 PM Downsview, Heathƒeld Thursday 5:46 AM - 10:44 PM Friday 5:46 AM - 10:44 PM Collingwood Avenue, Heathƒeld Saturday 6:39 AM - 10:44 PM The Heathƒeld Tavern, Heathƒeld Holly Drive, Heathƒeld Sandy Cross Lane, Sandy Cross 51 bus Info Direction: Eastbourne Town Centre Runt In Tun, Maynard's Green Stops: 61 Trip Duration: 60 min West Street Lane, Maynard's Green Line Summary: Streatƒeld Road, Heathƒeld, Marshlands Lane, Heathƒeld, Downsview, Heathƒeld, Collingwood Avenue, Heathƒeld, The Heathƒeld Primary School, Maynard's Green Tavern, Heathƒeld, Holly Drive, Heathƒeld, Sandy Cross Lane, Sandy Cross, Runt In Tun, Maynard's Vines Cross Road, Horam Green, West Street Lane, Maynard's Green, Primary School, Maynard's Green, Vines Cross Road, Horam, Merrydown Village, Horam Merrydown -

Parcel 1, Hellingly, Hailsham, East Sussex
GRM Development Solutions GRM Development Solutions Laurus House 14 Garden Court First Avenue Tewin Road Centrum 100 Welwyn Garden City Burton upon Trent Hertfordshire, AL7 1BH Staffordshire, DE14 2WH www.grm-uk.com e. [email protected] t. 01283 551249 t. 01707 830213 PARCEL 1, HELLINGLY, HAILSHAM, EAST SUSSEX PHASE 1 SITE APPRAISAL (DESK STUDY) FOR CATESBY ESTATES PLC Project Ref: P9009 Date: July 2019 Prepared for: Catesby Estates Plc Catesby House 5B Tournament Court Edgehill Drive, Warwick Warwickshire CV34 6LG This report has been prepared in accordance with GRM’s Accredited Quality Procedures. If you have any queries regarding this report please contact the project manager in the first instance. Prepared by: Reviewed by: Approved by: Project Manager Sonia Singh George Salloway Siobhan Jackson Chris Jerram BSc (Hons), FGS BSc (Hons) MSc MIEnvSc BSc (Hons) MIEnvSc CGeol FGS (Engineering Geologist) (Acting Senior Geo- (Principal Geo-environmental (Consultant) environmental Engineer) Scientist) [email protected] george.salloway@grm- [email protected] [email protected] uk.com When required in-house geological, geotechnical, environmental, structural and civil staff helped to produce this document. Issue Description of Revision Signature Amended Appendix; missing parcel I Revision A GS information [email protected] www.grm-uk.com GRM/P9009/DS.1.RevA GRM is a trading name of GRM Development Solutions Limited [email protected] www.grm-uk.com TABLE OF CONTENTS 1 INTRODUCTION ...................................................................................................... 1 2 PHASE I DESK STUDY AND SITE OBSERVATIONS ............................................ 2 3 PHASE I CONCEPTUAL SITE MODEL................................................................. 11 4 CONTAMINATION / REMEDIATION RECOMMENDATIONS ............................... 12 5 PRELIMINARY GEOTECHNICAL ASSESSMENT ............................................... -
Cuckoo Trail & Low Weald Circular
eastsussex.gov.uk 1 Cycling in East Sussex: Avenue Verte Route Guide Cuckoo Trail & Low Weald circular As an alternative to the roller coaster with fine views of the South Downs. roads of the High Weald, try this The land is a mixture of lush pasture delightful ride. It follows the flatter and arable fields, surrounded by lanes to the west of the Cuckoo Trail hedgerows and verges filled with wild and the toughest climb is only 55 flowers. Lovely old houses can be metres – a small challenge compared glimpsed at every turn of the road. to some of the other rides. Golden Cross – Polegate Polegate – Arlington Reservoir Take care crossing the busy A22 at Make your way from Polegate north- Golden Cross and rejoin the network west towards Abbot’s Wood and of quiet lanes through Chiddingly follow the bridleway on a mixture of with the impressive Chiddingly Place surfaces – at times it is a wonderful at the far end of the hamlet. Through smooth, stone-based track and at Stonehill, the route leads back to others it can be muddy after wet Horam on the A267. A gentle descent weather. Before long you are on the on the wonderful Cuckoo Trail south lane network which leads into the of Horam under a canopy of trees, village of Arlington. Shortly after takes you through Hailsham back crossing the Cuckmere River, keep to Polegate and the starting point. an eye out for the bridleway to the right that takes you past Arlington Places of Interest → Reservoir and onto Station Road, Cuckoo Trail: Wildlife Art Trail Lying to north of Berwick. -

Hellingly. Horse Bridge
224S HELLINGLY AND HORSEBRIDGE. SUSSEX. ' . 6 fine-toned bells and a clock with dial, added in 1886 as a pasture land and for the production of pottery-ware and a memorial to the late Earl of Chichester: the chapel has bricks; on this formation the district called "the Dicker," a fine Norman arcade, and it\ the chancel and other parts of which lies partly in this and partly in the adjoining parishes the church interesting remains of the older church are in- of Chiddingly and Arlington, is situated, and will be found corporated: in the south aisle is a window to tM Rev. John described under a separate heading. Here is a chalybeate Olive A.:r.r. 35 years vicar of the parish, and a memorial door spring. The soil is light clay; subsoil, dark gravel. The of oak to Margaret, his wife, opens into the church on the chief crops are wheat and oats. The area is 6,oso acres ; north side: the structure was thoroughly restored and re- rateable value, £6,702; the population in 1881 was 11 646, seated in 1869, and has 700 sittings. The register dates ihcluding 127 officers and inmates in the Hailsham work from the year 1618. The living is a vicarage, average tithe house. rent-charge £3o8, gross yearly value £300, with residence HOREHAM ROAD, partly in this parish, is given under a and 5 acres of glebe, in the gift of the Earl of Chichester, separate heading. and held since 1882 by the Rev. James Farrar M.A. of Sexton, George Horton. -

Winkenhurst Manor NORTH STREET • HELLINGLY • EAST SUSSEX
Winkenhurst Manor NORTH STREET • HELLINGLY • EAST SUSSEX Winkenhurst Manor NORTH STREET • HELLINGLY • EAST SUSSEX • BN27 4EB A stunning Grade II* listed Georgian country house with elegant secondary accommodation. The Manor House Entrance lobby • Drawing Room • Sitting Room • Kitchen/breakfast room Orangery • Guest cloakroom • WC Master bedroom with en-suite bathroom and dressing room • Guest bedroom suite 2 further bedrooms • Office/bedroom 5 • Family bathroom Spacious cellar with laundry room, boot room, boiler room, china room and further storage The Stables Sitting Room • Kitchen/Breakfast Room • Cloakroom • 2 bedroom suites Outbuildings housing a gym, cinema room and additional storage • Large garage Garden and grounds extending to approximately 4 acres Horam 1.75 miles • Heathfield 3 miles • Polegate mainline station 6 miles (London Victoria 80 minutes) Stonegate mainline station 11 miles (London Bridge from 62 minutes) Eastbourne 10 miles • Tunbridge Wells 19 miles • (All distances are approximate) These particulars are intended only as a guide and must not be relied upon as statements of fact. Your attention is drawn to the Important Notice on the last page of the text. Location • Winkenhurst Manor is located on the outskirts of the village of Hellingly in the rolling Sussex countryside. • Horam, just 1.75 miles away, has a selection of local amenities with more comprehensive shops and services being found in Heathfield 3 miles away. • Royal Tunbridge Wells is within easy striking distance offering a further comprehensive range of shopping, recreational and cultural amenities. • Communications in the area are very good. The property has access to major road and rail routes. Main line station at Polegate offers regular services to the capital, taking approximately 80 minutes. -

Notice-Of-Poll-Wealden.Pdf
NOTICE OF POLL East Sussex County Council – Wealden Electoral Divisions Election of a County Councillor for Arlington, East Hoathly & Hellingly Notice is hereby given that: 1. A poll for the election of a County Councillor for Arlington, East Hoathly & Hellingly will be held on Thursday 6 May 2021, between the hours of 7:00 am and 10:00 pm. 2. The number of County Councillors to be elected is one. 3. The names, home addresses and descriptions of the Candidates remaining validly nominated for election and the names of all persons signing the Candidates nomination paper are as follows: Names of Signatories Name of Candidate Home Address Description (if any) Proposers(+), Seconders(++) BENNETT Quarry Cottage, Royal Oak Lane, High The Conservative Party Alison J Dunbar-Dempsey Nick Hurstwood, East Sussex, TN22 4AL Candidate (+) Geoffrey C White (++) EVEREST (Address in Wealden) Reform UK Marie H Everest (+) Mark Raymond Stewart Chalmers (++) JOHNSTONE Broadhembury House, Treblers Road, Liberal Democrat Carole A Ridout (+) Beverley Ann Crowborough, East Sussex, TN6 3RL John R Ridout (++) SMITH (Address in Wealden) Labour Party Kathryn Richardson (+) Angie Paul D S Richardson (++) WILSON Church Cottage, Church Lane, Laughton, The Green Party Martin A.N. Wilson (+) Alison Jane BN8 6AH Kay G Syrad (++) 4. The situation of Polling Stations and the description of persons entitled to vote thereat are as follows: Station Ranges of electoral register numbers of Situation of Polling Station Number persons entitled to vote thereat Herstmonceux Village -

East Sussex Record Office Report of the County Archivist April 2008 to March 2009 Introduction
eastsussex.gov.uk East Sussex Record Office Report of the County Archivist April 2008 to March 2009 Introduction The year was again dominated by efforts towards achieving The Keep, the new Historical Resource Centre, but the core work of the Record Office continued more busily than ever and there was much of which to be proud. In July 2008 we took in our ten-thousandth accession, something of a milestone in the office’s own history of almost 60 years. An application to the Heritage Lottery Fund (HLF) for £4.9million towards the costs of The Keep was submitted by the Record Office on behalf of the capital partners, East Sussex County Council, Brighton & Hove City Council and the University of Sussex, in September. This represented around 20% of the anticipated costs of the building, since the partners remain committed to find the remainder. In December we learned our fate: that we had been unsuccessful. Feedback from the HLF indicated that ours had been an exemplary application, and one which they would have liked to have supported but, in a year when the effect of diverting HLF money to the Olympics was being felt, it was thought necessary to give precedence to some very high-profile projects. We were, of course, disappointed, but determined not to be deterred, and the partners agreed to pursue ways forward within the existing funding. Because it would further hold up the project, adding to inflation costs, but give no guarantee of success, we decided not to re-apply to the HLF, and by the end of the financial year were beginning to look at options for a less expensive building. -

List of Streets for Publication.Xlsx
EAST SUSSEX HIGHWAYS LIST OF CLASSIFIED ROADSLAST UPDATED OCTOBER 2018 WEALDEN DISTRICT USRN STREET LOCALITY TOWN NUMBER 42701595 ALFRISTON ROAD ALFRISTON C39 42702734 ALFRISTON ROAD BERWICK C39 42700737 ALICE BRIGHT LANE CROWBOROUGH C483 42701077 AMBERSTONE HAILSHAM A271 42703001 ARGOS HILL ROTHERFIELD A267 42703002 ARGOS HILL MAYFIELD A267 42701228 ARLINGTON ROAD EAST HAILSHAM C210 42701229 ARLINGTON ROAD WEST HAILSHAM C210 42700244 BACK LANE CROSS IN HAND HEATHFIELD C329 42700247 BACK LANE WALDRON C329 42700858 BACK LANE HALLAND C327 42702051 BACK LANE RUSHLAKE GREEN WARBLETON C16 42700420 BALACLAVA LANE WADHURST C539 42701889 BALACLAVA LANE TURNERS GREEN WADHURST C539 42701968 BALLSOCKS LANE VINES CROSS HORAM C596 42701775 BARNHORN ROAD HOOE A259 42700366 BARTLEY MILL ROAD LITTLE BAYHAM FRANT C82 42700367 BARTLEY MILL ROAD WADHURST C82 42700219 BATTLE ROAD PUNNETTS TOWN B2096 42700823 BATTLE ROAD THREE CUPS CORNER WARBLETON B2096 42701078 BATTLE ROAD HAILSHAM A295 42703023 BATTLE ROAD CHAPEL CROSS HEATHFIELD B2096 42703024 BATTLE ROAD CADE STREET HEATHFIELD B2096 42703025 BATTLE ROAD PUNNETTS TOWN HEATHFIELD B2096 42700504 BATTS BRIDGE ROAD MARESFIELD A272 42701037 BATTS BRIDGE ROAD PILTDOWN A272 42700353 BAYHAM ROAD FRANT B2169 42701688 BAYHAM ROAD BELLS YEW GREEN FRANT B2169 42701265 BAYLEYS LANE WILMINGTON C210 42702703 BEACHY HEAD ROAD EAST DEAN C37 42700595 BEACON ROAD CROWBOROUGH A26 42700770 BEACONSFIELD ROAD CHELWOOD GATE C3 42700317 BEECH GREEN LANE WITHYHAM C251 42701019 BEECHES FARM ROAD BUCKHAM HILL ISFIELD C255 42700063 -
MASTERPLAN a Programme for the Future
Hailsham &Hellingly MASTERPLAN A Programme for the Future Hailsham Town Council & Hellingly Parish Council January 2009 Hailsham & Hellingly Masterplan: A Programme for the Future ▪ Contents Contents 1. INTRODUCTION 2. ROADS 3. WATER, SEWERAGE & DRAINAGE 4. TRANSPORT 5. RETAIL 6. HAILSHAM MARKET 7. EMPLOYMENT LAND 8. HOUSING 9. HEALTHCARE 10. EDUCATION & TRAINING SKILLS 11. LEISURE, RECREATION & THE ARTS 12. APPENDIX: HAILSHAM TOWN CENTRE RETAIL CAPACITY STUDY Hailsham Town Council Hellingly Parish Council Inglenook ● Market Street ● Hailsham Village Hall ● North Street ● Hellingly East Sussex ● BN27 2AE East Sussex ● BN27 4DS T: (01323) 841702 T: (01323) 484210 F: (01323) 842978 F: (01323) 842978 [email protected] [email protected] www.hailsham-tc.gov.uk www.hellingly-pc.org.uk Hailsham & Hellingly Masterplan: A Programme for the Future ▪ Page 1 INTRODUCTION 1. Plan Objectives To provide a strategic document to guide and co-ordinate future development in the Parishes of Hailsham and Hellingly, but not to duplicate nor to seek to repeat national or regional planning policies that are to be found elsewhere To provide a document that can inform and supplement but not supplant the Wealden Local Development Framework To identify the present local infrastructure and to highlight additions, changes or upgrades that may be required to accommodate present and future developments To ensure that the needs of all sections of the community from the very young to the more senior are addressed To enhance the economic performance and potential of the area To improve the quality of life for all residents To conserve and enhance the landscape setting of the town Area Covered The parishes of Hailsham and Hellingly. -
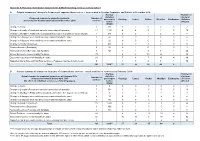
Proposed Reformulated Supported Bus Network
Appendix 6; Outcome reformulated supported bus network including services commercialised A Original summary of changes to frequency of supported bus services - as presented to Scrutiny Committee and Cabinet in December 2014: Average Number of daily bus electoral Proposed changes to supported network, Number of passengers Hastings Lewes Rother Wealden Eastbourne divisions as reported to Scrutiny and Cabinet in December 2014 services before affected RSBN Change to hourly 2 318 0 2 0 0 0 2 Change to 2 hourly off peak and maintain current days of operation 13 1351 6 4 5 1 0 19 Change to Monday to Friday school days/peak and reduce to 2 days per week off peak 4 348 0 2 1 2 0 8 Change to 2 days per week and frequency remains broadly the same 3 47 0 0 1 3 0 6 Change to 3 days per week and frequency remains broadly the same 2 22 0 0 0 2 0 4 Change to number of journeys 7 685 3 2 3 3 0 22 Removed service (Saturdays) 2 99 0 1 0 1 0 3 Removed services (Evenings and Sundays) 7 468 4 1 3 4 1 26 School Services – remain broadly the same 29 6 6 13 14 2 38 Days and frequency remain broadly the same 23 7 8 7 11 4 39 Supported Dial a Ride and Taxi Rider services – Proposed changes in table below 9 1 3 2 3 1 30 Total 101 3338** 27 29 35 44 8 B Current summary of changes to frequency of supported bus services - actual provision of services as at February 2016: Average Number of Actual changes to supported network as at February 2016, daily bus electoral Number of compared to network before April 2015 passengers Hastings Lewes Rother Wealden Eastbourne divisions -

Ditching Schedule – 2020 Last Updated 29/10/20
Ditching Schedule – 2020 Last updated 29/10/20 This schedule shows current scheduled dates for ditching. Please note that these dates can change due to weather. Road Road Name Parish Estimated Number Date A275 COOKSBRIDGE ROAD Hamsey Oct-20 A275 OFFHAM ROAD Hamsey Oct-20 A275 RESTING OAK HILL Hamsey Oct-20 C205 DEADMANTREE HILL Hamsey Oct-20 C6 BEECHWOOD LANE Hamsey Oct-20 C8 THE DROVE Hamsey Oct-20 C8 NORTH END LANE Hamsey Oct-20 U5012 WHITFELD LANE Hamsey Oct-20 U5012 HAMSEY LANE Hamsey Oct-20 U5013 IVORS LANE Hamsey Oct-20 C120 LULLINGTON ROAD Cuckmere Valley Oct-20 C39 ALFRISTON ROAD Alfriston Oct-20 U7726 WINTON STREET Alfriston Oct-20 C210 THE STREET Long Man Oct-20 C210 THORNWELL ROAD Long Man Oct-20 C724 MILTON STREET Long Man Oct-20 U7084 HAYREED LANE Long Man Oct-20 U7085 ROBIN POST LANE Long Man Oct-20 C39 STATION ROAD Berwick Oct-20 U70400 COMMON LANE Berwick Oct-20 U7724 THE VILLAGE Berwick Oct-20 C340 COMMON LANE Alciston Oct-20 U7086 BOPEEP LANE Alciston Oct-20 C207 LANGTYE LANE Selmeston Nov-20 C207 POUNDFIELD ROAD Selmeston Nov-20 U7044 DARP LANE Selmeston Nov-20 C210 CANEHEATH Arlington Nov-20 C210 ARLINGTON ROAD WEST Arlington Nov-20 C340 CHILVER BRIDGE ROAD Arlington Nov-20 C340 THE STREET Arlington Nov-20 C340 WILBEES ROAD Arlington Nov-20 C347 LOWER WICK STREET Arlington Nov-20 C39 STATION ROAD Arlington Nov-20 C39 WICK STREET Arlington Nov-20 C39 COLDHARBOUR ROAD Arlington Nov-20 C690 MICHELHAM PRIORY ROAD Arlington Nov-20 U7082 SESSINGHAM LANE Arlington Nov-20 U7083 TYE HILL LANE Arlington Nov-20 U7124 THE STREET