Current Scenario of Sars-Coronavirus 2: Epidemiology; Post-Covid-19 and Global Impacts
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Update Review of Globally Reported SARS-Cov-2 Vaccines in Preclinical and Clinical Stages
International Immunopharmacology 96 (2021) 107763 Contents lists available at ScienceDirect International Immunopharmacology journal homepage: www.elsevier.com/locate/intimp Review An update review of globally reported SARS-CoV-2 vaccines in preclinical and clinical stages Hamid Motamedi a, Marzie Mahdizade Ari b, Shirin Dashtbin b, Matin Fathollahi a, Hadi Hossainpour a, Amirhoushang Alvandi a,c, Jale Moradi a, Ramin Abiri a,d,* a Department of Microbiology, School of Medicine, Kermanshah University of Medical Sciences, Kermanshah, Iran b Department of Microbiology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran c Medical Technology Research Center, Health Technology Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran d Fertility and Infertility Research Center, Health Technology Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran ARTICLE INFO ABSTRACT Keywords: Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the causative agent of the rapidly spreading COVID-19 pandemic COVID-19 in the world. As an effective therapeutic strategy is not introduced yet and the rapid genetic SARS-CoV-2 variations in the virus, there is an emerging necessity to design, evaluate and apply effective new vaccines. An Vaccines acceptable vaccine must elicit both humoral and cellular immune responses, must have the least side effects and the storage and transport systems should be available and affordable for all countries. These vaccines can be classified into different types: inactivated vaccines, live-attenuated virus vaccines, subunit vaccines, virus-like particles (VLPs), nucleic acid-based vaccines (DNA and RNA) and recombinant vector-based vaccines (repli cating and non-replicating viral vector). According to the latest update of the WHO report on April 2nd, 2021, at least 85 vaccine candidates were being studied in clinical trial phases and 184 candidate vaccines were being evaluated in pre-clinical stages. -
Cuba: One Year Into the Pandemic
BULLETIN OF PAHO/WHO IN CUBA Vol. 25 No.1 JANUARY-MARCH 2021 CUBA: ONE YEAR INTO THE PANDEMIC 04 43 46 50 OUR NEWS: NOTEWORTHY: OVER A STORY A CUP OF TO TELL: Interview Benefits with Cuba's of a Cúrcumal onga COFFEE Dr. Ricardo Minister pdroject uring WITH… Pereda González: of Public Health, thep andemic Coordinator of Dr. José Angel Concepción the COVID-19 Clinical Portal Miranda Campa Experts Commission Huergo Pathways to Health is a bulletin prepared by the office of the Pan American Health Organization/World Health Organization EDITORIAL (PAHO/WHO) in Cuba. Its main aim is to share the most important aspects of the On March 11, 2020, the Director-General of the World Health Representation's technical cooperation with Organization (WHO) declared the novel coronavirus a pandemic, the country's Ministry of Public Health which at the time already affected 114 nations. Coincidentally, (MINSAP) and other institutions. that same day, the Pedro Kourí Tropical Medicine Institute (IPK) in Havana confirmed the first COVID-19 cases in Cuba. At the one-year anniversary of the pandemic in Cuba, this issue is dedicated to One year into the pandemic, more than 115 million cases and close to 2.6 million deaths have been reported from the disease systematically review key aspects of the worldwide. About half of both these cases and deaths have been national response over the last months. In registered in the Americas, with results differing according to how particular, it includes an interview with the well the response has been organized, how robust the healthcare Minister of Public Health, Dr. -

Updated May 26, 2021 Cross-Border Industry Partnerships on COVID-19 Vaccines and Therapeutics Vaccines • Curevac O Celonic Wi
Updated May 26, 2021 Cross-Border Industry Partnerships on COVID-19 Vaccines and Therapeutics Vaccines • CureVac o Celonic will manufacture 100 million doses of CureVac’s vaccine at its plant in Heidelberg, Germany, providing bulk substance for 50 million doses by the end of 2021. (press release) o Novartis will manufacture CureVac’s vaccine. (press release) o GlaxoSmithKline plc and CureVac N.V. announced a new €150m collaboration, building on their existing relationship, to jointly develop next generation mRNA vaccines for COVID-19 with the potential for a multi-valent approach to address multiple emerging variants in one vaccine. (press release) o Rentschler Biopharma SE will manufacture CureVac’s vaccine. (press release) o Bayer will support the further development, supply and key territory operations of CureVac’s vaccine candidate. (press release) o Fareva will dedicate a manufacturing plant in France to the fill and finish of CureVac’s vaccine. (press release) o Wacker Chemie AG will manufacture CureVac’s vaccine candidate at its Amsterdam site. (press release) o CureVac will collaborate with Tesla Grohmann Automation to develop an RNA printer that works like a mini-factory and can produce such drugs automatically. (press release) • Moderna o Samsung Biologics will provide large scale, commercial fill-finish manufacturing for Moderna’s vaccine in South Korea. (press release) o Baxter International will provide fill/finish services and supply packaging for Moderna. (press release) o Sanofi will manufacture 200 million doses of Moderna’s COVID-19 vaccine starting in September 2021. (press release) o Rovi will produce bulk substance for Moderna’s COVID-19 vaccine, expanding an agreement between the companies. -

Microsoft Outlook
Morris, Max From: Morris, Max Sent: Monday, March 22, 2021 11:38 PM To: Morris, Max Subject: 03/22/2021 Coronavirus Daily Recap This email is provided for informational, non-commercial purposes only. Use or reliance on the information contained in this email is at your sole risk. This email is not provided by or affiliated in any way with Ally Financial Inc. These updates are being shared to multiple organizations, individuals and lists who/which are bcc’d. Best effort we are sending Daily updates during the business week, typically in the evening, a Weekend Recap on Monday mornings, and any significant breaking news events provided anytime. Please note some numbers included in the Statistics and news stories come from various sources and so can vary as they are constantly changing and not reported at the same time. All communications are TLP GREEN and can be shared freely. Know someone who might want to be added to our Updates? Of course ask them first, and then have them send us an email to [email protected]. Live the message, share the message: Be safe – Stay home and limit travel as much as possible, self-quarantine if you or any members of your family are or may be sick, if you go out wear your mask – the right way, ensure safe social distancing, and practice good hygiene – wash your hands, avoid touching your face, and sanitize used items and surfaces. Need to find a vaccine? Here are a few good sites and resources we have come across that may help: CDC Vaccine Finder – https://vaccinefinder.org/ [Free government website where users can search for pharmacies and providers that offer vaccinations, currently limited number of states but expanding] Dr. -

COVID-19 Situation Report 210
For citation: Centre for Infectious Disease Epidemiology and Research-NUS. COVID-19 Situation Report 210. 27 August 2020 Aug 27 COVID-19 Situation Report 210 Centre for Infectious Disease Epidemiology and Research (CIDER) For citation: Centre for Infectious Disease Epidemiology and Research-NUS. COVID-19 Situation Report 210. 27 August 2020 i. Background In December, China notified the World Health Organization (WHO) of several cases of human respiratory illness, which appeared to be linked to an open seafood and livestock market in the city of Wuhan. The infecting agent has since been identified as a novel coronavirus, previously known as 2019-nCoV and now called SAR-CoV-2; The new name of the disease has also been termed COVID-19, as of 11th February 2020. Although the virus is presumed zoonotic in origin, person-to-person spread is evident. Screening of travellers, travel bans and quarantine measures are being implemented in many countries. Despite these precautions, it is anticipated that more cases will be seen both inside China and internationally. The WHO declared the outbreak of COVID-19 constitutes a Public Health Emergency of International Concern on 30 January. On 11 March, 2020, WHO declared the coronavirus outbreak a pandemic as the global death toll rose above 4,600 and the number of confirmed cases topped 125,000. This report aims to update Global Risk Assessment, Global Epidemiology, Quarantine Orders, Travel Ban/Advisory by countries, WHO’s and CDC’s Guidance and Protocols and Scientific publication on a daily basis. New updates in the tables are bolded. 1 | P a g e Centre for infectious di sease epidemiology and research For citation: Centre for Infectious Disease Epidemiology and Research-NUS. -

COVID-19 Vaccination Programme: Information for Healthcare Practitioners
COVID-19 vaccination programme Information for healthcare practitioners Republished 6 August 2021 Version 3.10 1 COVID-19 vaccination programme: Information for healthcare practitioners Document information This document was originally published provisionally, ahead of authorisation of any COVID-19 vaccine in the UK, to provide information to those involved in the COVID-19 national vaccination programme before it began in December 2020. Following authorisation for temporary supply by the UK Department of Health and Social Care and the Medicines and Healthcare products Regulatory Agency being given to the COVID-19 Vaccine Pfizer BioNTech on 2 December 2020, the COVID-19 Vaccine AstraZeneca on 30 December 2020 and the COVID-19 Vaccine Moderna on 8 January 2021, this document has been updated to provide specific information about the storage and preparation of these vaccines. Information about any other COVID-19 vaccines which are given regulatory approval will be added when this occurs. The information in this document was correct at time of publication. As COVID-19 is an evolving disease, much is still being learned about both the disease and the vaccines which have been developed to prevent it. For this reason, some information may change. Updates will be made to this document as new information becomes available. Please use the online version to ensure you are accessing the latest version. 2 COVID-19 vaccination programme: Information for healthcare practitioners Document revision information Version Details Date number 1.0 Document created 27 November 2020 2.0 Vaccine specific information about the COVID-19 mRNA 4 Vaccine BNT162b2 (Pfizer BioNTech) added December 2020 2.1 1. -
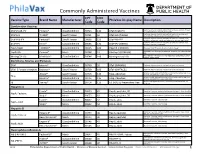
Commonly Administered Vaccines
Commonly Administered Vaccines CPT CVX Vaccine Type Brand Name Manufacturer PhilaVax Display Name Description Code Code Combination Vaccines Diptheria, tetanus toxoids and acellular pertussis vaccine, Hepati- DTaP-HepB-IPV Pediarix® GlaxoSmithKline 90723 110 DTaP-HepB-IPV tis B and poliovirus vaccine, inactivated Diptheria, tetanus toxoids and acellular pertussis vaccine and DTaP-Hib TriHIBit® Sanofi Pasteur 90721 50 DTaP-Hib (TriHIBit) Haemophilus influenzae type b conjugate vaccine Diptheria, tetanus toxoids and acellular pertussis vaccine, Hae- DTaP-Hib-IPV Pentacel® Sanofi Pasteur 90698 120 DTaP-Hib-IPV mophilus influenzae type b, and poliovirus vaccine, inactivated Diptheria, tetanus toxoids and acellular pertussis vaccine, and DTaP-IPV Kinrix® GlaxoSmithKline 90696 130 DTaP-IPV (KINRIX) poliovirus vaccine, inactivated HepA-HepB TWINRIX® GlaxoSmithKline 90636 104 HepA/B (TWINRIX) Hepatisis A and Hepatitis B vaccine, adult dosage Hepatitis B and Hemophilus influenza b vaccine, for intramuscular HepB-Hib Comvax® Merck 90748 51 Hib-Hep B (COMVAX) use Haemophilus influenza b and meningococcal sero groups C and Y MeningC/Y-Hib Menhibrix® GlaxoSmithKline 90644 148 Meningococcal-Hib vaccine, 4 dose series Diphtheria, Tetanus and Pertussis DTaP Infanrix® GlaxoSmithKline 90700 20 DTaP (INFANRIX) Diptheria, tetanus toxoids and acellular pertussis vaccine DTaP, 5 Pertussis Antigens Daptacel® Sanofi Pasteur 90700 106 DTaP (DAPTACEL) Diptheria, tetanus toxoids and acellular pertussis vaccine Tetanus toxoid, reduced diphtheria toxoid, and acellular -

Vaccins Contre La Covid-19 Et Utilisation De Cellules D'origine Fœtale
Vaccins contre la Covid-19 et utilisation de cellules d’origine fœtale : un questionnement éthique pour les chrétiens. Dr Michel Cambrelin La pandémie Covid-19 due au nouveau Coronavirus SARS-CoV-2 n’épargne pas nos sociétés occidentales, qui sont fortement ébranlées malgré leur richesse et leur technologie, et notre pays ne fait pas exception1. Après les échecs successifs des tentatives de contenir cette épidémie, la vaccination nous est présentée comme la planche de salut. Cette vaccination a pour principe de présenter à l’organisme receveur des éléments inoffensifs appartenant au virus, ce qui va lui permettre de fabriquer des anticorps prêts à le défendre lorsque le virus essaiera de le pénétrer. Pour ces vaccins différentes techniques ont été utilisées, qui pour certaines sont assez nouvelles, que nous expliquerons plus loin. De multiples questions et rumeurs circulent sur les vaccins Covid en particulier à ARN messager (ARNm), auxquelles l’OMS2 et la Société de Pathologie Infectieuse de Langue Française3 ont apporté leurs réponses. Bien que les Français y semblaient réticents au départ, une politique de vaccination croissante se met en place, dont on critique maintenant la lenteur du démarrage. Cependant une autre question interpelle les chrétiens, respectueux de la vie humaine constituant un don de Dieu dès la conception4, question qui n’est pas abordée dans les médias ni dans les recommandations scientifiques : certains vaccins contre la Covid auraient été élaborés à l’aide de cellules de fœtus avortés ! Nous allons tenter d’apporter les éléments de réponse nécessaires à cette question, qui semble ignorée du débat public, sans aborder les autres questions d’innocuité et d’efficacité de ces vaccins qui ont aussi leur importance éthique. -

Vaccine Hesitancy
Vaccine Hesitancy Dr Brenda Corcoran National Immunisation Office Presentation Outline An understanding of the following principles: • Overview of immunity • Different types of vaccines and vaccine contents • Vaccine failures • Time intervals between vaccine doses • Vaccine overload • Adverse reactions • Herd immunity Immunity Immunity • The ability of the human body to protect itself from infectious disease The immune system • Cells with a protective function in the – bone marrow – thymus – lymphatic system of ducts and nodes – spleen –blood Types of immunity Source: http://en.wikipedia.org/wiki/Immunological_memory Natural (innate) immunity Non-specific mechanisms – Physical barriers • skin and mucous membranes – Chemical barriers • gastric and digestive enzymes – Cellular and protein secretions • phagocytes, macrophages, complement system ** No “memory” of protection exists afterwards ** Passive immunity – adaptive mechanisms Natural • maternal transfer of antibodies to infant via placenta Artificial • administration of pre- formed substance to provide immediate but short-term protection (antitoxin, antibodies) Protection is temporary and wanes with time (usually few months) Active immunity – adaptive mechanisms Natural • following contact with organism Artificial • administration of agent to stimulate immune response (immunisation) Acquired through contact with an micro-organism Protection produced by individual’s own immune system Protection often life-long but may need boosting How vaccines work • Induce active immunity – Immunity and immunologic memory similar to natural infection but without risk of disease • Immunological memory allows – Rapid recognition and response to pathogen – Prevent or modify effect of disease Live attenuated vaccines Weakened viruses /bacteria – Achieved by growing numerous generations in laboratory – Produces long lasting immune response after one or two doses – Stimulates immune system to react as it does to natural infection – Can cause mild form of the disease (e.g. -

National Emergency Management Organisation (Nemo) Ministry of National Security St
NATIONAL EMERGENCY MANAGEMENT ORGANISATION (NEMO) MINISTRY OF NATIONAL SECURITY ST. VINCENT AND THE GRENADINES WEST INDIES Tel: 784-456-2975, Fax: 784-457-1691, Email: [email protected] or [email protected] ______________________________________________________________________________ ___________________________________________________________________________________________________________________ HEALTH SERVICES SUBCOMMITTEE PROTOCOL FOR THE ENTRY OF FULLY VACCINATED TRAVELLERS TO ST. VINCENT AND THE GRENADINES – revised 10/08/2021 AIM: The safe entry of travellers to St. Vincent and the Grenadines in a manner that reduces the risk of the importation and subsequent transmission of COVID-19 in St. Vincent and the Grenadines. OBJECTIVES: 1. To establish the risk of the arriving traveller introducing new COVID-19 cases to SVG; 2. To minimize exposure of residents of SVG to new COVID-19 cases; 3. Early identification of potential exposure to COVID-19 and 4. Early containment of new COVID-19 cases. ESTABLISH RISK OF ARRIVING TRAVELLER: The arriving traveller will: 1. Complete the Pre-Arrival Form available at health.gov.vc And the Port Health Officer will: 1. Review Port Health form for each arriving passenger. 1 PHASED PROCESS OF ENTRY OF FULLY VACCINATED TRAVELERS TO ST. VINCENT AND THE GRENADINES: TESTING & QUARANTINE: PHASE #16 - Commencing Wednesday, August 11, 2021: 1. Where ‘Fully Vaccinated Travelers’ are those persons who: a. Have completed a vaccination regimen with one of the following COVID-19 vaccines recognized by the Ministry of Health, Wellness and the Environment of St Vincent and the Grenadines: i. AstraZeneca – Oxford AstraZeneca (Vaxzevria), COVISHIELD, AstraZeneca COVID-19 vaccine by SK Bioscience; ii. Pfizer-BioNTech COVID-19 vaccine; iii. Moderna COVID-19 vaccine; iv. -
Criteria for Reviewing Pneumococcal Conjugate Vaccine
Draft—3/11/10 Oregon School/Facility Immunization Advisory Committee: Review of Pneumococcal Conjugate Vaccine Against Twelve Criteria for Children’s Facility Immunization Requirements Oregon Department of Human Services Public Health Division Office of Family Health Immunization Program 800 NE Oregon Street, Suite 370 Portland, Oregon 97232 Phone: 971-673-0300 Fax: 971-673-0278 Web: www.oregon.gov/DHS/ph/imm Page 1–Review of Pneumococcal Conjugate Vaccine Against Criteria for School Law Immunization Requirements Oregon School/Facility Immunization Advisory Committee: Review of Pneumococcal Conjugate Vaccine Against Twelve Criteria for School/Facility/College Immunization Requirements Process for Reviewing Antigens for Potential Inclusion in OAR 333-050-0050, 333-050-0130 and 333-050-0140. Request for the inclusion of additional antigens or vaccines can come from the Oregon Immunization Program, IPAT (Immunization Policy Advisory Team), or from the community. Proposed changes to vaccine requirements are discussed with IPAT either in a regularly scheduled meeting or through electronic communication. IPAT will submit their comments and a request for consideration to the Oregon Immunization School Law Advisory Committee. The Oregon School/Facility Immunization Advisory Committee was established as a part of the school law immunization requirements when the original legislation was passed in 1980. This Committee is composed of immunization stakeholders from the fields of public health, school health, school administration, medicine, day care, child advocacy and consumers (parents). Through consensus, the committee determines what vaccines (antigens) should be included in Oregon school immunization requirements. Information about new vaccines and the diseases they prevent, including transmission within schools, burden of disease, cost-effectiveness, effect on schools/counties and vaccine availability is presented at a scheduled meeting for committee consideration. -

Revision Rápida
REVISION RÁPIDA EVALUACIÓN DE LAS CARACTERÍSTICAS DE ALMACENAMIENTO, TRANSPORTE Y DISTRIBUCIÓN DE LAS VACUNAS COVID-19 EN ESTUDIO, Y LAS CARACTERÍSTICAS CLÍNICAS DE LA POBLACIÓN CANDIDATA A VACUNACIÓN Noviembre de 2020 El Instituto de Evaluación Tecnológica en Salud – IETS, es una corporación sin ánimo de lucro, de participación mixta y de carácter privado, con patrimonio propio, creado según lo estipulado en la Ley 1438 de 2011. Su misión es contribuir al desarrollo de mejores políticas públicas y prácticas asistenciales en salud, mediante la producción de información basada en evidencia, a través de la evaluación de tecnologías en salud y guías de práctica clínica, con rigor técnico, independencia y participación. Sus miembros son el Ministerio de Salud y Protección Social – MinSalud, el Departamento Administrativo de Ciencia, Tecnología e Innovación – Colciencias, el Instituto Nacional de Vigilancia de Medicamentos y Alimentos – INVIMA, el Instituto Nacional de Salud – INS, la Asociación Colombiana de Facultades de Medicina – ASCOFAME y la Asociación Colombiana de Sociedades Científicas – ACSC. Autores Lucas López Quiceno. Médico y cirujano, Especialista en Epidemiología, Magister en Epidemiología, Magíster en economía de la salud (c). Instituto de Evaluación Tecnológica en Salud - IETS. Jhyld Carolaind Camacho Barbosa, Nutricionista y Dietista, Magister en Epidemiología. Instituto de Evaluación Tecnológica en Salud - IETS. Kelly Estrada-Orozco. Médica, Magister en Epidemiología Clínica, Magister en Neurociencia. Doctorado en Salud Pública (actual). Doctorado en Epidemiología Clínica (actual). Instituto de Evaluación Tecnológica en Salud - IETS. Revisores Cortes-Muñoz, Ani Julieth. Bacterióloga y laboratorista clínica. MSc. Epidemiología. Instituto de Evaluación Tecnológica en salud - IETS. Ospina-Lizarazo, Nathalie. Nutricionista Dietista. MSc. Epidemiología Clínica. Instituto de Evaluación Tecnológica en salud - IETS.