Cambridgeshire and Peterborough Clinical Commissioning Group
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ely Circular Ely Circular (Extended)
Ely Circular Ely Circular (extended) 1st walk check 2nd walk check 3rd walk check 1st walk check 2nd walk check 3rd walk check 25th Sept. 2016 12th Sept. 2016 Current status Document last updated Monday, 24th July 2017 This document and information herein are copyrighted to Saturday Walkers’ Club. If you are interested in printing or displaying any of this material, Saturday Walkers’ Club grants permission to use, copy, and distribute this document delivered from this World Wide Web server with the following conditions: The document will not be edited or abridged, and the material will be produced exactly as it appears. Modification of the material or use of it for any other purpose is a violation of our copyright and other proprietary rights. Reproduction of this document is for free distribution and will not be sold. This permission is granted for a one-time distribution. All copies, links, or pages of the documents must carry the following copyright notice and this permission notice: Saturday Walkers’ Club, Copyright © 2016-2017, used with permission. All rights reserved. www.walkingclub.org.uk This walk has been checked as noted above, however the publisher cannot accept responsibility for any problems encountered by readers. Ely Circular Start: Ely station Finish: Ely station Ely station, map reference TL 543 793, is 23 km north east of Cambridge, 102 km north north east of Charing Cross, 5m above sea level, and in East Cambridgeshire. Length: 18.0 km (11.2 mi), of which 4.3 km (2.7 mi) on tarmac or concrete. Cumulative ascent/descent: 108m. -
Oosthuizen, MSR, DB Fenland, 30 Jan 2015
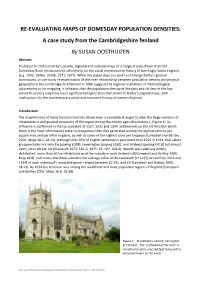
RE-EVALUATING MAPS OF DOMESDAY POPULATION DENSITIES: A case study from the Cambridgeshire fenland By SUSAN OOSTHUIZEN Abstract Professor Sir Clifford Darby’s county, regional and national maps of a range of data drawn from the Domesday Book revolutionized scholarship on the social and economic history of late Anglo-Saxon England (e.g. 1935, 1936a, 1936b, 1971, 1977). While this paper does not seek to challenge Darby’s general conclusions, a case study re-examination of the inter-relationship between population density and physical geography in the Cambridgeshire fenland in 1086 suggests the regional usefulness of methodological adjustments to his mapping. It indicates that the population density of the peat and silt fens in the late eleventh century may have been significantly higher than that shown in Darby’s original maps, with implications for the contemporary social and economic history of eastern England. Introduction The magnificence of many fenland churches allows even a complete stranger to infer the large numbers of inhabitants in and general prosperity of the region during the middle ages (Illustration 1, Figure 1). Its affluence is confirmed in the lay subsidies of 1327, 1332 and 1334. Settlements on the silt fens (for which there is the most information) were so prosperous that they generated among the highest returns per square mile and per vill in England, as well as some of the highest rates per taxpayer (Campbell and Bartley 2006: Maps 18.3, 18.13). Although only 20% of English settlements paid more than £225 in 1334, that select group includes not only Ely (paying £358), Leverington (paying £360), and Wisbech (paying £410) but almost every other silt fen vill (Glasscock 1973: 181-3; 1975: 28, 107, 168-9). -

The David Attenborough Building Pembroke St, Cambridge CB2 3QY
Venue The David Attenborough Building Pembroke St, Cambridge CB2 3QY http://www.conservation.cam.ac.uk/ Cambridge Cambridge is a university city and the county town of Cambridgeshire, England, on the River Cam about 50 miles (80 km) north of London. At the United Kingdom Census 2011, its population was 123,867, including 24,488 students. There is archaeological evidence of settlement in the area in the Bronze Age and in Roman Britain; under Viking rule, Cambridge became an important trading centre. The first town charters were granted in the 12th century, although city status was not conferred until 1951. Cambridge is the home of the University of Cambridge, founded in 1209 and one of the top five universities in the world. The university includes the Cavendish Laboratory, King's College Chapel, and the Cambridge University Library. The Cambridge skyline is dominated by the last two buildings, along with the spire of the Our Lady and the English Martyrs Church, the chimney of Addenbrooke's Hospital and St John's College Chapel tower. Cambridge is at the heart of the high-technology Silicon Fen with industries such as software and bioscience and many start-up companies spun out of the university. Over 40% of the workforce have a higher education qualification, more than twice the national average. Cambridge is also home to the Cambridge Biomedical Campus, one of the largest biomedical research clusters in the world, soon to be home to AstraZeneca, a hotel and relocated Papworth Hospital. Parker's Piece hosted the first ever game of Association football. The Strawberry Fair music and arts festival and Midsummer Fairs are held on Midsummer Common, and the annual Cambridge Beer Festival takes place on Jesus Green. -

The Jews of Medieval Cambridge
The Jews ofmedieval Cambridge R. B. DOBSON As it happens, this presidential address is being delivered more or less seven hundred years to the day since the last persecuted survivors of the once substantial medieval English Jewrywere crossing the Channel into involuntary exile, 'without the hope of ever returning', after their banishment from this country on i Novem? ber 1290.1 Itmay not be quite so important,but it is certainlymuch less dispiriting, to remember that almost a century has elapsed since the foundation of this Society in 1893.2 As we rapidly approach our centenary year, we must all hesitate to think what the present state of Jewish historical studies in this countrywould now be had it not been for the indefatigable labours and enterprise of our founding fathers a hundred years ago. Perhaps a medieval historian might be forgiven formaking the additional point that at the heart of our Society's almost instantaneous scholarly success in the 1890s lay a particular strength inmedieval Jewish studies. At a period when the academic study of history, heavily biased towards English national political and constitutional development, was an extremely young and tender plant within British universities, this Society's earliest members were conducting detailed documentary research of exceptional quality, research whose full value is still perhaps insufficiently appreciated a hundred years later. The enthusiasm for Jewish history unleashed by the great London Anglo-Jewish Historical Exhibition of 1887 created what Professor Robert Stacey has recently termed the 'heroic age' of Jewish historical scholarship in England.3 Above all, this was the heroic age for the study ofmedieval Anglo-Jewry, adorned as that studywas by scholars, often not themselves university-trained, of the calibre of Joseph Jacobs, Lionel Abrahams, Michael Adler, Herbert Loewe and Lucien Wolf, whose 'A Plea for Anglo-Jewish History' filled the first pages of the first volume of the Society's Transactions in 1893-4. -
King Open/Cambridge Street Upper School & Community Complex
THE CAMBRIDGE LIFE FALL 2019 ISSUE 3, VOL.4 A PUBLICATION OF THE CITY OF CAMBRIDGE, MASSACHUSETTS THECAMBRIDGELIFE.ORG Cambridge Street King Open/ Homecoming Cambridge Street Upper School & Community Meeting the Needs of Our Younger Complex Residents Valente Branch Library Recreation Amenities & Open Space Were Project Priorities Transportation & Mobility Features A Historical Pictorial of 850 Cambridge Street King Open/Cambridge Street Upper School & Community Complex Site Map Project Overview The 273,000 square foot facility at 850 Cambridge St. opened in September 2019 and houses the King Open School (JK-5), Cambridge Street Upper School (6-8), Cambridge Public Schools Administration, King Open Preschool, King Open Extended Day (KOED), Community Schools, and Valente Library The $159 million school and community complex is a net zero-ready project that consumes no fossil fuels onsite, has a highly efficient design to minimize energy demand, and incorporates the City’s largest solar array to renewably produce much of the energy needed. Remaining energy will come from the electrical grid, and when Cambridge secures 100% renewable electricity supply, the complex will achieve net zero emissions. Site amenities and open spaces include Gold Star Pool, two gyms, two basketball courts, Charles G. Rossi Bocce Court, five playgrounds, outdoor splash pad, Cambridge Street Plaza, Valente Reading Garden, a Learning Courtyard/Outdoor Classroom, and a 380-seat auditorium. “One of the important considerations throughout this entire process was to make sure we successfully met the needs of the students, staff, the school administration, the neighborhood, and users of Cambridge Street,” said Lisa Peterson, Deputy City Manager and King Open/Cambridge Street Upper School & Community Complex Project Manager, adding that an extensive community process was conducted. -

DAY 1: Cambridge
Expat Explore - Version: Sat Sep 25 2021 10:34:53 GMT+0000 (Coordinated Universal Time) Page: 1/9 Itinerary for Great Britain Christmas Tour • Expat Explore Start Point: End Point: Outside Hotel Novotel at Greenwich Outside Hotel Novotel at Greenwich station, station, 173-185 Greenwich High Road, London, SE10 173-185 Greenwich High Road, London, SE10 8JA 8JA 06:30 hrs 17:30 hrs – 20:30 hrs Hotel lobby at Holiday Inn Express, Greenwich, 85 Bugsby Way, Greenwich, London, SE10 0GD 07:00 hrs DAY 1: Start of tour in London - Cambridge - York Welcome to your Christmas tour of Great Britain! Today you will fill your lungs with fresh, English countryside air, as you depart the city of London, and head to where the grass is greener. Arriving in Cambridge, your first adventure will have you punting along the river in traditional style, taking in the stunning scenery and epic, historical buildings in the most relaxing way. Simply wonderful! The Expat Explore - Version: Sat Sep 25 2021 10:34:53 GMT+0000 (Coordinated Universal Time) Page: 2/9 afternoon sees you continuing your rural ‘rovering’, towards York, a mecca for history buffs and lovers of fine architecture and culture. Your walking tour offers fascinating insights, stories and history of the city. Tonight you will enjoy dinner in a traditional Sunday Roast dinner at a British pub - don’t forget to try the Yorkshire puddings! Experiences Cambridge punting: Float down the River Cam as you go punting - an age-old tradition in Cambridge Walking tour of York: Gain insights into this historic walled city on a walking tour with your Expat Explore tour leader. -

The Cambridge Handbook of the Learning Sciences Edited by R
Cambridge University Press 0521845548 - The Cambridge Handbook of the Learning Sciences Edited by R. Keith Sawyer Frontmatter More information The Cambridge Handbook of the Learning Sciences Learning sciences is an interdisciplinary field that studies teaching and learning. The sciences of learning include cognitive science, educational psychology, computer sci- ence, anthropology, sociology, neuroscience, and other fields. The Cambridge Handbook of the Learning Sciences shows how educators can use the learning sciences to design more effective learning environments, including school classrooms and informal settings such as science centers or after-school clubs, online distance learning, and computer- based tutoring software. The chapters in this handbook describe exciting new classroom environments, based on the latest science about how children learn. CHLS is a true handbook: readers can use it to design the schools of the future – schools that will prepare graduates to participate in a global society that is increasingly based on knowledge and innovation. R. Keith Sawyer is Associate Professor of Education at Washington University in St. Louis. He received his Ph.D. in Psychology at the University of Chicago and his S.B. in Computer Science at the Massachusetts Institute of Technology. He studies cre- ativity, collaboration, and learning. Dr. Sawyer has written or edited eight books. His most recent book is Explaining Creativity: The Science of Human Innovation (2006). © Cambridge University Press www.cambridge.org Cambridge University Press 0521845548 - The Cambridge Handbook of the Learning Sciences Edited by R. Keith Sawyer Frontmatter More information The Cambridge Handbook of the Learning Sciences Edited by R. Keith Sawyer Washington University © Cambridge University Press www.cambridge.org Cambridge University Press 0521845548 - The Cambridge Handbook of the Learning Sciences Edited by R. -

Witches and Witchcraft in Ely
Witches and Witchcraft in Ely A HISTORY Francis Young Printed for the author by Cambridge Print Solutions Cambridge, 2013 Published by Francis Young © Francis Young 2013 Francis Young has asserted his moral right under the Copyright, Designs and Patents Act, 1988, to be identified as the author of this work. francisyoung.wordpress.com ISBN 978-0-9926404-0-8 Table of Contents Introduction 1 1. Hereward and the Witch 3 2. A Necromancer in the Lady Chapel 5 3. Witchcraft and the Reformation 9 4. Witchfinders in Ely 11 5. Witchcraft in Ely in Modern Times 15 Notes 20 Introduction The Cambridgeshire Fens are one of the last places in England where traditional belief in witchcraft was widespread. Until as late as the mid-twentieth century, Fenland communities were isolated, and their inhabitants were more vulnerable to environmental illnesses, such as malaria, than the rest of the population. A hard life, geographical isolation, close-knit communities and mistrust of outsiders may all have contributed to the Fenlanders’ abiding belief in the power of witchcraft. Ely’s place in the history of English witchcraft is a special one. As the cathedral city at the heart of the Fens, under the independent jurisdiction of the Bishop, Ely was the place where anyone locally accused of witchcraft would be brought to trial. The city was the hub from which John Stearne completed the last stage of Matthew Hopkins’s infamous witch-hunt in the 1640s, and Ely was the scene for the (quite literal) downfall of the first ‘witch’ to appear in English history. -

Cambridge and Peterborough ICS Development Plan 31St March 2021
Cambridge and Peterborough ICS Development Plan 31st March 2021 NHS England and NHS Improvement Contents Section Page Executive summary 3 System overview 4-9 Cambridge and Peterborough ICS development plan 10-22 Gap analysis 23-30 Next steps 31-32 2 | Executive summary Cambridge and Peterborough have recently been successful in our application for ICS designation. Whilst this is a significant step in our journey as a system, we also acknowledge that there is much work to be done to make the C&P ICS a success. Our ambition is to launch our ICS in shadow form during Q4 of 2021/22 before the new ICS establishment is formalised in Q1 2022/23. There are a significant number of development steps that we need to take in order to meet this ambition, which have been grouped thematically to include: • System roles and capabilities • System leadership and accountability • System oversight and quality improvement • Leadership and people development • Financial framework and use of resources • System and digital transformation Each of these themes requires a significant amount of engagement, design work, implementation work, and throughout we must ensure that we continue to deliver business as usual activities and meet our operational and strategic targets. As a result, we have developed the following plan to set out how we aim to deliver the spectrum of activities required to ensure we progress towards our future vision whilst meeting the current needs of our local population and stakeholders. Whilst developing the plan, we have ensured it will deliver against five key development areas highlighted to us by the regional team including: finance, regional clinical leadership, workforce, provider collaboration and Local Authority engagement. -

Registered Food Premises V3 - Addresses Removed
Registered Food Premises V3 - addresses removed Food Use Business Name, Address Bakeries selling through their own shops F P Lanes & Sons Bakery 20 High Street Burwell Cambridge CB25 Bakers Shops Boswell & Son 5 High Street Passage Ely Cambridgeshir Bakers with no on site retail activity Grain Culture 16 Sedgeway Business Park Witchford C Beekeepers Helen Arnold Beekeepers Ely Queen Bees Beekeepers Michael Grey Brewery Three Blind Mice Brewery Unit 10 Black Bank Business Centre Blac Brewery Vinifera Ltd The Stables Hall Farm 8 London Road Ne Brewery Downham Isle Brewery 1 Matthew Wren Close Little Downham Brewery The Sparkling Sake Brewery Unit 1 Black Bank Business Centre Black Brewery Elysian Fields Vineyard Bedwell Hey Farm Ely Road Little Thetfo Butchers Edis Of Ely Limited 24 High Street Ely Cambridgeshire CB7 4 Butchers Bent & Cornwell Quality Meats 24 Market Place Ely Cambridgeshire CB7 Butchers Carter Street Butchers 125 Carter Street Fordham Ely Cambridg Butchers Jack Hurrell 26 High Street Burwell Cambridge CB5 0 Butchers JM & MA Thompson & Sons 1 Fen Bank Isleham Ely Cambridgeshire Butchers Harnwell And Son Limited 14 High Street Haddenham Ely Cambrid Cafes Beanies Vegan Coffee Hub Richmond House 16 - 18 Broad Street El Cafes Elk Coffee Limited 105 The Causeway Burwell Cambridge C Cafes Marmalade & Jam 27 High Street Ely Cambridgeshire CB7 4 02 July 2021 Page 1 of 39 Food Use Business Name, Address Cafes Gloof 9 Churchgate Street Soham Ely Cambrid Cafes Liz'spresso The Home 3 Saxon Business Park Littlep Cafes Fordham Abbey Cafe -

Divcowest Welcomes Bristol Myers Squibb to Cambridge Crossing Global Biopharmaceutical Company to Join Philips, Sanofi, and Cerevel at CX in the First Half of 2023
DivcoWest Welcomes Bristol Myers Squibb to Cambridge Crossing Global Biopharmaceutical Company To Join Philips, Sanofi, and Cerevel at CX in the First Half of 2023 Cambridge, MA, (August 18, 2020) – DivcoWest announced today that it has signed a 360,000 square- foot lease with Bristol Myers Squibb (NYSE:BMY) at 250 Water Street in Cambridge Crossing (CX), the new and connected neighborhood at the intersection of Cambridge, Somerville, and Boston. The new building is currently under construction and is expected to be complete in late 2022. Bristol Myers Squibb plans to combine its Cambridge presence at the state-of-the-art laboratory and office building at 250 Water Street by the end of the first half of 2023. Dedicated to helping patients prevail over serious diseases, the biopharmaceutical company will join Philips North America, Sanofi, and Cerevel Therapeutics in the vibrant CX community. “At Cambridge Crossing (CX), our mission is to create a home for innovative companies that inspires collaboration and scientific breakthroughs. We are thrilled that global leader Bristol Myers Squibb has chosen CX as their future home,” said Mark Roopenian, Managing Director at DivcoWest. “CX is designed to be a network of forward-thinking changemakers like Bristol Myers Squibb, and we are proud to create a space for them at 250 Water Street so that they can pursue discoveries that positively transform patients’ lives.” With the addition of Bristol Myers Squibb, approximately 1.7 million square-feet of commercial space is now leased and preleased at CX. Remaining space available for lease at CX includes 110,000 SF of science and technology space at 250 Water Street and 600,000 SF in two future buildings. -

School Prospectus 2014 - 2015 Learning, Growing and Achieving Together
Isle of Ely Primary School School Prospectus 2014 - 2015 Learning, Growing and Achieving Together Bryony Surtees Executive Head teacher Table of Contents Welcome letter 2 Whole School Aims 3 Who’s Who at Isle of Ely Primary School 4 Governors of Isle of Ely Primary School 5 Organisation of Education 6 Entry to School 7 The School Curriculum 9 Extra Curricular Activities 15 Special Needs, Including Gifted and Talented 16 Pastoral Care and Discipline 18 Uniform 20 Home-school Links 21 Absence 23 School Meals 24 Child Protection 25 Charging, Remissions and Complaints 26 1 An Active Learning Trust Academy Isle of Ely Primary School High Barns, CB7 Tel: 01223 728392 [email protected] Executive Head teacher: Mrs Bryony Surtees _____________________________________________________________________ Dear Parents The governors and staff at Isle of Ely Primary School extend a very warm welcome to you and your child. Isle of Ely Primary School is a fun, caring and stimulating learning environment. Our children are enthusiastic and lively, they enjoy the learning atmosphere of the school, but they are aware that we have high expectations and aspirations for them. We wish to work in partnership with you, to make you feel welcome and part of our team. Our Prospectus will tell you a little about our school, how we learn and develop, and what we are all working to achieve. To arrange a visit please contact Chloe Amory, our School General Assistant, in the school office. Yours faithfully Mrs Bryony Surtees Headteacher 2 Isle of Ely Primary School