Noreen Akhtar M.Sc
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Public Notice Auction of Gold Ornament & Valuables
PUBLIC NOTICE AUCTION OF GOLD ORNAMENT & VALUABLES Finance facilities were extended by JS Bank Limited to its customers mentioned below against the security of deposit and pledge of Gold ornaments/valuables. The customers have neglected and failed to repay the finances extended to them by JS Bank Limited along with the mark-up thereon. The current outstanding liability of such customers is mentioned below. Notice is hereby given to the under mentioned customers that if payment of the entire outstanding amount of finance along with mark-up is not made by them to JS Bank Limited within 15 days of the publication of this notice, JS Bank Limited shall auction the Gold ornaments/valuables after issuing public notice regarding the date and time of the public auction and the proceeds realized from such auction shall be applied towards the outstanding amount due and payable by the customers to JS Bank Limited. No further public notice shall be issued to call upon the customers to make payment of the outstanding amounts due and payable to JS Bank as mentioned hereunder: Customer ID Customer Name Address Amount as of 8th April 1038553 ZAHID HUSSAIN MUHALLA MASANDPURSHI KARPUR SHIKARPUR 343283.35 1012051 ZEESHAN ALI HYDERI MUHALLA SHIKA RPUR SHIKARPUR PK SHIKARPUR 409988.71 1008854 NANIK RAM VILLAGE JARWAR PSOT OFFICE JARWAR GHOTKI 65110 PAK SITAN GHOTKI 608446.89 999474 DARYA KHAN THENDA PO HABIB KOT TALUKA LAKHI DISTRICT SHIKARPU R 781000 SHIKARPUR PAKISTAN SHIKARPUR 361156.69 352105 ABDUL JABBAR FAZALEELAHI ESTATE S HOP NO C12 BLOCK 3 SAADI TOWN -

Flood Emergency Reconstruction and Resilience Project, Loan No. 3264
Due Diligence Report on Social Safeguards Loan 3264-PAK: Flood Emergency Reconstruction and Resilience Project (FERRP)–Punjab Roads Component Due Diligence Report on Social Safeguards on Reconstruction of Daska – Pasrur Road March 2017 Prepared by: Communication and Works Department, Government of the Punjab NOTES (i) The fiscal year (FY) of the Government of the Islamic Republic of Pakistan and its agencies ends on 30 June. (ii) In this report, "$" refers to US dollars. This Social Safeguards due diligence report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. GOVERNMENT OF THE PUNJAB COMMUNICATION & WORKS DEPARTMENT Flood Emergency Reconstruction and Resilience Project (FERRP) Social Due Diligence Report of Reconstruction of Daska- Pasrur Road (RD 0+000 – RD 30+000) March, 2017 Prepared by TA Resettlement Specialist for Communication and Works Department, Government of Punjab, Lahore Table of Contents CHAPTER 1 INTRODUCTION ................................................................................................................... 1 A. Background: ............................................................................................................. -

Batch-15 Candidates Waiting for Exam
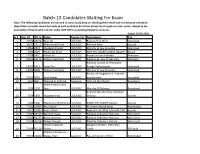
Batch-15 Candidates Waiting For Exam Note: The following Candidates are advised to consciously keep on checking their email and sms because intimation about Exam schedule would be made to each candidate by Virtual University through sms and email, subject to the availability of Examination Center under GOP SOP in prevailing Pandemic scenario. Hence, no need to contact VU or NITB in this regard. Dated:22/01/2021 S.No Name Course_ForDepartment NIC City Status AMF PAC BOARD KAMRA 1 MAJID ALI KHAN LDC/UDC (MoDP) 14202-1347682-3 Attock W_Batch15 Pakistan Bureau of Statistics, 2 Muhammad hanif LDC/UDC Peshawar 17301-1453072-5 Peshawar W_Batch15 Bureau of emigration & 3 Saad Nawaz LDC/UDC overseas employment 37402-8078184-5 islamabad W_Batch15 4 Muneeb ur Rehman Assistant GHQ, PS Directorate 37405-4070406-7 Rawalpindi W_Batch15 Airports Security Force 5 Muzaffar Khan LDC/UDC /Aviation Division 42201-1995929-9 Karachi W_Batch15 FF Centre Record Wing 6 Nasir Bashir LDC/UDC Abbottabad 35404-1441380-9 Abbottabad W_Batch15 Regional Tax Office-I,Karachi, 7 Yusra Sohail LDC/UDC FBR 42101-7219540-0 Karachi. W_Batch15 8 Zahid Ali Awan Assistant Pakistan Ordnance Factories 38403-6415504-7 Wah Cantt W_Batch15 9 Aamir Waheed LDC/UDC Pakistan Ordnance Factories 37406-1617666-1 Wah Cantt W_Batch15 10 Nabeel Ahmad LDC/UDC Pakistan Ordnance Factory 37406-0478098-7 Wah Cantt W_Batch15 Weapons Factory, POFs Wah 11 Muhammad Zain ShahidLDC/UDC Cantt. 37406-2805701-5 POF Wah W_Batch15 12 Muhammad Hassan WaqasAssistant Khan Pay and Account Office 38301-2125015-7 Abbottabad W_Batch15 Batch-15 Candidates Waiting For Exam Note: The following Candidates are advised to consciously keep on checking their email and sms because intimation about Exam schedule would be made to each candidate by Virtual University through sms and email, subject to the availability of Examination Center under GOP SOP in prevailing Pandemic scenario. -
Part-I: Post Code Directory of Delivery Post Offices
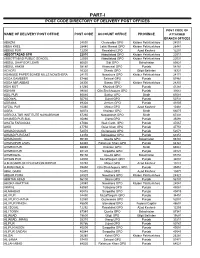
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Male / Co-Education) and Male Head of Institution at Ssc Level Upto 14-07-2021
1 LIST OF AFFILIATED INSTITUTIONS WITH STATUS (MALE / CO-EDUCATION) AND MALE HEAD OF INSTITUTION AT SSC LEVEL UPTO 14-07-2021 Inst Inst Principal S.No Inst Adress Gender Principal Name Phone No Principal Mobile No level Code Gender Angelique School, St.No.81, Embassy 051-2831007-8, 1. SSC 1002 Co-Education Maj (R) Nomaan Khan MALE 0321-5007177 Road, G-6/4, Islamabad 0321-5007177 Sultana Foundation Boys High School, 2. SSC 1042 Farash Town, Lehtrar Road (F.A), MALE WASEEM IRSHAD MALE 051-2618201 (Ext 152) 0315-7299977 Islamabad Scientific Model School, 25-26, Humak 051-4491188 , 3. SSC 1051 Co-Education KHAWAJA BASHIR AHMAD MALE 0345-5366348 (F.A), Islamabad 0345-5366348 Fauji Foundation Model School, Chak Wing Cdre Muhammad Laeeq 051-2321214, 4. SSC 1067 Co-Education MALE 0320-5635441 Shahzad Campus (F.A), Islamabad. Akhtar 0321-4044282 Academy of Secondary Education, Nai 051-4611613, 5. SSC 1070 Abadi G.T Road, Rewat (F.A), Co-Education Mr. AZHAR ALI SHAH MALE 0314-5136657 0314-5136657 Islamabad National Public Secondary School, G. 051-4612166, 6. SSC 1077 Co-Education IRFAN MAHMOOD MALE 03005338499 T Road, Rewat (F.A), Islamabad 0300-5338499 National Special Education Centre for 9260858, 7. SSC 1080 Physically Handicapped Children, G- Co-Education Islam Raziq MALE 0333-0732141 9263253 8/4, Islamabad Oxford High School, 413, Street No 43, 8. SSC 1083 Co-Education Lt. Col. Zafar Iqbal Malik (Retd) MALE 051-2253646 0321-5010789 Sector G-9/1, Islamabad Rawat Residential College, college 9. SSC 1090 Co-Education Tanzeela Malik Awan MALE 051-2516381 03465296351 Road, Rawat (F.A), Islamabad Sir Syed Ideal School System, House 10. -

Population Census of Pakistan 1961
( ·~ " POPULATION CENSUS OF PAKISTAN 1961 ~ DISTRICT CENSUS REPORT -RAWALPINDI PART-V rV lllAGE STATISJ.ics· 'COMPIL~D BY i<i-iA ·~ BASHIR AHMED KAAN 'ASSJSTANT DIRECTOR OF cENSUS Ri\WALPINoi ~ lt ~':"",.a;ll!;. mn=-rr:n INTRODUCTION The village is the ba sic unit of revenue The Village Statistics contained in this administration and the need for basic statis part have been compiled from Block-wise tics for villages is quite obvious as au plan fi gures contained in the Summaries prepared ning depends on such statistics. They are a lso by the Census Supervisors and Charge indispensable fo r carrying out sample surveys Superintendents. Except for data on houses over limited areas and form the basis of contin and houseJ10lds they are based on the results uous collection ofs tatistics on different aspects of the "Circle Sort"' which was carried out in of rural life and economy. The village was ta ken the Hand Sorting Centres after the physical as the basic unit of enumeration if its popula counting of the individual enumeration tion was 600 or it was a continuous collection schedules. The literacy figures, however, have of about 150 houses on an average. Where been lifted from the Summaries prepared by the village approximated to this size, it was the Supervisors and Charge Superintendents. constituted into a Block. A large nu mber of villages ha d to be split up into a number of The plan of presentati on is that for each Blocks, but the boundaries of Census Block village, the Hadbast number, its name in did not go beyond the limits of a revenue English and Urdu a nd a rea in acres, the estate. -

BIT Exam Schedule of Batch15 and Batch-14.5 Dated:28-03-2021 Sr # Name Department Testid Course Center Testdate Examtime VRWP01 - D-102, M.A
BIT Exam Schedule of Batch15 and Batch-14.5 Dated:28-03-2021 Sr # Name Department TestID Course Center TestDate ExamTime VRWP01 - D-102, M.A. Road Satellite Town, 1 Muhammad Junaid Rawalpindi. 051 – 4853215, 4853216, Ilyas Ministry Of Defence VU201500873 CPL1-3 4853217 Apr 03, 2021 02:30 PM VRWP01 - D-102, M.A. Road Satellite Town, 2 Rawalpindi. 051 – 4853215, 4853216, Muhammad Zubair Ministry of Defence VU201400821 CPL1-3 4853217 Apr 04, 2021 02:30 PM VKHI01 - Shahrah-e-Faisal Campus Ground and Mezzanine Floors, Park Avenue 3 Building, Opp: Jason Trade Center (Laal AVIATION DIVISION, AIRPORTS Kothi), Shahrah-e-Faisal. Block-6. PECHS. MOULA BUX SECURITY FORCE VU170911050 CPL1-3 Karachi. 021-34313660-1-2 Apr 04, 2021 08:30 AM VKHI02 - D3. First Floor. Block-D Above 4 Ufone Customer Service & Burj Bank North Mahmood UR Nazimabad, Karachi. 021-36631986, Rehman PNMIT DTE KS&EW Karachi VU201501603 CPL1-3 36632001, 36631982 Apr 03, 2021 11:10 AM VRWP01 - D-102, M.A. Road Satellite Town, 5 Ministry of Ports & Shipping, Rawalpindi. 051 – 4853215, 4853216, Muhammad Rashid Gwadar Section VU171011152 CPL1-6 4853217 Apr 06, 2021 11:10 AM VPSW01 - Opposite BISE Peshawar & 6 Adjacent to ICMS College, Board Bazar, Tauqeer Ali Shah Ministry of Defense Production VU170400144 CPL1-6 Peshawar 091-5701071, 091- 9239303 Apr 04, 2021 02:30 PM VRWP01 - D-102, M.A. Road Satellite Town, 7 Munir Ahmed Rawalpindi. 051 – 4853215, 4853216, Abbasi National Accountability Bureau VU170910729 CPL1-3 4853217 Apr 04, 2021 08:30 AM BIT Exam Schedule of Batch15 and Batch-14.5 Dated:28-03-2021 Sr # Name Department TestID Course Center TestDate ExamTime VRWP01 - D-102, M.A. -

List of Ssc Institutions Affiliated with Fbise Within Pakistan Upto Dated 16-10-2020
LIST OF SSC INSTITUTIONS AFFILIATED WITH FBISE WITHIN PAKISTAN UPTO DATED 16-10-2020 LIST OF SSC INSTITUTIONS AFFILIATED WITH FBISE WITHIN PAKISTAN UPTO DATED 16-10-2020 Institution Inst Principal S.No Inst level Inst Address Principal Name Principal Phone No Principal Mobile No Code Gender Gender Angelique School, St.No.81, Embassy Road, Co-Education 1. SSC 1002 Maj (R) Nomaan Khan MALE 051-2831007 0321-5007177 G-6/4, Islamabad Sultana Foundation Boys High School, 2. SSC 1042 Farash Town, Lehtrar Road (F.A), MALE CH.MUHAMMAD ILYAS MALE 051-2329149 0333-5155434 Islamabad Scientific Model School, 25 -26, Humak Co-Education 3. SSC 1051 KHAWAJA BASHIR AHMAD MALE 051-4491188 0345-5366348 (F.A), Islamabad Fauji Foundation Model School, Chak Co-Education 4. SSC 1067 LT COL KHALID FAIZ(R) MALE 051-2321214 0321-4044282 Shahzad Campus (F.A), Islamabad. Academy of Secondary Education, Nai Co-Education 5. SSC 1070 Mr. AZHAR ALI SHAH MALE 051-4611613 0314-5136657 Abadi G.T Road, Rewat (F.A), Islamabad National Public Secondary School, G. T Co-Education 6. SSC 1077 IRFAN MAHMOOD MALE 0514612166 03005338499 Road, Rewat (F.A), Islamabad National Special Education Centre for 7. SSC 1080 Physically Handicapped Children, G-8/4, Co-Education Dr. Irfan Ahmed MALE 051-9260858 Islamabad Oxford High School, 413, Street No 43, Co-Education 8. SSC 1083 Col(R) Zafar Iqbal Malik MALE 051-2253646 923215010789 Sector G-9/1, Islamabad Rawat Residential College, college Road, Co-Education 9. SSC 1090 Tanzeela Malik Awan MALE 03025020927 03465296351 Rawat (F.A), Islamabad National Special Education Centre For 10. -

Tender Notice January, 2018
OFFICE OF THE DISTRICT COUNCIL, RAWALPINDI TENDER NOTICE Sealed percentage/item rate tenders are hereby invited for the following schemes/works from the approved enslited contractors who have got their names enlisted/renewed for the current Financial year 2017-2018 from any of MC/Municipal Corporation/District Council of Rawalpindi Division on following terms and conditions:- 1. In case of Limited Company the partnership deed will have to be presented before officials. 2. Registration receipt/letter of current year 2017-2018 must be submitted. 3. If the case the tender rates are below than 5%, the Performance Security will be received according to policy of the Government of the Punjab i.e 10% on contract amount in shape of CDR from schedule bank in the name of District Council, Rawalpindi. 4. From date of publication, the applications for issuance of tenders form will be received upto 29-12-2017 during office timmings alongwith tender fees amounting to Rs. 1000/- per tender form in the office of Head Clerk (I&S) branch, District Council, Rawalpindi. 05% Earnest Money in shape of Call Deposit (CDR) from the scheduled banks in name of District Council, Rawalpindi will also be received upto 29-12-2017. 5. Tender forms will be issued on 01-01-2018 upto 12:00PM. 6. 5% (Five percent) earnest money in shape of Call Deposit (CDR) from the scheduled banks in name of District Council, Rawalpindi should be accompanied with each tender form. 7. Tender forms will be received upto 01:00 PM on 01-01-2018 and will be opened at 02:00 PM in the presence of Tender Openning Committee and Contractors or their representatives in the office of District Council, Rawalpindi. -
Batch-15 Candidates Waiting for Exam
Batch-15 Candidates Waiting For Exam Note: The following Candidates are advised to consciously keep on checking their email and sms because intimation about Exam schedule would be made to each candidate by Virtual University through sms and email, subject to the availability of Examination Center under GOP SOP in prevailing Pandemic scenario. Dated: 10-03-2021 Sr # App_ID Off_Sr Name Course_For Department City 1 75542 23163 Noor Ali LDC/UDC Regional Tax Office Islamabad 2 39077 22111 Muhammad Tariq LDC/UDC Pakistan Navy Karachi 3 12855 2822 Muqbool Ahmed LDC/UDC Ministry of Law & Justice Islamabad 4 4995 1025 MAJID ALI KHAN LDC/UDC AMF PAC BOARD KAMRA (MoDP) Attock 5 19298 5431 Adnan Ali LDC/UDC Postal Services Pakistan Peshawar 6 29039 10173 Muhammad hanif LDC/UDC Pakistan Bureau of Statistics, Peshawar Pakistan Council of Renewable 7 18155 5413 Sadar Din LDC/UDC Energy Technologies Islamabad 8 13701 4000 Muhammad Islam LDC/UDC Ministry of Law & Justice, Islamabad Bureau of emigration & overseas 9 25935 8315 Saad Nawaz LDC/UDC employment islamabad 10 4537 992 Muneeb ur Rehman Assistant GHQ, PS Directorate Rawalpindi Muhammad Junaid 11 2296 1174 Ilyas LDC/UDC Ministry Of Defence Rawalpindi Airports Security Force /Aviation 12 5876 1403 Muzaffar Khan LDC/UDC Division Karachi 13 2933 1000 Mahmood UR Rehman LDC/UDC PNMIT DTE KS&EW Karachi Karachi 14 74369 22085 Nasir Bashir LDC/UDC FF Centre Record Wing Abbottabad 15 70352 22086 Yusra Sohail LDC/UDC Regional Tax Office-I,Karachi, FBR Karachi. 16 71005 20526 Zahid Ali Awan Assistant Pakistan Ordnance Factories Wah Cantt 17 71010 20527 Aamir Waheed LDC/UDC Pakistan Ordnance Factories Wah Cantt 18 71014 20528 Nabeel Ahmad LDC/UDC Pakistan Ordnance Factory Wah Cantt Muhammad Zain Weapons Factory, POFs Wah 19 71306 20529 Shahid LDC/UDC Cantt. -
Rawalpindi Blockwise
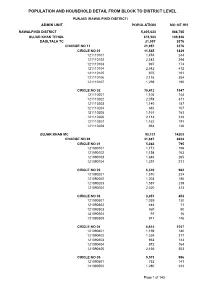
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL PUNJAB (RAWALPINDI DISTRICT) ADMIN UNIT POPULATION NO OF HH RAWALPINDI DISTRICT 5,405,633 888,765 GUJAR KHAN TEHSIL 678,503 109,826 DAULTALA TC 21,957 3376 CHARGE NO 11 21,957 3376 CIRCLE NO 01 11,545 1829 121110101 1,474 244 121110102 2,143 294 121110103 997 174 121110104 2,542 412 121110105 975 161 121110106 2,116 354 121110107 1,298 190 CIRCLE NO 02 10,412 1547 121110201 1,105 144 121110202 2,078 311 121110203 1,140 187 121110204 682 107 121110205 1,167 163 121110206 2,114 318 121110207 1,162 191 121110208 964 126 GUJAR KHAN MC 90,131 14203 CHARGE NO 09 41,687 6634 CIRCLE NO 01 5,363 795 121090101 1,172 156 121090102 1,154 163 121090103 1,646 265 121090104 1,391 211 CIRCLE NO 02 6,320 962 121090201 1,510 224 121090202 1,203 186 121090203 1,587 239 121090204 2,020 313 CIRCLE NO 03 3,051 453 121090301 1,039 130 121090302 444 71 121090303 560 90 121090304 97 16 121090305 911 146 CIRCLE NO 04 6,614 1057 121090401 1,198 180 121090402 1,324 217 121090403 963 143 121090404 973 164 121090405 2,156 353 CIRCLE NO 05 5,573 996 121090501 752 141 121090502 1,280 233 Page 1 of 143 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL PUNJAB (RAWALPINDI DISTRICT) ADMIN UNIT POPULATION NO OF HH 121090503 1,083 196 121090504 1,313 233 121090505 1,145 193 CIRCLE NO 06 5,306 839 121090601 774 117 121090602 1,193 193 121090603 832 143 121090604 1,634 244 121090605 873 142 CIRCLE NO 07 5,736 921 121090701 1,128 178 121090702 547 104 121090703 1,670 261 121090704 2,391 378 CIRCLE NO 08 -

Dassu Chilas Swat Disputed Area Bala Kot Athmuqam Allai Palas
73°0’0"E 73°30’0"E 74°0’0"E Karang Gilgit Darel/Tangir Thuti Sazin Karin Goshali 35°30’0"N 35°30’0"N Baryar Parwa Swat Siglo Dassu Seo Bar Jalkot Chilas Goshali Koz Jalkot Dassu Chawa Dara Dubair Bala Kamila Kayal Sagayon Pattan Jijal CRS, Army Dubair Khas SPO Kunshair CRS Dubair Pain Patan SPO, Army SPO, Army Peach Bela Shalkan Abod Bar Paro Pir Kana Ronolia SPO, Army Haran SPO Shareed Sheryal CRS, SPO Khota Kot Kuz Paro Kuz Kalle Albat SPO, Army Bazar SPO Sherakot SPO, Army SPO SPO CRS, SPO, Army Kolai Bankhad SPO, Army 35°0’0"N Lilunai SPO Palas Mada Khail 35°0’0"N SPO, Army Bar Kana SPO, Army Batera Pain Alpuri CRS, BEST SPO, Army Shahpur Sakargarh CARE, SCF, Sungi SPO, Army Kaghan Alpuri Kuz Kana Batyal WVI Damorai SPO, Army SPO, CWS Jambera Pir Abad SCF, BEST Pashto Kel SPO, Army PPAF, SCF, BEST Bisham Bateela Dherai Allai ACTED, Sungi, CARE SPO, Army Bana Bala Kot Dandai SCF, CWS, Sungi, BEST Malik Khel Chakisar Army ACTED, PPAF, SCF, Sungi, CARE Biari Shardi SPO, Army Rashang IR Puran Batkul SPO, Army Chakisar PPAF, CARE, CRS, ACTED Musa Khail Guresinakka Paimal Sharif PPAF, SDC, Sungi, FRC Athmuqam Alouch Thakot Sungi, BEST Batamori Puran SPO, Army SPO, CWS, Sungi Bunerwal Devli Jaberr Dudhnial Batagram SDC, SPO, Sungi, BEST PPAF, CRS, KP, BEST Shamlai Kewal IR Batagram SFL,PPAF, ACTED, CWS, Sungi, ILAP Peshora Nilam SPO, Army Bassi Khel PPAF, SPO, Sungi IOM, SPO, CWS, Sungi, SCF AC, Army IR Martoong Rajdhari Mohandri Gijbori Ajmera SPO, Sungi, BEST PPAF, KP,MC, CRS, BEST, ILAP HFH, SDC, CWS, Sungi Behlool Khail SPO, Sungi, BEST