The Best Start for Life
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

House of Commons Official Report Parliamentary Debates
Monday Volume 652 7 January 2019 No. 228 HOUSE OF COMMONS OFFICIAL REPORT PARLIAMENTARY DEBATES (HANSARD) Monday 7 January 2019 © Parliamentary Copyright House of Commons 2019 This publication may be reproduced under the terms of the Open Parliament licence, which is published at www.parliament.uk/site-information/copyright/. HER MAJESTY’S GOVERNMENT MEMBERS OF THE CABINET (FORMED BY THE RT HON. THERESA MAY, MP, JUNE 2017) PRIME MINISTER,FIRST LORD OF THE TREASURY AND MINISTER FOR THE CIVIL SERVICE—The Rt Hon. Theresa May, MP CHANCELLOR OF THE DUCHY OF LANCASTER AND MINISTER FOR THE CABINET OFFICE—The Rt Hon. David Lidington, MP CHANCELLOR OF THE EXCHEQUER—The Rt Hon. Philip Hammond, MP SECRETARY OF STATE FOR THE HOME DEPARTMENT—The Rt Hon. Sajid Javid, MP SECRETARY OF STATE FOR FOREIGN AND COMMONWEALTH AFFAIRS—The Rt. Hon Jeremy Hunt, MP SECRETARY OF STATE FOR EXITING THE EUROPEAN UNION—The Rt Hon. Stephen Barclay, MP SECRETARY OF STATE FOR DEFENCE—The Rt Hon. Gavin Williamson, MP LORD CHANCELLOR AND SECRETARY OF STATE FOR JUSTICE—The Rt Hon. David Gauke, MP SECRETARY OF STATE FOR HEALTH AND SOCIAL CARE—The Rt Hon. Matt Hancock, MP SECRETARY OF STATE FOR BUSINESS,ENERGY AND INDUSTRIAL STRATEGY—The Rt Hon. Greg Clark, MP SECRETARY OF STATE FOR INTERNATIONAL TRADE AND PRESIDENT OF THE BOARD OF TRADE—The Rt Hon. Liam Fox, MP SECRETARY OF STATE FOR WORK AND PENSIONS—The Rt Hon. Amber Rudd, MP SECRETARY OF STATE FOR EDUCATION—The Rt Hon. Damian Hinds, MP SECRETARY OF STATE FOR ENVIRONMENT,FOOD AND RURAL AFFAIRS—The Rt Hon. -

Announcement
Announcement Total 100 articles, created at 2016-07-09 18:01 1 Wimbledon: Serena Williams eyes revenge against Angelique Kerber in today's final (1.14/2) Serena Williams has history in her sights as the defending champion plots to avenge one of the most painful defeats of her career by beating Angelique Kerber in today’s Wimbledon final 2016-07-09 14:37 1KB www.mid-day.com 2 Phoenix police use tear gas on Black Lives Matter rally (PHOTOS, VIDEOS) — RT America (1.03/2) Police have used pepper spray during a civil rights rally in Phoenix, Arizona, late on Friday night. The use of impact munitions didn’t lead to any injuries, and no arrests have been made, Phoenix Police Chief said. 2016-07-09 18:00 1KB www.rt.com 3 Castile would be alive today if he were white: Minnesota Governor (1.02/2) A county prosecutor investigating the police shooting of a black motorist in Minnesota on Friday said law enforcement authorities in his state and nationwide must improve practices and procedures to prevent future such tragedies, regardless of the outcome of his probe. 2016-07-09 18:00 3KB www.timeslive.co.za 4 Thousands take to streets across US to protest police violence (1.02/2) Thousands of people took to the streets in US cities on Friday to denounce the fatal police shootings of two black men this week, marching the day after a gunman killed five police officers watching over a similar demonstration in Dallas. 2016-07-09 18:00 3KB www.timeslive.co.za 5 Iran says it will continue its ballistic missile program (1.02/2) TEHRAN, Iran—Iran says it will continue its ballistic missile program after claims made by the UN Secretary-General Ban Ki-Moon that its missile tests aren't in the spirit of the 2016-07-09 17:37 1KB newsinfo.inquirer.net 6 Hillary Clinton reacts to Dallas shootings In an interview with Scott Pelley that aired first on CBSN, Hillary (1.02/2) Clinton shared her thoughts on Thursday's shooting in Dallas. -
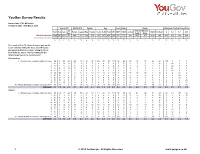
Survey Report
YouGov Survey Results Sample Size: 1703 GB Adults Fieldwork: 25th - 26th March 2019 Vote in 2017 EU Ref 2016 Gender Age Social Grade Region Likelihood of voting Conservative Lib Rest of Midlands / Total Con Lab Remain Leave Male Female 18-24 25-49 50-64 65+ ABC1 C2DE London North Scotland 0 1-4 5-7 8-10 Dem South Wales Weighted Sample 1703 562 526 95 656 702 824 879 187 717 405 393 971 732 204 569 368 416 146 640 303 342 419 Unweighted Sample 1703 619 526 110 737 720 766 937 148 684 447 424 1012 691 174 615 373 399 142 622 294 327 460 % % % % % % % % % % % % % % % % % % % % % % % On a scale of 0 to 10, where 0 means you would never consider voting for them, and 10 means you would definitely consider voting for them, how likely are you to consider voting for the following parties at the next election? Conservative 0 - Would never consider voting for them 38 8 58 40 45 26 38 37 45 40 39 27 36 40 35 33 37 44 42 100 0 0 0 1 6 2 9 12 7 4 7 5 3 8 5 3 5 7 4 7 4 6 9 0 32 0 0 2 5 1 6 11 6 3 5 5 7 5 5 4 5 6 7 4 5 5 6 0 28 0 0 3 4 2 6 10 5 3 4 3 7 4 3 3 4 3 5 4 3 4 4 0 21 0 0 4 3 2 3 2 3 3 3 3 5 4 3 2 3 3 3 3 5 2 3 0 19 0 0 5 10 10 8 6 8 11 8 13 10 11 9 10 9 12 15 10 10 8 13 0 0 52 0 6 4 4 5 5 3 7 5 4 7 5 4 3 5 4 6 4 5 4 3 0 0 22 0 7 5 11 2 4 5 7 6 5 3 5 6 6 5 5 5 5 6 6 2 0 0 26 0 8 5 10 1 4 4 8 5 5 1 5 7 5 6 4 3 6 4 5 5 0 0 0 20 9 3 7 0 3 2 4 3 3 3 2 3 5 4 2 4 4 2 2 3 0 0 0 12 10 - Would definitely consider voting for them 17 44 2 4 12 26 16 18 7 11 16 33 19 14 11 21 17 15 11 0 0 0 68 AVERAGE 3.9 7.5 1.6 2.6 3.1 5.4 3.8 4.1 2.8 3.3 3.9 5.5 4.2 3.5 -

Unity, Vision and Brexit
1 ‘Brexit means Brexit’: Theresa May and post-referendum British politics Nicholas Allen Department of Politics and International Relations Royal Holloway, University of London Surrey, TW20 0EX [email protected] Abstract: Theresa May became prime minister in July 2016 as a direct result of the Brexit referendum. This article examines her political inheritance and leadership in the immediate wake of the vote. It analyses the factors that led to her victory in the ensuing Tory leadership contest and explores both the main challenges that confronted her and the main features of her response to them. During his first nine months in office, May gave effect to the referendum, defined Brexit as entailing Britain’s removal from membership of the European Union’s single market and customs union and sought to reposition her party. However, her failure to secure a majority in the 2017 general election gravely weakened her authority and the viability of her plans. At time of writing, it is unclear how much longer her premiership can last or if she will be able to exercise effective leadership over Brexit. Keywords: Theresa May; Brexit; prime ministers; leadership; Conservative party This is a post-peer-review, pre-copyedit version of an article published in British Politics. The definitive publisher-authenticated version, Nicholas Allen (2017) ‘‘Brexit means Brexit’: Theresa May and post-referendum British politics’, British Politics, First Online: 30 November, doi.org/10.1057/s41293-017-0067-3 is available online at: https://link.springer.com/article/10.1057/s41293-017-0067-3 2 Introduction According to an old university friend, Theresa May had once wanted to be Britain’s first female prime minister (Weaver, 2016). -

How Andrea Leadsom Could Have Avoided the Debate About Her Times Interview
This is the newspaper article at the centre of the furore Jul 09, 2016 20:58 +08 How Andrea Leadsom could have avoided the debate about her Times interview Do parents make better government leaders than childless people? This question has become a big source of embarassment for Andrea Leadsom, who is competing with Theresa May to lead the Conservative Party and become the United Kingdom's Prime Minister after David Cameron steps down. At issue is a newspaper interview with the London Times, in which she suggested that being a mother made her more qualified than the childless May. "I feel being a mum means you have a very real stake in the future of our country, a tangible stake," she is quoted as saying. When the article was published, she was incensed, saying in a tweet: Truly appalling and the exact opposite of what I said. I am disgusted. https://t.co/DPFzjNmKie — Andrea Leadsom MP (@andrealeadsom) July 8, 2016 Journalist Rachel Sylvester defended the article in an interview with the BBC, saying that "...the article was 'fairly written up' and she was 'baffled' by Mrs Leadsom's 'rather aggressive reaction'." (full article under Links) Times Deputy Editor Emma Tucker tweeted the relevant part of the transcript: Transcript from the key part of the interview with Andrea Leadsom this morning in @thetimespic.twitter.com/aFtIECBIiC — Emma Tucker (@emmatimes2) July 8, 2016 David Cameron weighed in with his own tongue-in-cheque assessment: I'm disgusted that Andrea #Leadsom has been reported saying exactly what she actually said. Shoddy journalism. -

Parliamentary Conventions
REPORT Parliamentary Conventions Jacqy Sharpe About the Author Jacqy Sharpe is a former Clerk in the House of Commons. Her period as Clerk of the Journals provided her with significant insight into the historical and contemporary context of parliamentary conventions and procedure. Message from the Author With thanks to Dr Andrew Blick, Sir David Beamish, Helen Irwin and Sir Malcolm Jack for their comments on drafts of this paper. The conclusions, and any errors or omissions, are, of course, the responsibility of the author. Parliamentary Conventions Executive Summary “General agreement or consent, as embodied in any accepted usage, standard, etc”1 “Rules of constitutional practice that are regarded as binding in operation, but not in law”2 “[B]inding rules of behaviour accepted by those at whom they are directed. A practice that is not invariable does not qualify.”3 A list of various conventions with a note on how, if at all, they, or the approaches to them, have lately been modified or changed: CONVENTION CURRENT POSITION Conventions relating to behaviour in the House of Commons Speaking in the House of Commons Members should address the House through the Chair Although both questioned and frequently breached, and refer to other Members in the third person, by the convention is generally accepted constituency or position. Except for opening speeches, maiden speeches and Accepted and generally observed where there is special reason for precision, Members should not read speeches, though they may refer to notes Attendance at debates Members -

Download Andrea Leadsom
Northampton Forward Board: Register of Interests October 2020 As board member of the Northampton Forward Board, I declare that I have the following disclosable interests. Please state ‘none’ where appropriate, do not leave any boxes blank. Each board member shall review their individual register of interests at the beginning of every financial year or as there are any changes. Name: Job Role: SECTION 1 ANY EMPLOYMENT, OFFICE. TRADE, PROFESSION OR VOCATION DECLARATION CARRIED ON FOR PROFIT OR GAIN 1.1 Name of: Paid as a Member of Parliament by the • Your employer Independent Parliamentary Standards Authority • Any business carried out by you • Any other role in which you receive renumeration (this includes remunerated roles such as councillors) 1.2 Description of employment or business activity Member of Parliament for South Northamptonshire 1.3 The name of any firm in which you are a partner N/A 1.4 The name of any company for which you are a remunerated director N/A SECTION 2 SPONSORSHIP DECLARATION 2.1 Any financial benefit obtained which is paid as a result of carrying out N/A duties as a Board Member. This includes any permanent or financial benefit from a Trade Union within the meaning of the Trade Union and Labour Relations (Consolidation) Act 1992 (a). SECTION 3 CONTRACTS DECLARATION 3.1 Any contract for goods, works or services which has not been fully N/A discharged by any organisation named at 1.1. 3.2 Any contract for goods, works or services entered into by any organisation N/A named at 1.1. -

BIA Briefing on the Conservative Party Leadership Candidates
BIA briefing on the Conservative Party leadership candidates June 2019 Contents The candidates...................................................................................................................................................... 2 The election process ............................................................................................................................................. 3 Biographies ........................................................................................................................................................... 4 Michael Gove ............................................................................................................................................ 4 Matt Hancock ........................................................................................................................................... 4 Mark Harper ............................................................................................................................................. 5 Jeremy Hunt ............................................................................................................................................ 6 Sajid Javid ................................................................................................................................................ 6 Boris Johnson .......................................................................................................................................... 7 Andrea Leadsom ..................................................................................................................................... -

EU Referendum 2016 V7
EU Referendum 2016 Three Scenarios for the Government An insights and analysis briefing from The Whitehouse Consultancy Issues-led communications 020 7463 0690 [email protected] whitehouseconsulting.co.uk The EU Referendum The EU referendum has generated an unparalleled level of political If we vote to leave, a new Prime Minister will likely emerge from among debate in the UK, the result of which is still too close to call. Although the 'Leave' campaigners. What is questionable is whether Mr Cameron we cannot make any certain predictions, this document draws upon will stay in position to deal with the immediate questions posed by Whitehouse’s political expertise and media analysis to suggest what Brexit: such as the timetable for withdrawal, or how trading and may happen to the Government’s composition in the event of: diplomatic relations will proceed. Will he remain at Number 10, perhaps • A strong vote to remain (by 8% or more); until a party conference in the autumn, or will there be more than one new beginning? • A weak vote in favour of remaining (by up to 8%); or • A vote to leave. “The result could create If the UK chooses to remain by a wide margin, the subsequent reshue will aord an opportunity to repair the Conservative Party after a a new political reality.” bruising campaign period. This result will prompt a flurry of It is clear that the referendum result could create a new political reality on parliamentary activity, renewing the Prime Minister’s mandate until he 24 June. Businesses must be prepared to engage if they are to mitigate the stands down closer to 2020 and enable a continuation of the impacts and take advantage of the opportunities presented. -

Cabinet Committee Membership Lists
Cabinet December Committee Membership 2014 Lists 1 Contents Coalition Committee ................................................................................................... 3 Devolution Committee ................................................................................................ 4 Economic Affairs Committee ...................................................................................... 5 Economic Affairs (Infrastructure) sub-Committee ................................................... 6 Economic Affairs (Reducing Regulation) sub-Committee ....................................... 7 European Affairs Committee ...................................................................................... 8 European Affairs sub-Committee ............................................................................ 9 Flooding Committee ................................................................................................. 10 Growth and Enterprise Committee ........................................................................... 11 Home Affairs Committee .......................................................................................... 12 Home Affairs (Armed Forces Covenant) sub-Committee ...................................... 14 Home Affairs (Greening Government Commitments) sub-Committee .................. 15 Local Growth Committee .......................................................................................... 16 Local Growth sub-Committee .............................................................................. -

Tories Should Have Faith in Their Grassroots; Party Members Must Not Be Banned from Electing a Leader - They Need More Power, Not Less
5th September 2016, The Times, http://www.thetimes.co.uk/article/tories-should-have-faith-in-their- grassroots-bqn3b9fns Tories should have faith in their grassroots; Party members must not be banned from electing a leader - they need more power, not less Mark Wallace What possessed the members of the Conservative Party, 15 years ago this month? Newly entrusted with the power to choose their leader, they proceeded to elect Iain Duncan Smith, one of the most woeful opposition leaders of modern times. The decision has been interpreted ever since by MPs and observers alike as a sign that card-carrying Conservatives are deranged - "swivel-eyed loons", in the alleged words of a certain former senior CCHQ official. The experience left scars on the parliamentary Conservative Party. When Mr Duncan Smith was unseated in 2003, MPs refused to offer the membership any choice at all, opting unanimously for Michael Howard. When Mr Howard stood down in 2005, he attempted to strip the membership of their power and put MPs completely in charge once more. The 1922 Committee supported him. Happily, after concerted resistance, the proposal to return the party to feudalism failed to pass. So it isn't a surprise to see the idea crop up again, raised this time by Andrew Tyrie, chairman of the Treasury select committee, who was cheerleader for Mr Howard's proposals the first time round. In Mr Tyrie's letter, Andrea Leadsom's name has joined Mr Duncan Smith's in the column marked "cautionary tales". He argues that her withdrawal from the leadership race was a "narrow escape" for the government, which could have been saddled with a prime minister who did not have the support of MPs. -
List of Ministers' Interests
LIST OF MINISTERS’ INTERESTS CABINET OFFICE DECEMBER 2015 CONTENTS Introduction 1 Prime Minister 3 Attorney General’s Office 5 Department for Business, Innovation and Skills 6 Cabinet Office 8 Department for Communities and Local Government 10 Department for Culture, Media and Sport 12 Ministry of Defence 14 Department for Education 16 Department of Energy and Climate Change 18 Department for Environment, Food and Rural Affairs 19 Foreign and Commonwealth Office 20 Department of Health 22 Home Office 24 Department for International Development 26 Ministry of Justice 27 Northern Ireland Office 30 Office of the Advocate General for Scotland 31 Office of the Leader of the House of Commons 32 Office of the Leader of the House of Lords 33 Scotland Office 34 Department for Transport 35 HM Treasury 37 Wales Office 39 Department for Work and Pensions 40 Government Whips – Commons 42 Government Whips – Lords 46 INTRODUCTION Ministerial Code Under the terms of the Ministerial Code, Ministers must ensure that no conflict arises, or could reasonably be perceived to arise, between their Ministerial position and their private interests, financial or otherwise. On appointment to each new office, Ministers must provide their Permanent Secretary with a list in writing of all relevant interests known to them which might be thought to give rise to a conflict. Individual declarations, and a note of any action taken in respect of individual interests, are then passed to the Cabinet Office Propriety and Ethics team and the Independent Adviser on Ministers’ Interests to confirm they are content with the action taken or to provide further advice as appropriate.