Difficult but Not Impossible PAGE 14 Annual Report 2012 Progress Highlights Contents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

EASTERN VISAYAS: SUMMARY of REHABILITATION ACTIVITIES (As of 24 Mar)
EASTERN VISAYAS: SUMMARY OF REHABILITATION ACTIVITIES (as of 24 Mar) Map_OCHA_Region VIII_01_3W_REHAB_24032014_v1 BIRI PALAPAG LAVEZARES SAN JOSE ALLEN ROSARIO BOBON MONDRAGON LAOANG VICTORIA SAN CATARMAN ROQUE MAPANAS CAPUL SAN CATUBIG ANTONIO PAMBUJAN GAMAY N O R T H E R N S A M A R LAPINIG SAN SAN ISIDRO VICENTE LOPE DE VEGA LAS NAVAS SILVINO LOBOS JIPAPAD ARTECHE SAN POLICARPIO CALBAYOG CITY MATUGUINAO MASLOG ORAS SANTA GANDARA TAGAPUL-AN MARGARITA DOLORES SAN JOSE DE BUAN SAN JORGE CAN-AVID PAGSANGHAN MOTIONG ALMAGRO TARANGNAN SANTO PARANAS NI-O (WRIGHT) TAFT CITY OF JIABONG CATBALOGAN SULAT MARIPIPI W E S T E R N S A M A R B I L I R A N SAN JULIAN KAWAYAN SAN SEBASTIAN ZUMARRAGA HINABANGAN CULABA ALMERIA CALBIGA E A S T E R N S A M A R NAVAL DARAM CITY OF BORONGAN CAIBIRAN PINABACDAO BILIRAN TALALORA VILLAREAL CALUBIAN CABUCGAYAN SANTA RITA BALANGKAYAN MAYDOLONG SAN BABATNGON ISIDRO BASEY BARUGO LLORENTE LEYTE SAN HERNANI TABANGO MIGUEL CAPOOCAN ALANGALANG MARABUT BALANGIGA TACLOBAN GENERAL TUNGA VILLABA CITY MACARTHUR CARIGARA SALCEDO SANTA LAWAAN QUINAPONDAN MATAG-OB KANANGA JARO FE PALO TANAUAN PASTRANA ORMOC CITY GIPORLOS PALOMPON MERCEDES DAGAMI TABONTABON JULITA TOLOSA GUIUAN ISABEL MERIDA BURAUEN DULAG ALBUERA LA PAZ MAYORGA L E Y T E MACARTHUR JAVIER (BUGHO) CITY OF BAYBAY ABUYOG MAHAPLAG INOPACAN SILAGO HINDANG SOGOD Legend HINUNANGAN HILONGOS BONTOC Response activities LIBAGON Administrative limits HINUNDAYAN BATO per Municipality SAINT BERNARD ANAHAWAN Province boundary MATALOM SAN JUAN TOMAS (CABALIAN) OPPUS Municipality boundary MALITBOG S O U T H E R N L E Y T E Ongoing rehabilitation Ongoing MAASIN CITY activites LILOAN MACROHON PADRE BURGOS SAN 1-30 Planned FRANCISCO SAN 30-60 RICARDO LIMASAWA PINTUYAN 60-90 Data sources:OCHA,Clusters 0 325 K650 975 1,300 1,625 90-121 Kilometers EASTERN VISAYAS:SUMMARY OF REHABILITATION ACTIVITIES AS OF 24th Mar 2014 Early Food Sec. -

2014 Annual Report a CONTENTS 2 Message from the Board of Trustees
2014 Annual Report a CONTENTS 2 Message from the Board of Trustees 6 PROTOTYPING Going where health inequities are most challenging 18 COVER STORY Attaining better health outcomes is our bottom line 22 EXPANSION Partnership: Creating added value, innovating and reaching more areas 34 REPLICATION On the way to influencing the national impact 42 MOVING FORWARD Onward to quest for improved health outcomes 46 Financial Highlights 48 Management and Staff Lilybelle Bakil is a 35-year-old mother of six living in Malacca village in Panglima Sugala, Tawi-Tawi. Her municipality became part of Zuellig Family Foundation’s prototype municipalities—under Cohort 3—in 2011. In this town, among the health programs introduced to ensure better health is the use of the Wireless Access for Health (WAH) technology. With this, pregnancy cases like Lilybelle’s are tracked and monitored regularly by municipal health personnel. In the Autonomous Region in Muslim Mindanao, health is not devolved to the local government units (LGUs) unlike in the rest of the country. Despite the difference, ZFF has seen its Health Change Model remaining effective in most of its ARMM LGUs. In Panglima Sugala, there has been no maternal death since 2012. Leadership changed when then municipal mayor Nurbert Sahali was elected provincial governor in 2013. He was succeeded by his sister Rejie Sahali, who has kept health on top of her administration’s priority. b Zuellig Family Foundation 2014 SNAPSHOT A Based on ZFF’s internal funds and co-financed funds (UNFPA, UNICEF, USAID, and MSD) spent, and brokered funds based on the Department of Health’s approved budget for its partnership program with ZFF. -

Palapag-Mapanas-Gamay
\.-7 .- Republic of the Philippines DEPARTMENT OF PUBLIC WORKS AND HIGHWAYS NORTHERI{ SAMAR 2lrD DISTRICT ENGINEERING OFFICE REGIONAL OFFICE t{O. VHI Brgy, Burabud, Laoang, Northern Samar Telephone No./Fax No. 2518254 INVITATION TO BID FOR REMEDIAL MEASURE ON DAMAGED ROAD ALOI{G PAI{GPANG. PALAPAG-MAPANAS-GAMAY-LAPINIG ROAD, CABATUAN-MAGTAON SECTION, KO820+900 The Departsnent of Public works and Highways - Northern Samar Second District Engineering Office, through its Eids and Awards Committee (BAC) invites suppliers to submit bids for the following Contract: Contract ID No. 21Grr0001 Remedial Measure on Damaged Road along Pangpang-Palapag- Contract Name MaDanas-Gamay-Lapiniq Road, Cabatuan-lvaqtaon *ction, K0820+900 Contract Location PalaDao, Northern Samar 1. Installation of additional Four (4) pcs. Reinforced Concrete Pipe Brief Description of Cuivert (RCPC), 910mm diameter (36?) Goods to be Procured 2. Construction of 20 Linear meter Detour, (4.00m x 30.00m) Approved Budget for Pho 499.628.14 the Contract Source of Funds GOP Delivery Date of Goods/Contract 30 Cnlendar Days Durauon Service The BAC is conduding the public bidding for this Contract in accordance with RA 9184 and its Implementing Rules and Regulations. Bidders should have completed, within from the date of submission and receipt of bids, a contract similar to the Project. The description of an eligible bidder is contained in the Bidding Documents, particularty, in Section IV Instrudion to Bidders. To be eligible to bid for this Contract, a supplier must meet the following -

World Bank Document
39386 Public Disclosure Authorized Paper No. 102 / January 2007 Public Disclosure Authorized Measuring the Costs and Benefits of Community Driven Development: The KALAHI-CIDSS Project, Philippines Public Disclosure Authorized Eduardo Araral Camilla Holmemo Public Disclosure Authorized Summary Findings The main focus of this analysis is the economic impacts of the KALAHI-CIDSS project. It looks at the costs and benefits of seven major subproject (SP) categories that cover 1,175 completed and ongoing subprojects (e.g., domestic water supply [both pump and gravity], roads construction and improvement, elementary school buildings, barangay health centers, and day care centers). These seven major categories accounted for 82 percent of total subproject costs. The main findings from the analysis are: 1. The Project overall is economically beneficial. Based on available information and plausible assumptions, the Project overall will generate a conservatively estimated economic internal rate of return of 21 percent and a net present value of Philippine peso (PHP) 1.03 billion. It is therefore considered economically beneficial. The rates of return for the subprojects ranged from 16 percent for day care centers to 65 percent for water supply projects. These results are conservative, considering that other benefits and subprojects were not examined, including benefits from investments to strengthen community participation and local governance. 2. The Project overall is sensitive to a 20 percent increase in costs and 20 percent benefit reduction, with some subprojects more sensitive than others. For the major subproject categories, we show that rates of return for road improvement and school building subprojects are highly sensitive to a 20 percent increase in costs; they are moderately sensitive for health and day care centers, and are not as sensitive for water supply (gravity and pump) and new road construction. -

Total Total 0 0 2 0 0 0 0 0 0 1 0 0 21 0 1 0 24 94
PHILIPPINES: Summary of Completed Response Activities (as of 7 December 2013) Reg. Prov. Total IV-B Occidental Mindoro 0 0 0 2 0 0 0 0 0 2 Palawan 0 0 0 0 0 0 0 0 1 1 VI Aklan 0 0 0 0 0 0 0 0 0 0 Antique 1 0 0 4 0 0 0 0 0 5 Capiz 9 4 3 80 14 0 0 0 21 131 Iloilo 5 1 9 29 0 0 0 0 0 44 Negros Occidental 1 0 0 0 0 0 0 0 1 2 VII Bohol 0 0 0 0 0 0 0 0 0 0 Cebu 4 0 33 44 0 1 0 0 24 106 VIII Eastern Samar 3 0 120 14 0 0 1 222 94 454 Leyte 4 71 220 69 14 0 11 115 150 654 Northern Samar 1 0 0 0 0 0 0 0 0 1 Samar 5 0 0 5 0 0 1 0 40 51 Southern Leyte 1 0 0 0 0 0 0 0 0 1 Total 34 76 385 247 28 1 13 337 331 1452 Affected Persons (in thousands) 0 - 250 250-500 500-750 750-1,000 > 1,000 The numbers above represent the number of activties in a sector (or in some cases, subsector) by province. The figures above are almost certainly incomplete. Nevertheless the sectoral and geographic coverage shown above can be considered indicative of the overall response. The Province names are colored based on the number of people affected as reported in the DSWD DROMIC database. -

The Socio-Economic Impact of the Help for Catubig Agricultural Advancement Project (Hcaap)
[Ocaña *, Vol.7 (Iss.5): May 2019] ISSN- 2350-0530(O), ISSN- 2394-3629(P) DOI: https://doi.org/10.29121/granthaalayah.v7.i5.2019.830 Social THE SOCIO-ECONOMIC IMPACT OF THE HELP FOR CATUBIG AGRICULTURAL ADVANCEMENT PROJECT (HCAAP) Eduardo L. Ocaña Jr. *1 *1 Department of Social Sciences, College of Arts and Communication, University of Eastern Philippines, Catarman, Northern Samar, Philippines 6400 Abstract Development must not only focus on economic growth expressed in rosy figures of GDP and GNP. The economic gains of the rich as expected by economists, must “trickle down” down to the grass roots. It is along this reality that prompted the national government and development planners to look for strategy in which the marginalized which constitute the biggest number of the population in the Third World countries become recipients of development initiatives. Northern Samar, one of the poorest provinces in the Philippines, has been a recipient of the Help for Catubig Agricultural Advancement Project (HCAPP), a project of 5.2 billion yen or 3.4 billion in pesos allocating 2.4 billion pesos alone to irrigate 4, 550 hectares of agricultural lands to spur agricultural development in the Catubig Valley area of Northern Samar. This research aimed to determine the level of socio-economic impact of the HCAAP and related problems. The areas covered by the HCAAP were the Municipalities of Catubig and Las Navas both located in the Catubig Valley. A descriptive-evaluative study, utilized quantitative techniques like survey employing interview schedule for data collection and analyses. The respondents were beneficiaries from Municipality of Catubig, and Las Navas. -
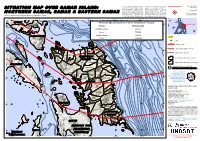
Potentially Affected Population in Samar Island (Eastern Visayas) ¥¦¬ F Map Extent
This map illustrates potentially affected comprise Samar Island. About 620,000 Tropical Cyclone Production Date: areas by the Typhoon Hagupit in Samar people are potentially affected in 09/12/2014 Island, Philippines. Hagupit Typhoon Northern Samar province, ~ 770,000 in made landfall over Philippines on 6 Samar province and ~ 450,000 in Version 1.0 December 2014 causing hurricane force Eastern Samar province. This is a winds and heavy rainfall that have preliminary analysis and has not yet !5 Activation Number: potentially affected ~ 1,800,000 people been validated in the field. Please send ! TC20141204PHL Shuttle Radar Topography Mission (SRTM 3") (90m) in the three different provinces that ground feedback to UNITAR /UNOSAT. 123°30'0"E 124°0'0"E 124°30'0"E 125°0'0"E 125°30'0"E 126°0'0"E Metro Manila Potentially Affected Population in Samar Island (Eastern Visayas) ¥¦¬ F Map Extent Sorsogon 13°0'0"N 13°0'0"N Province Population 2013 City Northern Samar 618,470 Koror¥¦¬ Samar 770,054 ¥¦¬BandarSeriBegawan Eastern Samar 446,218 LEGEND 200 Biri Total 1,834,742 City 3000 1_ Typhoon Track 6500 1_ 4500 5500 5000 2500 Strong Wind Buffer (120 km/h) Lavezares Palapag San 4000 6000 500 San Jose Laoang 12°30'0"N 3500 Bathymetery (Depth m) 12°30'0"N Rosario Roque Pambujan Mapanas Capul Catubig 2000 Victoria Bobon Catarman San Gamay Antonio Administrative Boundary - Province Masbate San Isidro Mondragon Lapinig Lope de Las Silvino 1_San Vega Navas Jipapad Administrative Boundary - Municipality Vicente Lobos Arteche Map Scale for A3: 1:1,000,000 Matuguinao Calbayog San Policarpo I Km ! 0 5 10 20 30 40 50 Oras City Maslog Calbayog Disaster coverage by the Gandara Dolores International Charter 'Space and City Calbayog Santa San Jose Major Disasters'. -

Understanding Community Preferences for the Use and Management of Samar Island Forest Reserve Based on Participatory Rural Appraisap
UNDERSTANDING COMMUNITY PREFERENCES FOR THE USE AND MANAGEMENT OF SAMAR ISLAND FOREST RESERVE BASED ON PARTICIPATORY RURAL APPRAISAP ..'-- USAIO ******* ...-- UNDERSTANDING COMMUNITY PREFERENCES FOR THE USE AND MANAGEMENT OF SAMAR ISLAND FOREST RESERVE BASED ON PARTICIPATORY RURAL APPRAISAL 1 by LUIS P. ELEAZAR2 Institutional! PRA SpE'cialist July 2000 • Samar Island Biodiversity Study (SAMBIO) Resources, Environment and Economics Center for Studies, Inc. (REECS) In association wiTh Tandaya Foundation Eastern Samar Development Foundation, Inc. (ESADEF) Samar Center for Rural Education and Development, Inc. (SACRED) .. I Thi .. publication was made- possible through support provided by Ihe> lJ. S. AgE"ncy for International DE"velopmpnl fl!5AIDl under the INms of Gr.ant No. 492-G-Oo-OO-00001-00. ThE' opinions expressed hNein are those- of the dulnor dod drJ nol npl.f-':-:-arily fenecllhe views of the U. S. Agency for Internalional DE'v€'iopment. Th~-" .\lIlhor. Mr. luis P. Ele..lzar, is the PRA SpE'cialist of SAMBIO, REECS . ... TABLE OF CONTENTS list of Tables list of Figures Executive Summary...........•...........••.•..•.••..•...•........•..•.•..•.•.•....••••.........•.•.....•.•. vi 1. INTRODUCTION...............................................................•..•............•.. 1 .. 1.1 PRA in the Context of SAMBIO . 1 1.2 The PRA Objectives . 2 1.3 The PRA Teams . 2 ... 2. EXPLANATORY NOTES ON PARTICIPATORY RURAL APPRAiSAL.......•• 3 2.1 Why PRA? . 3 2.2 PRA Research Plan . 3 2.3 PRA Sites and Participants . 4 2.4 Methodology of PRA . 6 3. GENERAL CONTEXT OF SAMAR ISLAND...•..••••..•••••...•••.•....•..•.....•.••.•.•• 8 3.1 Background Information . 8 3.2 Land Use . 9 3.3 Local Economy . 11 3.3.1 Agriculture . 13 3.3.2 Cottage Industry . 14 3.3.3 Tourism . -
One Big File
MISSING TARGETS An alternative MDG midterm report NOVEMBER 2007 Missing Targets: An Alternative MDG Midterm Report Social Watch Philippines 2007 Report Copyright 2007 ISSN: 1656-9490 2007 Report Team Isagani R. Serrano, Editor Rene R. Raya, Co-editor Janet R. Carandang, Coordinator Maria Luz R. Anigan, Research Associate Nadja B. Ginete, Research Assistant Rebecca S. Gaddi, Gender Specialist Paul Escober, Data Analyst Joann M. Divinagracia, Data Analyst Lourdes Fernandez, Copy Editor Nanie Gonzales, Lay-out Artist Benjo Laygo, Cover Design Contributors Isagani R. Serrano Ma. Victoria R. Raquiza Rene R. Raya Merci L. Fabros Jonathan D. Ronquillo Rachel O. Morala Jessica Dator-Bercilla Victoria Tauli Corpuz Eduardo Gonzalez Shubert L. Ciencia Magdalena C. Monge Dante O. Bismonte Emilio Paz Roy Layoza Gay D. Defiesta Joseph Gloria This book was made possible with full support of Oxfam Novib. Printed in the Philippines CO N T EN T S Key to Acronyms .............................................................................................................................................................................................................................................................................. iv Foreword.................................................................................................................................................................................................................................................................................................... vii The MDGs and Social Watch -
F866e63db19145e7492573f70
Sitrep No. 3 Tab A EFFECTS OF FLOODING AND LANDSLIDE AFFECTED POPULATION As of February 22, 2008, 8:00 AM AFFECTED POPULATION No. of Evac DISPLACED POPULATION PROVINCE / CITY / REGION Centers Inside Evac Center Outside Evac Center MUNICIPALITY Brgys Families Persons Established Families Persons Families Persons GRAND TOTAL 896 106,455 514,862 7 96 515 60,558 294,882 IV-B 38 7,113 38,192 1 3 12 800 4,800 Oriental Mindoro 38 7,113 38,192 1 3 12 800 4,800 Baco 14 2,243 8,972 Naujan 24 4,870 29,220 1 3 12 800 4,800 V 021,35081,63800000 Albay 9,839 51,162 Catanduanes 150 650 Sorsogon 51 235 Camarines Sur 11,187 28,853 Camarines Norte 123 738 VI 98 3,043 14,757 2 17 45 0 0 Capiz 98 3,043 14,757 2 17 45 Cuartero 8 Dao 12 575 3,420 Dumalag 2 Dumarao 4 120 620 Maayon 15 340 2,040 Mambusao 3 Panay 4 59 353 Panitan 20 100 600 Pontevedra 15 1,059 3,774 1 15 33 Sigma 15 790 3,950 1 2 12 VIII 738 73,302 372,266 1 19 56 58,502 283,802 Eastern Samar 360 33,036 164,716 0 0 0 29,079 144,840 Arteche 13 1,068 5,340 1,068 5,340 Balangiga 13 1,184 5,920 5 17 Balangkayan 10 573 2,267 451 2,183 Borongan 30 1,376 6,582 1,314 6,328 Can-avid 14 1,678 8,411 1,678 8,411 Dolores 27 4,050 20,250 4,050 20,450 Gen. -

Catubig Pcr.Pdf
List of Acronyms AO - Assisting Organization AP - Assisting Professional ASU - Administrative Support Unit CAPWA - Catubig Association for the Protection of Watershed Area CBFM - Community-Based Forest Management CBU - Capital-Build Up CENRO - Community Environment and Natural Resources Office CFDF - Community Forestry Development Fund CIC - CENRO Inspection Committee CO - Community Organizing CSD - Comprehensive Site Development DENR - Department of Environment and Natural Resources DEVELOPERS - Development for Environmental and Rural Sustainability ENRO - Environment and Natural Resources Officer FGD - Focus Group Discussion FSP - Forestry Sector Project GIS - Geographic Information System GPS - Global Positioning System HCAAP - Help Catubig Agricultural Advancement Project HIREDERA - Hinaga River Environmental Development Residents Association HLDMU - Household Land Development Management IEC - Information and Education Campaign LGU - Local Government Unit MASLOG - Maslog Forest Resource Development Association, Inc. MOU - Memorandum of Understanding M & E - Monitoring and Evaluation NGO - Non-Governmental Organization NIA - National Irrigation Authority OJT - On-the-Job Training O/M - Operation and Maintenance PENRO - Provincial Environment and Natural Resources Office PO - People’s Organization SACRED - Samar Center for Rural Education and Development SIBP - Samar Island Biodiversity Foundation SMP - Survey, Mapping and Planning SUSIMO - Subproject Site Management Office SWC - Soil and Water Conservation TPEC-MPDAI - Taft People’s -

Region 8 Households Under 4Ps Sorsogon Biri 950
Philippines: Region 8 Households under 4Ps Sorsogon Biri 950 Lavezares Laoang Palapag Allen 2174 Rosario San Jose 5259 2271 1519 811 1330 San Roque Pambujan Mapanas Victoria Capul 1459 1407 960 1029 Bobon Catarman 909 San Antonio Mondragon Catubig 1946 5978 630 2533 1828 Gamay San Isidro Northern Samar 2112 2308 Lapinig Lope de Vega Las Navas Silvino Lobos 2555 Jipapad 602 San Vicente 844 778 595 992 Arteche 1374 San Policarpo Matuguinao 1135 Calbayog City 853 Oras 11265 2594 Maslog Calbayog Gandara Dolores ! 2804 470 Tagapul-An Santa Margarita San Jose de Buan 2822 729 1934 724 Pagsanghan San Jorge Can-Avid 673 1350 1367 Almagro Tarangnan 788 Santo Nino 2224 1162 Motiong Paranas Taft 1252 2022 Catbalogan City Jiabong 1150 4822 1250 Sulat Maripipi Samar 876 283 San Julian Hinabangan 807 Kawayan San Sebastian 975 822 Culaba 660 659 Zumarraga Almeria Daram 1624 Eastern Samar 486 Biliran 3934 Calbiga Borongan City Naval Caibiran 1639 2790 1821 1056 Villareal Pinabacdao Biliran Cabucgayan Talalora 2454 1433 Calubian 588 951 746 2269 Santa Rita Maydolong 3070 784 Basey Balangkayan Babatngon 3858 617 1923 Leyte Llorente San Miguel Hernani Tabango 3158 Barugo 1411 1542 595 2404 1905 Tacloban City! General Macarthur Capoocan Tunga 7531 Carigara 1056 2476 367 2966 Alangalang Marabut Lawaan Balangiga Villaba 3668 Santa Fe Quinapondan 1508 1271 800 895 2718 Kananga Jaro 997 Salcedo 2987 2548 Palo 1299 Pastrana Giporlos Matag-Ob 2723 1511 902 1180 Leyte Tanauan Mercedes Ormoc City Dagami 2777 326 Palompon 6942 2184 Tolosa 1984 931 Julita Burauen 1091