Guidance for Basic and Advanced Life Support in COVID-19 Adult Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Basic Life Support + First Aid for Healthcare Providers 2020 Course Introduction
Basic Life Support + First Aid for Healthcare Providers 2020 Course Introduction SECTION 1: Foundational concepts of BCLS SECTION 2: Response to an adult in cardiac arrest SECTION 3: Basic Life Support for infants and children SECTION 4: Automated external defibrillation in infants and children SECTION 5: Preventing cardiac arrest SECTION 6: First aid for adults SECTION 7: First aid for children Activity Summary • Activity Title: Basic Life Support (BLS) & First Aid (Cardiopulmonary Resuscitation (CPR), Automated External Defibrillator (AED), and First Aid) • Release date: 2021-06-01 • Expiration date: 2024-06-01 • Estimated time to complete activity: 8 hours • This course is accessible with any web browser. We recommend recent versions of • Google Chrome, Internet Explorer 9 and later, or Apple iPad. • This course is jointly provided by Pacific Medical Training and Postgraduate Institute for Medicine (PIM). You may reach PIM at [email protected]. Target Audience This activity has been designed to meet the educational needs of physicians, physician assistants, nurse practitioners, registered nurses, pharmacists and dentists involved in the care of patients who require advanced life support. 3103 Philmont Ave, Suite 308 • Huntingdon Valley, PA 19006 • 800-417-1748 page 1 Educational Objectives After completing this activity, the participant should be better able to: • Explain the change in emphasis from airway and ventilation to compressions and perfusion. • Select the correct order of interventions for the victim of cardiopulmonary arrest. • List the steps required to safely operate an AED. • Differentiate between adult and pediatric guidelines for CPR. • Explain how to apply the various first aid interventions. • Describe how to apply the various pediatric first aid interventions. -

Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality 1
Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality 1 Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality Web-based Integrated 2010 & 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Key Words: cardiac arrest cardiopulmonary resuscitation defibrillation emergency 1 Highlights & Introduction 1.1 Highlights: Lay Rescuer CPR Summary of Key Issues and Major Changes Key issues and major changes in the 2015 Guidelines Update recommendations for adult CPR by lay rescuers include the following: The crucial links in the out-of-hospital adult Chain of Survival are unchanged from 2010, with continued emphasis on the simplified universal Adult Basic Life Support (BLS) Algorithm. The Adult BLS Algorithm has been modified to reflect the fact that rescuers can activate an emergency response (ie, through use of a mobile telephone) without leaving the victim’s side. It is recommended that communities with people at risk for cardiac arrest implement PAD programs. Recommendations have been strengthened to encourage immediate recognition of unresponsiveness, activation of the emergency response system, and initiation of CPR if the lay rescuer finds an unresponsive victim is not breathing or not breathing normally (eg, gasping). Emphasis has been increased about the rapid identification of potential cardiac arrest by dispatchers, with immediate provision of CPR instructions to the caller (ie, dispatch-guided CPR). The recommended sequence for a single rescuer has been confirmed: the single rescuer is to initiate chest compressions before giving rescue breaths (C-A-B rather than A-B-C) to reduce delay to first compression. The single rescuer should begin CPR with 30 chest compressions followed by 2 breaths. -
(Als) Ambulance Inventory List
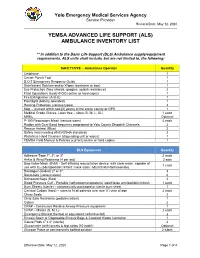
Yolo Emergency Medical Services Agency Service Provider Revised Date: May 12, 2020 YEMSA ADVANCED LIFE SUPPORT (ALS) AMBULANCE INVENTORY LIST ** In addition to the Basic Life Support (BLS) Ambulance supply/equipment requirements, ALS units shall include, but are not limited to, the following: SAFETY/PPE – Ambulance Operator Quantity Cellphone 1 Center Punch Tool 1 D.O.T Emergency Response Guide 1 Disinfectant Solution and/or Wipes (container or box) 1 Eye Protection (face shields, goggles, splash resistance) 2 Field Operations Guide (FOG) online or hard copies 1 Fire Extinguisher (A-B-C) 1 Flashlight (battery operated) 1 Hearing Protection (various types) 2 Map – (current within two [2] years) of the entire county or GPS 1 Medical Grade Gloves, Latex free – sizes (S, M, L, XL) 1 each MREs Optional P-100 Respiratory Mask (various sizes) 4 each Radios with Dual Band frequency programed to Yolo County Dispatch Channels 2 Rescue Helmet (Blue) 2 Safety Vest meeting ANSI/OSHA standards 2 Waterless Hand Cleanser (dispensing unit or wipes) 1 YEMSA Field Manual & Policies (current) online or hard copies 1 BLS Equipment Quantity Adhesive Tape 1", 2", or 3" 2 each Ankle & Wrist Restraints (4 per set) 2 sets Bag-Valve-Mask (BVM) - Self-inflating resuscitation device, with clear mask, capable of 1 each use with O2 (adult/pediatric/infant; mask sizes: adult/child/infant/neonate) Bandages (Rolled) 2" or 3" 3 Band-Aids (various sizes) 6 Biohazard Bags (Red) 2 Blood Pressure Cuff - Portable (sphygmomanometers) (adult/large arm/pediatric/infant) 1 each -

Emergency Medical Services Statutes and Regulations
Emergency Medical Services Statutes and Regulations Printed: August 2016 Effective: September 11, 2016 1 9/16/2016 Statutes and Regulations Table of Contents Title 63 of the Oklahoma Statutes Pages 3 - 13 Sections 1-2501 to 1-2515 Constitution of Oklahoma Pages 14 - 16 Article 10, Section 9 C Title 19 of the Oklahoma Statutes Pages 17 - 24 Sections 371 and 372 Sections 1- 1201 to 1-1221 Section 1-1710.1 Oklahoma Administrative Code Pages 25 - 125 Chapter 641- Emergency Medical Services Subchapter 1- General EMS programs Subchapter 3- Ground ambulance service Subchapter 5- Personnel licenses and certification Subchapter 7- Training programs Subchapter 9- Trauma referral centers Subchapter 11- Specialty care ambulance service Subchapter 13- Air ambulance service Subchapter 15- Emergency medical response agency Subchapter 17- Stretcher aid van services Appendix 1 Summary of rule changes Approved changes to the June 11, 2009 effective date to the September 11, 2016 effective date 2 9/16/2016 §63-1-2501. Short title. Sections 1-2502 through 1-2521 of this title shall be known and may be cited as the "Oklahoma Emergency Response Systems Development Act". Added by Laws 1990, c. 320, § 5, emerg. eff. May 30, 1990. Amended by Laws 1999, c. 156, § 1, eff. Nov. 1, 1999. NOTE: Editorially renumbered from § 1-2401 of this title to avoid a duplication in numbering. §63-1-2502. Legislative findings and declaration. The Legislature hereby finds and declares that: 1. There is a critical shortage of providers of emergency care for: a. the delivery of fast, efficient emergency medical care for the sick and injured at the scene of a medical emergency and during transport to a health care facility, and b. -

State Ambulance Policies and Services (OEI-09-95-00410; 2/98)
- - -- -------- --of -- - OFFICE OF INSPECTOR GENERAL FEBRUARY 1998 OEI-09-95-00410 EXECUTIVE SUMMARY PURPOSE To provide baseline data about the ambulance industry and determine how State and local ordinances affect the delivery of ambulance services. BACKGROUND According to Section 1861(s)(7) of Social Security Act, Medicare pays for medically necessary ambulance services when other forms of transportation would endanger the beneficiary’s health. Ambulance suppliers provide two distinct levels of service--advanced life support and basic life support. The major distinctions between the levels are the types of vehicles and the skills of the personnel and the services they render. The Health Care Financing Administration (HCFA) is considering proposed Medicare regulations that would base reimbursement for ambulance services on the patient’s condition rather than the type of vehicle and personnel used. The final rule may include a special waiver for suppliers in non-Metropolitan Statistical Areas who would be hurt financially if they use only advanced life support ambulances. The HCFA may consider several options and may include a special waiver only if HCFA is convinced through overwhelming information of the need for the waiver. We decided to examine the effect and need for a special waiver based on Metropolitan Statistical Areas and non-Metropolitan Statistical Areas. In addition, we developed baseline information on the number of ambulance suppliers, vehicles, and personnel nationwide. We conducted in-person and telephone interviews with 53 State Emergency Medical Services Directors for the 50 States, the District of Columbia, the Commonwealth of Puerto Rico, and the U.S. Virgin Islands. Using a structured discussion guide, we (1) identified State, county, and municipal mandates that require specific levels of ambulance services and (2) obtained baseline data on the number of suppliers, licensed vehicles, and certified personnel operating within the States in 1995 and 1996. -

Collective Advanced Life Support Ambulance an Innovative Transportation of Critical Care Patients by Bus in COVID-19 Pandemic Response
Collective Advanced Life Support Ambulance An Innovative Transportation of Critical Care Patients by Bus in COVID-19 Pandemic Response Thierry Lentz SAMU 92 Charles Groizard SAMU 92 Abel Colomes SAMU 92 Anna Ozguler ( [email protected] ) INSERM https://orcid.org/0000-0002-9277-610X Michel Baer SAMU 92 Thomas Loeb SAMU 92 Research article Keywords: Emergency medical service, Critical care transport, Interhospital transfer of critically ill patients, Collective Transport, Mass casualty incidents, Disaster DOI: https://doi.org/10.21203/rs.3.rs-48425/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/14 Abstract Background: During the COVID-19 pandemic, as the number of available Intensive Care beds in France did not meet the needs, it appeared necessary to transfer a large number of patients from the most affected areas to the less ones. Mass transportation resources were deemed necessary. To achieve that goal, the concept of a Collective Advanced Life Support Ambulance (CALSA) was proposed in the form of a long-distance bus re-designed and equipped so as to accommodate up to six intensive care patients and allow Advanced Life Support (ALS) techniques to be performed while en route. Methods: The expected beneƒt of the CALSA, when compared to ALS ambulances accommodating a single patient, was to reduce the resources requirements, in particular by a lower personnel headcount for several patients being transferred to the same destination. A foreseen prospect, comparing to other collective transportation vectors such as airplanes, was the door-to-door capability, minimalizing patients’ handovers for safety concerns and time e∆ciency. -

Goals of Care and End of Life in the ICU
Goals of Care and End of Life in the ICU Ana Berlin, MD, MPH, FACS KEYWORDS Goals of care Shared decision making ICU Functional and cognitive outcomes End-of-life care Palliative care Communication KEY POINTS The trauma and long-term sequelae of critical illness affect not only patients but also their families and caregivers. Unrealistic expectations and erroneous assumptions about the outcomes acceptable to patients are important drivers of misguided and goal-discordant medical treatment. Compassionately delivering accurate and honest prognostic information inclusive of func- tional, cognitive, and psychosocial outcomes is crucial for helping patients and families understand what to expect from an episode of surgical crticial illness. Skilled communication and shared decision-making strategies ensure that treatments provided in the ICU are aligned with realistic and attainable patient goals. Attentive management of physical and nonphysical symptoms, including the psychosocial and spiritual needs of families and caregivers, eases suffering in the ICU and beyond. INTRODUCTION There is little doubt that the past half-century has seen tremendous advances in surgical critical care. The advent of lung-protective ventilation in the management of acute respiratory distress syndrome (ARDS), the evolution of balanced resusci- tation strategies for the reduction of abdominal compartment syndrome, and the aggressive deployment of prevention and treatment strategies against the systemic inflammatory response syndrome and sepsis, along with many other technological innovations, have markedly reduced the morbidity and mortality associated with critical illness and multiorgan system failure. Nevertheless, at times even the Disclosure Statement: Support for Dr A. Berlin’s preparation of this article was provided by the New Jersey Medical School Hispanic Center of Excellence, Health Resources and Services Administration through Grant D34HP26020. -

Required ALS and BLS Equipment and Supplies
S T A T E O F H A W A I I D E P A R T M E N T O F H E A L T H ESSENTIAL EQUIPMENT and SUPPLIES FOR BASIC and ADVANCED LIFE SUPPORT Ambulance Service Standards Revised 10-14-10 ESSENTIAL EQUIPMENT FOR BASIC LIFE SUPPORT Ambulance cot w/ 3 seatbelts Sheets, linen or disp., 4 ea Cot fasteners, Floor/Wall Mount Blankets, non-synthetic, 4 ea Portable oxygen unit 360L min. tank Gauze pads, sterile, 3x3 min, 24 ea Flowmeter 0-15L/min Gauze rolls, sterile, 2" x 5 yds, 4 ea Positive pressure elder-type valve Gauze rolls, sterile 3"/4" x 5 yds, 4 ea Oxygen masks, clear, disposable, adult/pedi 1 ea Gauze rolls, sterile, 6" x 5 yds, 4 ea Oxygen nasal cannula, disposable 2 ea Triangle bandage, 40" min, 3 ea Oropharyngeal airways, adult/ped/infant 1 ea Universal dressing, 8 x 10 min, sterile, 1 ea Nasopharyngeal airways, 2 ea Tape, 1" and 2" x 5 yds, 1 ea Oxygen tanks, spare, 360L min, 2 ea Bandaids, assorted Bag-valve-mask, pedi w/02 reservoir Plastic wrap, 12" x' 12" min, 1 ea Bag-valve-mask, adult w/02 reservoir Burn sheets, sterile, 2 ea Suction, portable, battery operated Sphygmomanometer, adult, 1 ea Widebore tubing Extra large adult, 1 ea Rigid pharyngeal suction tip Pediatric, 1 ea Suction catheters 5, 10, 14, 18fr, 1 ea Stethescope, 1 ea Bite sticks (mouth gag), 2 ea Scissors, bandage, 5" min Ammonia inhalants, 3 ea Thermometer, oral and rectal, 1 ea Antiseptic swabs, 50 ea Spineboard, short, w/straps, 1 ea Bulb syringe, 3 oz. -

2016-05 REMAC Advisory ALS Medical Director
THE REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL OF NEW YORK CITY, INC. NYC REMAC Advisory No. 2016-05 Title: Requirements for the Provision of Advanced Life Support Level Care, Section III: Paramedic (EMTP) Service Medical Director (Updated) Issue Date: July 1, 2016 Effective Date: July 1, 2016, Sunsets July 1, 2017 Supersedes: n/a Page: 1 of 4 The Regional Emergency Medical Advisory Committee (REMAC) of New York City is responsible to develop, approve and implement prehospital treatment and transport protocols for use within the five boroughs of the City of New York. The Regional Emergency Medical Advisory Committee (REMAC) of New York City operates under the auspices of Article 30 of the New York State Public Health Law. Requirements for Advanced Life Support Medical Director have been revised and are attached. These requirements apply to all medical directors of Advanced Life Support EMS Agencies operating in the NYC region. Medical Director Requirements are effective July 1, 2016. These requirements will be assessed when ALS Agency recertifies. Agency will be responsible to provide all information needed. Any agency renewing after July 1, 2016 must meet new standards, with a sunset date of July 1, 2017. If requirements not met, ALS agency will receive a 30-day warning letter, then suspension. Current and Updated Protocols can be accessed at the Regional EMS Council website: www.nycremsco.org. Owners/operators of Ambulance and ALS First Response Services providing prehospital medical treatment within the five boroughs of the City of New York are responsible to provide copies of the NYC REMAC Prehospital Treatment Protocols to their personnel, and to ensure that Service Medical Directors and EMS personnel are informed of all changes/updates to the NYC REMAC Prehospital Treatment Protocols. -

Event Medical Flyer.Pub
EMS DETAIL PRICE LIST MedStar Vision Ambulance Crew We aspire to be a world class Mobile Healthcare Provider for ALS: $110.00 per hour with a 4 hour minimum both our customers and employees and to set standards for others to follow BLS: $100.00 per hour with a 4 hour minimum Bicycle Team $100.00 per hour with a 4 hour minimum MedStar Mission Mule Team To provide World Class Mobile Healthcare with the highest quality Customer Service and Clinical Excellence in a Fiscally ALS: $110.00 per hour with a 4 hour minimum Responsible Manner. BLS: $100.00 per hour with a 4 hour minimum First‐Aid One ALS Provider: $60.00 per hour with a 4 hour minimum One BLS Provider: $45.00 per hour with a 4 hour minimum ALS Team: $110.00 per hour with a 4 hour minimum BLS Team: $100.00 per hour with a 4 hour minimum Rodeo Team for 2 person team ALS: $110.00 per hour with a 4 hour minimum MedStar Mobile Healthcare BLS: $100.00 per hour with a 4 hour minimum 2900 Alta Mere Drive EMS Supervisor Fort Worth, TX 76116 $80.00 per hour with a 4 hour minimum Tina Marn, EMT ALS: Advanced Life Support is a set of life‐saving protocols and Special Operaons Supervisor skills that extend BLS to further support the circulaon and pro‐ Office: 817‐840‐2058 vide an open airway and adequate venlaon (breathing). MedStar Mobile Healthcare is the exclusive Cell: 817‐372‐2123 emergency and non‐emergency mobile BLS: Basic Life Support is basic First Aid and Airway management Email: [email protected] healthcare provider to Fort Worth and 14 other without the use of medicaons and advance skills and treat‐ hp://www.medstar911.org/community‐events surrounding cies including Haltom City, Bur‐ ments. -

Recommendations for End-Of-Life Care in the Intensive Care Unit: a Consensus Statement by the American College of Critical Care Medicine
Special Articles Recommendations for end-of-life care in the intensive care unit: A consensus statement by the American College of Critical Care Medicine Robert D. Truog, MD, MA; Margaret L. Campbell, PhD, RN, FAAN; J. Randall Curtis, MD, MPH; Curtis E. Haas, PharmD, FCCP; John M. Luce, MD; Gordon D. Rubenfeld, MD, MSc; Cynda Hylton Rushton, PhD, RN, FAAN; David C. Kaufman, MD Background: These recommendations have been developed to to die, and between consequences that are intended vs. those that improve the care of intensive care unit (ICU) patients during the are merely foreseen (the doctrine of double effect). Improved dying process. The recommendations build on those published in communication with the family has been shown to improve pa- 2003 and highlight recent developments in the field from a U.S. tient care and family outcomes. Other knowledge unique to end- perspective. They do not use an evidence grading system because of-life care includes principles for notifying families of a patient’s most of the recommendations are based on ethical and legal death and compassionate approaches to discussing options for principles that are not derived from empirically based evidence. organ donation. End-of-life care continues even after the death of Principal Findings: Family-centered care, which emphasizes the patient, and ICUs should consider developing comprehensive the importance of the social structure within which patients are bereavement programs to support both families and the needs of embedded, has emerged as a comprehensive ideal for managing the clinical staff. Finally, a comprehensive agenda for improving end-of-life care in the ICU. -

Tracheal Intubation Intubação Traqueal
0021-7557/07/83-02-Suppl/S83 Jornal de Pediatria Copyright © 2007 by Sociedade Brasileira de Pediatria ARTIGO DE REVISÃO Tracheal intubation Intubação traqueal Toshio Matsumoto1, Werther Brunow de Carvalho2 Resumo Abstract Objetivo: Revisar os conceitos atuais relacionados ao procedimento Objective: To review current concepts related to the procedure of de intubação traqueal na criança. tracheal intubation in children. Fontes dos dados: Seleção dos principais artigos nas bases de Sources: Relevant articles published from 1968 to 2006 were dados MEDLINE, LILACS e SciELO, utilizando as palavras-chave selected from the MEDLINE, LILACS and SciELO databases, using the intubation, tracheal intubation, child, rapid sequence intubation, keywords intubation, tracheal intubation, child, rapid sequence pediatric airway, durante o período de 1968 a 2006. intubation and pediatric airway. Síntese dos dados: O manuseio da via aérea na criança está Summary of the findings: Airway management in children is relacionado à sua fisiologia e anatomia, além de fatores específicos related to their physiology and anatomy, in addition to specific factors (condições patológicas inerentes, como malformações e condições (inherent pathological conditions, such as malformations or acquired adquiridas) que influenciam decisivamente no seu sucesso. As principais conditions) which have a decisive influence on success. Principal indicações são manter permeável a aérea e controlar a ventilação. A indications are in order to maintain the airway patent and to control laringoscopia e intubação traqueal determinam alterações ventilation. Laryngoscopy and tracheal intubation cause cardiovascular cardiovasculares e reatividade de vias aéreas. O uso de tubos com alterations and affect airway reactivity. The use of tubes with cuffs is not balonete não é proibitivo, desde que respeitado o tamanho adequado prohibited, as long as the correct size for the child is chosen.