Hepatitis C Virus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DEEP SEA LEBANON RESULTS of the 2016 EXPEDITION EXPLORING SUBMARINE CANYONS Towards Deep-Sea Conservation in Lebanon Project
DEEP SEA LEBANON RESULTS OF THE 2016 EXPEDITION EXPLORING SUBMARINE CANYONS Towards Deep-Sea Conservation in Lebanon Project March 2018 DEEP SEA LEBANON RESULTS OF THE 2016 EXPEDITION EXPLORING SUBMARINE CANYONS Towards Deep-Sea Conservation in Lebanon Project Citation: Aguilar, R., García, S., Perry, A.L., Alvarez, H., Blanco, J., Bitar, G. 2018. 2016 Deep-sea Lebanon Expedition: Exploring Submarine Canyons. Oceana, Madrid. 94 p. DOI: 10.31230/osf.io/34cb9 Based on an official request from Lebanon’s Ministry of Environment back in 2013, Oceana has planned and carried out an expedition to survey Lebanese deep-sea canyons and escarpments. Cover: Cerianthus membranaceus © OCEANA All photos are © OCEANA Index 06 Introduction 11 Methods 16 Results 44 Areas 12 Rov surveys 16 Habitat types 44 Tarablus/Batroun 14 Infaunal surveys 16 Coralligenous habitat 44 Jounieh 14 Oceanographic and rhodolith/maërl 45 St. George beds measurements 46 Beirut 19 Sandy bottoms 15 Data analyses 46 Sayniq 15 Collaborations 20 Sandy-muddy bottoms 20 Rocky bottoms 22 Canyon heads 22 Bathyal muds 24 Species 27 Fishes 29 Crustaceans 30 Echinoderms 31 Cnidarians 36 Sponges 38 Molluscs 40 Bryozoans 40 Brachiopods 42 Tunicates 42 Annelids 42 Foraminifera 42 Algae | Deep sea Lebanon OCEANA 47 Human 50 Discussion and 68 Annex 1 85 Annex 2 impacts conclusions 68 Table A1. List of 85 Methodology for 47 Marine litter 51 Main expedition species identified assesing relative 49 Fisheries findings 84 Table A2. List conservation interest of 49 Other observations 52 Key community of threatened types and their species identified survey areas ecological importanc 84 Figure A1. -

Metagenomic Identification of Diverse Animal Hepaciviruses and Pegiviruses
bioRxiv preprint doi: https://doi.org/10.1101/2020.05.16.100149; this version posted May 17, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Metagenomic identification of diverse animal hepaciviruses and 2 pegiviruses 3 4 5 Ashleigh F. Porter1, John H.-O. Pettersson1,2, Wei-Shan Chang1, Erin Harvey1, Karrie Rose3, 6 Mang Shi5, John-Sebastian Eden1,4, Jan Buchmann1, Craig Moritz6, Edward C. Holmes1 7 8 9 1. Marie Bashir Institute for Infectious Diseases and Biosecurity, School of Life and 10 Environmental Sciences and School of Medical Sciences, The University of Sydney, 11 Sydney, Australia. 12 2. Zoonosis Science Center, Department of Medical Biochemistry and Microbiology, 13 Uppsala University, Uppsala, Sweden. 14 3. Australian Registry of Wildlife Health, Taronga Conservation Society Australia, 15 Mosman, Australia. 16 4. Centre for Virus Research, Westmead Institute for Medical Research, Westmead, 17 Australia. 18 5. School of Medicine, Sun Yat-sen University, Guangzhou, China. 19 6. Research School of Biology, and Centre for Biodiversity Analysis, Australian National 20 University, Acton, ACT, Australia. 21 22 23 Address correspondence to: 24 Edward C. Holmes, 25 Marie Bashir Institute for Infectious Diseases and Biosecurity, School of Life and 26 Environmental Sciences and School of Medical Sciences, The University of Sydney, 27 Sydney, Australia 28 [email protected] 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.05.16.100149; this version posted May 17, 2020. -

Origins and Evolution of the Global RNA Virome
bioRxiv preprint doi: https://doi.org/10.1101/451740; this version posted October 24, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 1 Origins and Evolution of the Global RNA Virome 2 Yuri I. Wolfa, Darius Kazlauskasb,c, Jaime Iranzoa, Adriana Lucía-Sanza,d, Jens H. 3 Kuhne, Mart Krupovicc, Valerian V. Doljaf,#, Eugene V. Koonina 4 aNational Center for Biotechnology Information, National Library of Medicine, National Institutes of Health, Bethesda, Maryland, USA 5 b Vilniaus universitetas biotechnologijos institutas, Vilnius, Lithuania 6 c Département de Microbiologie, Institut Pasteur, Paris, France 7 dCentro Nacional de Biotecnología, Madrid, Spain 8 eIntegrated Research Facility at Fort Detrick, National Institute of Allergy and Infectious 9 Diseases, National Institutes of Health, Frederick, Maryland, USA 10 fDepartment of Botany and Plant Pathology, Oregon State University, Corvallis, Oregon, USA 11 12 #Address correspondence to Valerian V. Dolja, [email protected] 13 14 Running title: Global RNA Virome 15 16 KEYWORDS 17 virus evolution, RNA virome, RNA-dependent RNA polymerase, phylogenomics, horizontal 18 virus transfer, virus classification, virus taxonomy 1 bioRxiv preprint doi: https://doi.org/10.1101/451740; this version posted October 24, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. 19 ABSTRACT 20 Viruses with RNA genomes dominate the eukaryotic virome, reaching enormous diversity in 21 animals and plants. The recent advances of metaviromics prompted us to perform a detailed 22 phylogenomic reconstruction of the evolution of the dramatically expanded global RNA virome. -

REVIEW Hepatitis C Virus
DOI:http://dx.doi.org/10.7314/APJCP.2012.13.12.5917 Hepatitis C Virus -Proteins, Diagnosis, Treatment and New Approaches for Vaccine Development REVIEW Hepatitis C Virus - Proteins, Diagnosis, Treatment and New Approaches for Vaccine Development Hossein Keyvani1, Mehdi Fazlalipour2*, Seyed Hamid Reza Monavari1, Hamid Reza Mollaie2 Abstract Background: Hepatitis C virus (HCV) causes acute and chronic human hepatitis infection and as such is an important global health problem. The virus was discovered in the USA in 1989 and it is now known that three to four million people are infected every year, WHO estimating that 3 percent of the 7 billion people worldwide being chronically infected. Humans are the natural hosts of HCV and this virus can eventually lead to permanent liver damage and carcinoma. HCV is a member of the Flaviviridae family and Hepacivirus genus. The diameter of the virus is about 50-60 nm and the virion contains a single-stranded positive RNA approximately 10,000 nucleotides in length and consisting of one ORF which is encapsulated by an external lipid envelope and icosahedral capsid. HCV is a heterogeneous virus, classified into 6 genotypes and more than 50 subtypes. Because of the genome variability, nucleotide sequences of genotypes differ by approximately 31-34%, and by 20-23% among subtypes. Quasi-species of mixed virus populations provide a survival advantage for the virus to create multiple variant genomes and a high rate of generation of variants to allow rapid selection of mutants for new environmental conditions. Direct contact with infected blood and blood products, sexual relationships and availability of injectable drugs have had remarkable effects on HCV epidemiology. -

Participant List
Participant List 10/20/2019 8:45:44 AM Category First Name Last Name Position Organization Nationality CSO Jillian Abballe UN Advocacy Officer and Anglican Communion United States Head of Office Ramil Abbasov Chariman of the Managing Spektr Socio-Economic Azerbaijan Board Researches and Development Public Union Babak Abbaszadeh President and Chief Toronto Centre for Global Canada Executive Officer Leadership in Financial Supervision Amr Abdallah Director, Gulf Programs Educaiton for Employment - United States EFE HAGAR ABDELRAHM African affairs & SDGs Unit Maat for Peace, Development Egypt AN Manager and Human Rights Abukar Abdi CEO Juba Foundation Kenya Nabil Abdo MENA Senior Policy Oxfam International Lebanon Advisor Mala Abdulaziz Executive director Swift Relief Foundation Nigeria Maryati Abdullah Director/National Publish What You Pay Indonesia Coordinator Indonesia Yussuf Abdullahi Regional Team Lead Pact Kenya Abdulahi Abdulraheem Executive Director Initiative for Sound Education Nigeria Relationship & Health Muttaqa Abdulra'uf Research Fellow International Trade Union Nigeria Confederation (ITUC) Kehinde Abdulsalam Interfaith Minister Strength in Diversity Nigeria Development Centre, Nigeria Kassim Abdulsalam Zonal Coordinator/Field Strength in Diversity Nigeria Executive Development Centre, Nigeria and Farmers Advocacy and Support Initiative in Nig Shahlo Abdunabizoda Director Jahon Tajikistan Shontaye Abegaz Executive Director International Insitute for Human United States Security Subhashini Abeysinghe Research Director Verite -

Arenaviridae Astroviridae Filoviridae Flaviviridae Hantaviridae
Hantaviridae 0.7 Filoviridae 0.6 Picornaviridae 0.3 Wenling red spikefish hantavirus Rhinovirus C Ahab virus * Possum enterovirus * Aronnax virus * * Wenling minipizza batfish hantavirus Wenling filefish filovirus Norway rat hunnivirus * Wenling yellow goosefish hantavirus Starbuck virus * * Porcine teschovirus European mole nova virus Human Marburg marburgvirus Mosavirus Asturias virus * * * Tortoise picornavirus Egyptian fruit bat Marburg marburgvirus Banded bullfrog picornavirus * Spanish mole uluguru virus Human Sudan ebolavirus * Black spectacled toad picornavirus * Kilimanjaro virus * * * Crab-eating macaque reston ebolavirus Equine rhinitis A virus Imjin virus * Foot and mouth disease virus Dode virus * Angolan free-tailed bat bombali ebolavirus * * Human cosavirus E Seoul orthohantavirus Little free-tailed bat bombali ebolavirus * African bat icavirus A Tigray hantavirus Human Zaire ebolavirus * Saffold virus * Human choclo virus *Little collared fruit bat ebolavirus Peleg virus * Eastern red scorpionfish picornavirus * Reed vole hantavirus Human bundibugyo ebolavirus * * Isla vista hantavirus * Seal picornavirus Human Tai forest ebolavirus Chicken orivirus Paramyxoviridae 0.4 * Duck picornavirus Hepadnaviridae 0.4 Bildad virus Ned virus Tiger rockfish hepatitis B virus Western African lungfish picornavirus * Pacific spadenose shark paramyxovirus * European eel hepatitis B virus Bluegill picornavirus Nemo virus * Carp picornavirus * African cichlid hepatitis B virus Triplecross lizardfish paramyxovirus * * Fathead minnow picornavirus -

Hepatitis C Virus Vaccine Research: Time to Put up Or Shut Up
viruses Review Hepatitis C Virus Vaccine Research: Time to Put Up or Shut Up Alex S. Hartlage 1,2 and Amit Kapoor 1,3,* 1 Center for Vaccines and Immunity, Abigail Wexner Research Institute at Nationwide Children’s Hospital, Columbus, OH 43205, USA; [email protected] 2 Medical Scientist Training Program, College of Medicine and Public Health, The Ohio State University, Columbus, OH 43205, USA 3 Department of Pediatrics, College of Medicine and Public Health, The Ohio State University, Columbus, OH 43205, USA * Correspondence: [email protected] Abstract: Unless urgently needed to prevent a pandemic, the development of a viral vaccine should follow a rigorous scientific approach. Each vaccine candidate should be designed considering the in- depth knowledge of protective immunity, followed by preclinical studies to assess immunogenicity and safety, and lastly, the evaluation of selected vaccines in human clinical trials. The recently concluded first phase II clinical trial of a human hepatitis C virus (HCV) vaccine followed this approach. Still, despite promising preclinical results, it failed to protect against chronic infection, raising grave concerns about our understanding of protective immunity. This setback, combined with the lack of HCV animal models and availability of new highly effective antivirals, has fueled ongoing discussions of using a controlled human infection model (CHIM) to test new HCV vaccine candidates. Before taking on such an approach, however, we must carefully weigh all the ethical and health consequences of human infection in the absence of a complete understanding of HCV immunity and pathogenesis. We know that there are significant gaps in our knowledge of adaptive immunity necessary to prevent chronic HCV infection. -

Ribavirin Inhibits West Nile Virus Replication and Cytopathic Effect in Neural Cells
1214 CONCISE COMMUNICATION Ribavirin Inhibits West Nile Virus Replication and Cytopathic Effect in Neural Cells Ingo Jordan,1 Thomas Briese,1 Nicole Fischer,1 1Emerging Diseases Laboratory, Departments of Microbiology Johnson Yiu-Nam Lau,2 and W. Ian Lipkin1 and Molecular Genetics, Neurology, and Anatomy and Neurobiology, University of California, Irvine, and 2ICN Pharmaceuticals, Costa Mesa, California West Nile virus (WNV) is an emerging mosquito-borne pathogen that was reported for the ®rst time in the Western hemisphere in August 1999, when an encephalitis outbreak in New York City resulted in 62 clinical cases and 7 deaths. WNV, for which no antiviral therapy has been described, was recently recovered from a pool of mosquitoes collected in New York City. In anticipation of the recurrence of WNV during the summer of 2000, an analysis was made of the ef®cacy of the nucleoside analogue ribavirin, a broad-spectrum antiviral compound with activity against several RNA viruses, for treatment of WNV infection. High doses of ribavirin were found to inhibit WNV replication and cytopathogenicity in human neural cells in vitro. The Flaviviridae, a family of enveloped positive-strand RNA substantial [3]. Genetic analysis of the envelope protein se- viruses, include West Nile virus (WNV), as well as other sig- quence indicated that the viral strain most closely resembled ni®cant human pathogens, such as hepatitis C, yellow fever, an isolate from a goose in Israel in 1998, demonstrating the dengue, Japanese encephalitis, and St. Louis encephalitis vi- wide geographic distribution of this emerging pathogen [4, 5]. ruses [1]. Whereas hepatitis C virus (genus Hepacivirus) may Antiviral therapy for hepatitis C has been described [6]; how- be transmitted by blood products or sexual activity, most mem- ever, no speci®c treatment has been reported for WNV or other bers of the Flavivirus genus, including WNV, are transmitted ¯avivirus infections. -
Conventional and Unconventional Mechanisms for Capping Viral Mrna
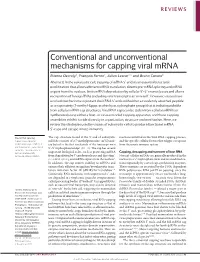
REVIEWS Conventional and unconventional mechanisms for capping viral mRNA Etienne Decroly1, François Ferron1, Julien Lescar1,2 and Bruno Canard1 Abstract | In the eukaryotic cell, capping of mRNA 5′ ends is an essential structural modification that allows efficient mRNA translation, directs pre-mRNA splicing and mRNA export from the nucleus, limits mRNA degradation by cellular 5′–3′ exonucleases and allows recognition of foreign RNAs (including viral transcripts) as ‘non-self’. However, viruses have evolved mechanisms to protect their RNA 5′ ends with either a covalently attached peptide or a cap moiety (7‑methyl-Gppp, in which p is a phosphate group) that is indistinguishable from cellular mRNA cap structures. Viral RNA caps can be stolen from cellular mRNAs or synthesized using either a host- or virus-encoded capping apparatus, and these capping assemblies exhibit a wide diversity in organization, structure and mechanism. Here, we review the strategies used by viruses of eukaryotic cells to produce functional mRNA 5′-caps and escape innate immunity. Pre-mRNA splicing The cap structure found at the 5′ end of eukaryotic reactions involved in the viral RNA-capping process, A post-transcriptional mRNAs consists of a 7‑methylguanosine (m7G) moi‑ and the specific cellular factors that trigger a response modification of pre-mRNA, in ety linked to the first nucleotide of the transcript via a from the innate immune system. which introns are excised and 5′–5′ triphosphate bridge1 (FIG. 1a). The cap has several exons are joined in order to form a translationally important biological roles, such as protecting mRNA Capping, decapping and turnover of host RNA functional, mature mRNA. -

Medcruise News
MEDCRUISE Newsletter Issue 31-new1-3 22/02/2011 15:29 Page 1 MedCruise News CELEBRATING 15 YEARS 1996-2011 March 2011 | Issue 31 IN THIS ISSUE Association News/People 1-3 MedCruise at Seatrade Med Port facilities & Infrastructure 4-14 Patras 4 Kefalonia 4 Heraklion 4 Kavala 5 Kos 5 Igoumenitsa 5 Istanbul 6 Kusadasi, Bodrum & Antalya 6 Rize 7 Portimao 7 MedCruise comes together in Yalta 7 Trieste 8 Cannes at Seatrade Med Ravenna 8 Livorno 8 edCruise held its 37th General MedCruise was also well represented at the Genoa 8 Conference sessions with Board members Assembly in Cannes, France, on Venice 8 December 2nd, 2010 on the Giovanni Spadoni and Carla Salvado invited M Koper 9 occasion of Seatrade Med Cruise Convention, to speak at the Port Development session Split 9 hosted by the French Riviera Cruise Club. whilst Snijezana Papes joined the Upscale The event was held at Cannes’ famous Palais Cruising panel. Dubrovnik 9 des Festivals et des Congrès. Topics discussed by the assembly Rijeka 9 Greek deputy minister of culture and included waste management at ports, Barcelona 10 joining efforts with other regions on finding tourism, George Nikitiadis, addressed the Valencia 10 assembly to confirm the importance of solutions to reducing at-port ship Cartagena 10 cruise tourism in Greece, proven by the emissions, the selection of a cruise port admission to MedCruise of six Greek port benchmarking consultant, the creation of Palamos 10 members at Cannes. MedCruise ‘day Tarragona 11 The assembly voted in The assembly voted in workshops’ on cruise Almeria 11 a record number of new port operations, and the Malaga 11 a record number of MedCruise 2010 members – eleven port Gibraltar 11 members and six new members. -

Structure Unveils Relationships Between RNA Virus Polymerases
viruses Article Structure Unveils Relationships between RNA Virus Polymerases Heli A. M. Mönttinen † , Janne J. Ravantti * and Minna M. Poranen * Molecular and Integrative Biosciences Research Programme, Faculty of Biological and Environmental Sciences, University of Helsinki, Viikki Biocenter 1, P.O. Box 56 (Viikinkaari 9), 00014 Helsinki, Finland; heli.monttinen@helsinki.fi * Correspondence: janne.ravantti@helsinki.fi (J.J.R.); minna.poranen@helsinki.fi (M.M.P.); Tel.: +358-2941-59110 (M.M.P.) † Present address: Institute of Biotechnology, Helsinki Institute of Life Sciences (HiLIFE), University of Helsinki, Viikki Biocenter 2, P.O. Box 56 (Viikinkaari 5), 00014 Helsinki, Finland. Abstract: RNA viruses are the fastest evolving known biological entities. Consequently, the sequence similarity between homologous viral proteins disappears quickly, limiting the usability of traditional sequence-based phylogenetic methods in the reconstruction of relationships and evolutionary history among RNA viruses. Protein structures, however, typically evolve more slowly than sequences, and structural similarity can still be evident, when no sequence similarity can be detected. Here, we used an automated structural comparison method, homologous structure finder, for comprehensive comparisons of viral RNA-dependent RNA polymerases (RdRps). We identified a common structural core of 231 residues for all the structurally characterized viral RdRps, covering segmented and non-segmented negative-sense, positive-sense, and double-stranded RNA viruses infecting both prokaryotic and eukaryotic hosts. The grouping and branching of the viral RdRps in the structure- based phylogenetic tree follow their functional differentiation. The RdRps using protein primer, RNA primer, or self-priming mechanisms have evolved independently of each other, and the RdRps cluster into two large branches based on the used transcription mechanism. -

Cruise Ship Owners/Operators and Passenger Ship Financing & Management Companies
More than a Directory! Cruise Ship Owners/Operators and Passenger Ship Financing & Management Companies 1st Edition, April 2013 © 2013 by J. R. Kuehmayer www.amem.at Cruise Ship Owners / Operators Preface The AMEM Publication “Cruise Ship Owners/Operators and Passenger Ship Financing & Management Compa- nies” in fact is more than a directory! Company co-ordinates It is not only the most comprehensively and accurately structured listing of cruise ship owners and operators in the industry, despite the fact that the majority of cruise lines is more and more keeping both the company’s coordinates and the managerial staff secret. The entire industry is obtrusively focused on selling their services weeks and months ahead of the specific cruise date, collecting the money at a premature stage and staying almost unattainable for their clients pre and after cruise requests. They simply ignore the fact that there are suppliers and partners around who wish to keep in touch personally at least with the cruise line’s technical and procurement departments! The rest of the networking-information is camouflaged by the yellow-pages industry, which is facing a real prospect of extinction. The economic downturn is sending the already ailing business into a tailspin. The yellow-pages publishers basically give back in one downturn what took seven years to grow! Cruise Ship Financing It is more than a directory as it unveils the shift in the ship financing sector and uncovers how fast the traditional financiers to the cruise shipping industry fade away and perverted forms of financing are gaining ground. Admittedly there are some traditional banks around, which can maintain their market position through a blend of sober judgements, judicious risk management and solid relationships.