2014 Annual Report a CONTENTS 2 Message from the Board of Trustees
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

EASTERN VISAYAS: SUMMARY of REHABILITATION ACTIVITIES (As of 24 Mar)
EASTERN VISAYAS: SUMMARY OF REHABILITATION ACTIVITIES (as of 24 Mar) Map_OCHA_Region VIII_01_3W_REHAB_24032014_v1 BIRI PALAPAG LAVEZARES SAN JOSE ALLEN ROSARIO BOBON MONDRAGON LAOANG VICTORIA SAN CATARMAN ROQUE MAPANAS CAPUL SAN CATUBIG ANTONIO PAMBUJAN GAMAY N O R T H E R N S A M A R LAPINIG SAN SAN ISIDRO VICENTE LOPE DE VEGA LAS NAVAS SILVINO LOBOS JIPAPAD ARTECHE SAN POLICARPIO CALBAYOG CITY MATUGUINAO MASLOG ORAS SANTA GANDARA TAGAPUL-AN MARGARITA DOLORES SAN JOSE DE BUAN SAN JORGE CAN-AVID PAGSANGHAN MOTIONG ALMAGRO TARANGNAN SANTO PARANAS NI-O (WRIGHT) TAFT CITY OF JIABONG CATBALOGAN SULAT MARIPIPI W E S T E R N S A M A R B I L I R A N SAN JULIAN KAWAYAN SAN SEBASTIAN ZUMARRAGA HINABANGAN CULABA ALMERIA CALBIGA E A S T E R N S A M A R NAVAL DARAM CITY OF BORONGAN CAIBIRAN PINABACDAO BILIRAN TALALORA VILLAREAL CALUBIAN CABUCGAYAN SANTA RITA BALANGKAYAN MAYDOLONG SAN BABATNGON ISIDRO BASEY BARUGO LLORENTE LEYTE SAN HERNANI TABANGO MIGUEL CAPOOCAN ALANGALANG MARABUT BALANGIGA TACLOBAN GENERAL TUNGA VILLABA CITY MACARTHUR CARIGARA SALCEDO SANTA LAWAAN QUINAPONDAN MATAG-OB KANANGA JARO FE PALO TANAUAN PASTRANA ORMOC CITY GIPORLOS PALOMPON MERCEDES DAGAMI TABONTABON JULITA TOLOSA GUIUAN ISABEL MERIDA BURAUEN DULAG ALBUERA LA PAZ MAYORGA L E Y T E MACARTHUR JAVIER (BUGHO) CITY OF BAYBAY ABUYOG MAHAPLAG INOPACAN SILAGO HINDANG SOGOD Legend HINUNANGAN HILONGOS BONTOC Response activities LIBAGON Administrative limits HINUNDAYAN BATO per Municipality SAINT BERNARD ANAHAWAN Province boundary MATALOM SAN JUAN TOMAS (CABALIAN) OPPUS Municipality boundary MALITBOG S O U T H E R N L E Y T E Ongoing rehabilitation Ongoing MAASIN CITY activites LILOAN MACROHON PADRE BURGOS SAN 1-30 Planned FRANCISCO SAN 30-60 RICARDO LIMASAWA PINTUYAN 60-90 Data sources:OCHA,Clusters 0 325 K650 975 1,300 1,625 90-121 Kilometers EASTERN VISAYAS:SUMMARY OF REHABILITATION ACTIVITIES AS OF 24th Mar 2014 Early Food Sec. -

Understanding Community Preferences for the Use and Management of Samar Island Forest Reserve Based on Participatory Rural Appraisap
UNDERSTANDING COMMUNITY PREFERENCES FOR THE USE AND MANAGEMENT OF SAMAR ISLAND FOREST RESERVE BASED ON PARTICIPATORY RURAL APPRAISAP ..'-- USAIO ******* ...-- UNDERSTANDING COMMUNITY PREFERENCES FOR THE USE AND MANAGEMENT OF SAMAR ISLAND FOREST RESERVE BASED ON PARTICIPATORY RURAL APPRAISAL 1 by LUIS P. ELEAZAR2 Institutional! PRA SpE'cialist July 2000 • Samar Island Biodiversity Study (SAMBIO) Resources, Environment and Economics Center for Studies, Inc. (REECS) In association wiTh Tandaya Foundation Eastern Samar Development Foundation, Inc. (ESADEF) Samar Center for Rural Education and Development, Inc. (SACRED) .. I Thi .. publication was made- possible through support provided by Ihe> lJ. S. AgE"ncy for International DE"velopmpnl fl!5AIDl under the INms of Gr.ant No. 492-G-Oo-OO-00001-00. ThE' opinions expressed hNein are those- of the dulnor dod drJ nol npl.f-':-:-arily fenecllhe views of the U. S. Agency for Internalional DE'v€'iopment. Th~-" .\lIlhor. Mr. luis P. Ele..lzar, is the PRA SpE'cialist of SAMBIO, REECS . ... TABLE OF CONTENTS list of Tables list of Figures Executive Summary...........•...........••.•..•.••..•...•........•..•.•..•.•.•....••••.........•.•.....•.•. vi 1. INTRODUCTION...............................................................•..•............•.. 1 .. 1.1 PRA in the Context of SAMBIO . 1 1.2 The PRA Objectives . 2 1.3 The PRA Teams . 2 ... 2. EXPLANATORY NOTES ON PARTICIPATORY RURAL APPRAiSAL.......•• 3 2.1 Why PRA? . 3 2.2 PRA Research Plan . 3 2.3 PRA Sites and Participants . 4 2.4 Methodology of PRA . 6 3. GENERAL CONTEXT OF SAMAR ISLAND...•..••••..•••••...•••.•....•..•.....•.••.•.•• 8 3.1 Background Information . 8 3.2 Land Use . 9 3.3 Local Economy . 11 3.3.1 Agriculture . 13 3.3.2 Cottage Industry . 14 3.3.3 Tourism . -
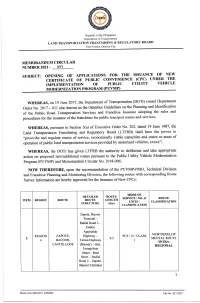
Implementation Ot Public Utility Yehicle Modernization Program (Puymp)
Republic of the PhiliPPines Department of Transportation LAND TRANSPORTATION FRANCIIISING & REGULATORY BOARI) East Avenue, Quezon CitY MEMORANDUM CIRCULAR NUMBER 2A2I. OO'I SUBJECT: OPENING OF APPLICATIONS FOR TIIE ISSUAI\ICE OF I\TEW CERTIFICATE OF PUBLIC CONVENIENCE (CPC) T]}[DER THE IMPLEMENTATION OT PUBLIC UTILITY YEHICLE MODERNIZATION PROGRAM (PUYMP) WHEREAS, on 19 June 2017, the Departuent of Transportation (DOTr) issued Department Identification order No. 2017 - 011 also known as tho Omnibus Guidelines on the Planning and of the public Road Transportation Services and Franchise Issuance adopting the rules and procedures for the issuance of the franchises for public transport routes and services; IyIIEREAS, pursuant to Section 5(a) of Executive Order No. 202, dated 19 June 1987, the Land Transportation Franchising and Regulatory Board (LTFRB) shall have the power to o.prescribe and regulate routes of service, economically viable capaoities and zones or meas of operation of public land transportation services proyided by motorized vehicles, xxxxx"; WIIEREAS, the DOTr has grven LTFRB the authority to deliberate and take appopriate action on proposed nedadditional routes pursuant to the Public Utilify Vehicle Modernization Program (PUVMP) and Memorandum CircularNo. 2018-006; NOW THEREI'ORE, upon the recommendation of the PUVMP-PMO, Technical Division and Franohise Planning and Monitoring Division, the following routes with corresponding Route Survey Information ars hereby approved for the issuance of New CPCs: MODIOT DETAILED ROUTE SERVICEINO. of ROTITE R.EGION ROUTE ROUTE LENGTH ITEM T]NITS / CLASSIFICATION STRUCTURE (k-) CLASSIFICATION Zapote, Bacoor Terminal * Radial Road 2 * Emilio Aguinaldo NEW/DEVELOP REGION ZAPOTE, Highway - PUJ/15/CLASS I 9.2 MENTAL ROUTE 4 BACOOR, Tirona Highway I /NTRA. -

Legend Bernard Tomas Anahawan Matalom Oppus San Juan
Eastern Visayas: Road Conditions as of 7 December 2014 Sorsogon Biri Low-Lying Portions of the Road IMPASSABLE due to Flooding Lavezares Palapag San Jose Laoang Allen Rosario Catbalogan-Catarman via Allen Mondragon San PASSABLE Roque Mapanas Victoria Catarman Capul San Bobon Antonio Catubig Northern Samar Pambujan Gamay San Isidro Lapinig Lope de Vega Silvino Las Navas Lobos Jipapad Arteche Low-Lying Portions of the Road San Policarpo IMPASSABLE due to Flooding Calbayog City Matuguinao Oras Gandara Maslog Tagapul-An San Jose Dolores Catbalogan-LopeDeVega-Catarman Santa de Buan IMPASSABLE due to Margarita Landslide San Jorge Can-Avid Tacloban-Hinabangan-Taft Pagsanghan Jiabong-Tacloban Road Motiong PASSABLE Tarangnan Samar Almagro IMPASSABLESanto due to LandslideNino at Jiabong Masbate Paranas Taft Catbalogan Jiabong Taft-Borongan Road City IMPASSABLE due to Catbalogan-Jiabong Road Sulat Debris & Flooding Maripipi PASSABLE San Julian Hinabangan San Sebastian Kawayan Brgy.Buray-Taft RoadZumarraga Going In & Out of Almeria Culaba IMPASSABLE due to Calbiga Culaba, Biliran Biliran Debris & Flooding Eastern Samar INACCESSIBLE ACCESS ROADS Naval Daram Caibiran Pinabacdao Villareal Borongan City Biliran Calubian Talalora Cabucgayan Santa Rita San Maydolong Isidro Balangkayan Basey Babatngon Leyte San Llorente Tabango Hernani Barugo Miguel Tacloban City General Capoocan Tunga Balangiga Macarthur Carigara Marabut Alangalang Santa Villaba Lawaan Quinapondan Leyte Fe Tacloban to Borongan via Basey Kananga Jaro Salcedo Palo PASSABLE Giporlos All Roads -

EASTERN VISAYAS REGION 0-59 Months Old Prevalence Rate of Malnutrition Overweight and Obese Children Source: OPT 2017
EASTERN VISAYAS REGION 0-59 Months Old Prevalence Rate of Malnutrition Overweight and Obese Children Source: OPT 2017 Ranking per PROVINCES Rank Province Prevalence Rate Magnitude 1 Samar 3.9% 2,741 2 Biliran 3.7% 1,061 3 Northern Samar 3.3% 2,961 4 Leyte 3.3% 5,989 5 Eastern Samar 3.1% 1,988 6 Southern Leyte 2.3% 1,156 Ranking per CITIES Rank City Prevalence Rate Magnitude 1 Baybay City 5.7% 574 2 Ormoc City 5.5% 1,368 3 Calbayog City 5.0% 844 4 Borongan City 4.8% 144 5 Catbalogan City 3.7% 674 6 Tacloban City 3.8% 640 7 Maasin City 1.1% 75 EASTERN VISAYAS REGION 0-59 Months Old Prevalence Rate of Malnutrition Overweight and Obese Children Source: OPT 2017 Ranking per MUNICIPALITIES Rank Municipality Prevalence Rate Magnitude 1 Laoang 22% 290 2 Tolosa 16% 298 3 Gen. Macarthur 15% 200 4 Oras 14% 432 5 San Jorge 14% 204 6 Capoocan 13% 389 7 Basey 12% 403 8 Palompon 11% 537 9 San Policarpo 11% 145 10 Motiong 11% 133 11 Jipapad 10% 71 12 Hinabangan 10% 127 13 Mercedes 10% 82 14 Zumarraga 9% 124 15 Gandara 9% 257 16 Catarman 9% 171 17 Almagro 9% 89 18 Biliran 9% 125 19 Mahaplag 9% 255 20 Carigara 8% 174 21 Palapag 8% 122 22 Giporlos 8% 131 23 Biri 8% 30 24 Matalom 8% 192 25 Can-Avid 8% 138 26 Babatngon 7% 241 27 Capul 7% 66 28 Abuyog 7% 365 29 Sulat 7% 83 30 Tomas Oppus 7% 92 31 Kawayan 7% 88 32 Culaba 7% 38 33 Inopacan 7% 139 34 Kananga 7% 384 35 Isabel 7% 237 36 Malitbog 7% 110 37 Merida 6% 185 38 Daram 6% 277 39 Cabucgayan 6% 121 40 Naval 6% 510 EASTERN VISAYAS REGION 0-59 Months Old Prevalence Rate of Malnutrition Overweight and Obese Children Source: OPT 2017 Ranking per MUNICIPALITIES Rank Municipality Prevalence Rate Magnitude 41 Hilongos 6% 388 42 Maydolong 6% 90 43 Tunga 6% 42 44 Calubian 6% 188 45 Macrohon 6% 137 46 Hernani 6% 49 47 Catubig 6% 80 48 San Julian 6% 70 49 Almeria 6% 106 50 San Francisco 6% 57 51 Sta. -
Untitled Spreadsheet
Facility Name Health Facility Type Street Name and # Building name and # Province Name City/Municipality Name Barangay Name Facility Head: Last Name Facility Head: First Name Facility Head: MiddleFacility Name Head: Position ALMERIA RHU, TB DOTS AND BIRTHING FACILITY Rural Health Unit SITIO BASUD BILIRAN ALMERIA POBLACION GARCIA EVELYN N. Municipal Health Officer BILIRAN MUNICIPAL HEALTH OFFICE Rural Health Unit BILIRAN BILIRAN SAN ROQUE (POB.) BRIONES ELLENOR V Municipal Health Officer CABUCGAYAN MUNICIPAL HEALTH OFFICE Rural Health Unit BILIRAN CABUCGAYAN MAGBANGON (POB.) TAN JULIETA C. Municipal Health Officer CAIBIRAN RURAL HEALTH UNIT Rural Health Unit SANTIAGO STREET BILIRAN CAIBIRAN PALENGKE (POB.) PLAZA DIONESIO B. Municipal Health Officer CULABA MUNICIPAL HEALTH OFFICE LYING-IN AND EMERGENCY CLINIC Rural Health Unit BILIRAN CULABA MARVEL (POB.) PEDROSA ESTRELLA P. Municipal Health Officer KAWAYAN RHU TB DOTS AND BIRTHING FACILITY Rural Health Unit BILIRAN KAWAYAN POBLACION BALASBAS CHRISTINE S Municipal Health Officer MARIPIPI MUNICIPAL HEALTH OFFICE BIRTHING HOME Rural Health Unit BILIRAN MARIPIPI ERMITA (POBLACION SUR) LLEVER MARY GRACE R. Municipal Health Officer NAVAL MUNICIPAL HEALTH OFFICE AND BIRTHING HOME Rural Health Unit BILIRAN NAVAL (Capital) PADRE INOCENTES GARCIA (POB.) MONTEJO FERNANDO B. Municipal Health Officer ARTECHE RURAL HEALTH UNIT Rural Health Unit EASTERN SAMAR ARTECHE CENTRAL (POB.) DULFO BERNIZE Municipal Health Officer BALANGIGA RURAL HEALTH UNIT Rural Health Unit RIZAL STREET EASTERN SAMAR BALANGIGA BARANGAY POBLACION III ENCISO ROSARITA A. Municipal Health Officer BALANGKAYAN RURAL HEALTH UNIT Rural Health Unit ABOGADO STREET EASTERN SAMAR BALANGKAYAN POBLACION II LABRO MA. NELSIE L. Municipal Health Officer BORONGAN CITY HEALTH OFFICE I Rural Health Unit EASTERN SAMAR CITY OF BORONGAN (Capital) SONGCO SACMAR DAISY G. -
Rurban Code Rurban Description 135301 Aborlan
RURBAN CODE RURBAN DESCRIPTION 135301 ABORLAN, PALAWAN 135101 ABRA DE ILOG, OCCIDENTAL MINDORO 010100 ABRA, ILOCOS REGION 030801 ABUCAY, BATAAN 021501 ABULUG, CAGAYAN 083701 ABUYOG, LEYTE 012801 ADAMS, ILOCOS NORTE 135601 AGDANGAN, QUEZON 025701 AGLIPAY, QUIRINO PROVINCE 015501 AGNO, PANGASINAN 131001 AGONCILLO, BATANGAS 013301 AGOO, LA UNION 015502 AGUILAR, PANGASINAN 023124 AGUINALDO, ISABELA 100200 AGUSAN DEL NORTE, NORTHERN MINDANAO 100300 AGUSAN DEL SUR, NORTHERN MINDANAO 135302 AGUTAYA, PALAWAN 063001 AJUY, ILOILO 060400 AKLAN, WESTERN VISAYAS 135602 ALABAT, QUEZON 116301 ALABEL, SOUTH COTABATO 124701 ALAMADA, NORTH COTABATO 133401 ALAMINOS, LAGUNA 015503 ALAMINOS, PANGASINAN 083702 ALANGALANG, LEYTE 050500 ALBAY, BICOL REGION 083703 ALBUERA, LEYTE 071201 ALBURQUERQUE, BOHOL 021502 ALCALA, CAGAYAN 015504 ALCALA, PANGASINAN 072201 ALCANTARA, CEBU 135901 ALCANTARA, ROMBLON 072202 ALCOY, CEBU 072203 ALEGRIA, CEBU 106701 ALEGRIA, SURIGAO DEL NORTE 132101 ALFONSO, CAVITE 034901 ALIAGA, NUEVA ECIJA 071202 ALICIA, BOHOL 023101 ALICIA, ISABELA 097301 ALICIA, ZAMBOANGA DEL SUR 012901 ALILEM, ILOCOS SUR 063002 ALIMODIAN, ILOILO 131002 ALITAGTAG, BATANGAS 021503 ALLACAPAN, CAGAYAN 084801 ALLEN, NORTHERN SAMAR 086001 ALMAGRO, SAMAR (WESTERN SAMAR) 083704 ALMERIA, LEYTE 072204 ALOGUINSAN, CEBU 104201 ALORAN, MISAMIS OCCIDENTAL 060401 ALTAVAS, AKLAN 104301 ALUBIJID, MISAMIS ORIENTAL 132102 AMADEO, CAVITE 025001 AMBAGUIO, NUEVA VIZCAYA 074601 AMLAN, NEGROS ORIENTAL 123801 AMPATUAN, MAGUINDANAO 021504 AMULUNG, CAGAYAN 086401 ANAHAWAN, SOUTHERN LEYTE -

2019 Regional Nutrition Situation
2020 Regional Nutrition Situation 2020 OPERATION TIMBANG PLUS COVERAGE Local Government No. of LGUs No. of LGU with % Submission Units Submission Province 6 6 100% City 7 7 100% Municipality 136 134 98.5% Note: No 2020 OPT+ report from Matag-ob and Villaba, Leyte Total Estimated population Actual number of Percent Coverage Population 0-59 months 0-59 4,742,337 533,039 349, 946 65.7% No. of IP PS measured 4,051 Number of Number of Total Number of Total Number of Province/Independent City Cities/Municipalities with Barangays with OPT Cities/Municipalities Barangays OPT Plus Results Results (1) (2) (3) (4) (5) EASTERN SAMAR 22 22 536 536 SAMAR 24 24 737 731 NORTHERN SAMAR 24 24 569 503 LEYTE 40 37 1,196 1,106 SOUTHERN LEYTE 18 18 430 430 BILIRAN 8 8 132 132 TACLOBAN 0 0 138 129 ORMOC 0 0 110 110 BAYBAY 0 0 92 90 MAASIN 0 0 70 70 CATBALOGAN 0 0 57 57 CALBAYOG 0 0 157 129 BORONGAN 0 0 61 46 STATUS (0-59 months Preschool Children) WEIGHT FOR AGE Magnitude Prevalence Underweight 20,882 6.0% Severely Underweight 5,240 1.5% UW + SUW 26, 122 7.5% HEIGHT FOR AGE Stunted 41,887 12.0% Severely Stunted 16,962 4.8% S+SS 57,980 16.8% WEIGHT FOR LENGTH/HEIGHT Normal 319, 210 91.2% Wasted 10, 136 2.9% Severely Wasted 3, 754 1.1% Overweight 9,625 2.8% Obese 7,137 2.0% W+SW 16,417 4% OW+Ob 15,896 4.8% 2020 REGIONAL NUTRITIONAL STATUS (per age group) 25.0% 20.0% 19.5% 19.2% 18.0% 17.6% 15.0% 11.3% 9.5% 9.2% 10.0% 8.8% 8.2% 6.8% 6.3% 5.3% 4.9% 5.0% 4.9% 4.4% 4.3% 4.3% 5.0% 3.6%3.9% 3.8% 3.3% 3.2% 2.5% 0.0% 0-5 439936-11 4418812-23 24-25 36-47 48-59 UW+SUW St+SSt -

Difficult but Not Impossible PAGE 14 Annual Report 2012 Progress Highlights Contents
Crossing Rivers to Get Pre-Natal Care PAGE ii The First Five Years: Testing the Health Change Model PAGE 4 Leadership Transformation and Health Reforms PAGE 8 End Goal is Sustainability of Good Health Outcomes PAGE 22 Health Challenges in Isolated and Disadvantaged Areas: Difficult But Not Impossible PAGE 14 Annual Report 2012 Progress Highlights Contents 1 Message from the Board of Trustees 4 The First Five Years: P198.1m Testing the Health Change Model ZFF Expenditures 8 Leadership Transformation and Health Reforms 14 Health Challenges in Isolated and Disadvantaged Areas: 95 Difficult but Not Impossible 16 Samar Provinces: Partner-Municipalities 849 Poverty, Governance Health Leaders and Health Trained 22 End Goal is Sustainability of Good Health Outcomes 2.7m 27 Financial Highlights Persons Benefitting from ZFF Programs 2,751 Frontline Health Workers Trained 51 Health Facilities Funded 933,182 Crossing Rivers Residents Benifitting from 51 ZFF-sponsored to Get Pre-Natal Care Health Facilities in 30 Municipalities For some, getting healthcare requires literally going the extra mile – taking hours of boat rides, long walks, lengthy land travels or a combination of these. Such is the case of these three pregnant women who are boarding a boat with the help of midwife Elmer Estudillo. They need to cross the river that separates their village from the poblacion where the Rural Health Unit is located. The short one-way ride costs P5 a person. They can also use a hanging bridge but that is a longer and riskier alternative, especially for these expectant mothers. Daram, Samar Location: Barangay Calingnan, Catubig in Northern Samar B ZUELLIG FAMILY FOUNDATION A Message from the Zuellig Family Committed to Rural Health government units in programs to build disadvantaged areas, and continuous specific capacities in health leadership efforts will be required to ensure and health governance. -

The Study on the Provincial Water Supply, Sewerage and Sanitation Sector Plan in the Republic of the Philippines
No. JAPAN INTERNATIONAL COOPERATION AGENCY THE STUDY ON THE PROVINCIAL WATER SUPPLY, SEWERAGE AND SANITATION SECTOR PLAN IN THE REPUBLIC OF THE PHILIPPINES SUMMARY REPORT PROVINCIAL WATER SUPPLY, SEWERAGE AND SANITATION SECTOR PLAN FOR THE PROVINCES OF AGUSAN DEL NORTE MISAMIS ORIENTAL AGUSAN DEL SUR BUKIDNON DAVAO DEL SUR DAVAO DEL NORTE DAVAO ORIENTAL SOUTH COTABATO SURIGAO DEL NORTE SARANGANI NORTHERN SAMAR AKLAN EASTERN SAMAR ANTIQUE SAMAR CAPIZ BILIRAN ILOILO LEYTE NEGROS OCCIDENTAL SOUTHERN LEYTE AUGUST 2000 NJS CONSULTANTS CO., LTD. SSS J R 00-112 EXCHANGE RATE (As of 31 July 2000) US$ 1.00 = Peso 42.23 = Yen 110.65 JAPAN INTERNATIONAL COOPERATION AGENCY DEPARTMENT OF THE INTERIOR AND LOCAL GOVERNMENT THE REPUBLIC OF THE PHILIPPINES THE STUDY ON THE PROVINCIAL WATER SUPPLY, SEWERAGE AND SANITATION SECTOR PLAN IN THE REPUBLIC OF THE PHILIPPINES SUMMARY REPORT PROVINCIAL WATER SUPPLY, SEWERAGE AND SANITATION SECTOR PLAN FOR THE PROVINCES OF AGUSAN DEL NORTE MISAMIS ORIENTAL AGUSAN DEL SUR BUKIDNON DAVAO DEL SUR DAVAO DEL NORTE DAVAO ORIENTAL SOUTH COTABATO SURIGAO DEL NORTE SARANGANI NORTHERN SAMAR AKLAN EASTERN SAMAR ANTIQUE SAMAR CAPIZ BILIRAN ILOILO LEYTE NEGROS OCCIDENTAL SOUTHERN LEYTE AUGUST 2000 NJS CONSULTNTS CO., LTD. PREFACE In response to a request from the Government of the Republic of the Philippines, the Government of Japan decided to conduct the Study on Provincial Water Supply, Sewerage and Sanitation Sector Plans for Visayas and Mindanao and entrusted the study to the Japan International Cooperation Agency (JICA). JICA slected and dispatched the study team headed by Mr. Masatoshi Momose of NJS Consultants Co., Ltd. to the Philippines, 4 times between January 1998 and May 2000. -

Region VIII OPERATION TIMBANG RESULTS 2012
Region VIII OPERATION TIMBANG RESULTS 2012 Free Powerpoint Templates Page 1 ComparativeOPT COVERAGE OPT 2011-2012% PREVALENCE Results (based on 2000 proj. pop) PROVINCES 2011 2012 2011 2012 BILIRAN 75.69 77.93 13.11 12.38 E. SAMAR 75.94 11.83 10.82 79.60 LEYTE 69.25 15.73 15.12 70.50 N. SAMAR 80.43 17.69 15.80 76.30 SAMAR 62.76 21.54 17.88 69.30 So. LEYTE 69.21 7.95 7.82 73.40 Free Powerpoint Templates Page 2 OPT COVERAGE % PREVALENCE (based on 2000 proj. pop) CITIES 2011 2012 2011 2012 BAYBAY 63.73 62.27 13.97 13.56 BORONGAN 61.95 63.48 14.05 11.47 60.81 CALBAYOG 80.78 11.76 12.31 CATBALOGAN 73.57 67.57 27.75 18.31 MAASIN 74.84 5.03 4.69 62.90 93.70 12.57 11.99 ORMOC 93.77 TACLOBAN 71.38 9.88 8.51 66.92 14.98 13.68 REGION VIII 73.15 Free71.71 Powerpoint Templates Page 3 Southern Eastern Visayas: 25.7 Leyte: Free Powerpoint Templates 21.6 Page 4 Southern Leyte: 37.1 Free Powerpoint Templates Eastern Visayas: Page 5 41.7 Phil. Ave. 7.3 Eastern Visayas: Free Powerpoint Templates 7.8 Page 6 Comparative OPT 2011-2012 Results Province/ City 2011 Prev (%) 2012 Prev (%) % Change Biliran 13.11 12.38 0.73 Eastern Samar 11.83 10.82 1.01 Leyte 15.73 15.12 0.61 Northern Samar 17.69 15.80 1.89 Samar 21.54 17.88 3.66 Southern Leyte 7.95 7.82 0.13 Baybay City 13.97 13.56 0.41 Borongan City 14.05 11.47 2.58 Calbayog City 11.76 12.31 -0.55 Catbalogan City 27.75 18.31 9.44 Maasin City 5.03 4.69 0.34 Ormoc City 12.57 11.99 0.58 Tacloban City 9.88 8.51 1.37 Region VIII 14.98Free Powerpoint13.68 Templates 1.30 Page 7 Prevalence of Underweight According to -
Contribution to the Mosses of the Philippines
PR E S L I A 1959 31: 247-250 Zdenek P i 1 o u s: Contribution to the Mosses of the Philippines By the kindness of members of Philippine Nationa] Herbarium of Manila a collection of Philippine mosses was sent to me for determination. In this contribution I am giving first part of the mosses determinated. Acanthorrchynchium papillosum (Har v.) F 1 e is c h. P a lawan , Victor·ia Mountains, a long forest edge, ea. 800 m ., leg. G. E. Edano, J 4258 bis. Ac'f"oporium alto-pungens (C. M.) Broth. Negros Occidental: Canlaon Val, a long lake, ea. 1860 m., leg. G. E. Edaiio, 20145, 20147. Acroporium hamatum F l eis c h. Palawan: Victoria Mountains, summit, ea. 760 m., leg. G. E. Edaiio, 14264. Acroporium secundum (H, e in w.) F 1 e i s c h. Palawan: Brooke's Point, Mt. Mantalingahan, Routh slopes ban summit, ea. 5660 ft., leg. G. E. Edano, 590. Negros Occ>.identa l : Mt. Canlaon, summit, ea. 1960 m., leg. G. E. Edafto , 20157. Acroporium rufum (Rein w. et Horns c h.) F l eis c h. Palawan: Victoria Mountains, summit, ea. 760 m., leg. G. E. Edaf10, 14263. Aerobryopsis longissima (D o z. et Mo l k.) F l e i s c h. Rarnar: Mt. Capot.o}tn along forest edge, ea. 200 m., leg. G. E. Edano, 15921, 15922. Samar: Matuguinao, leg. F'. Ga()halia n, 15903 bis. Arthrocormus Schimperi Do z. et Mo I k. Samar: Mount, Purog, Along forested ridge, ea. 110 m., leg.