Tongmai Yangxin Intervening in Myocardial Remodeling After PCI For
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
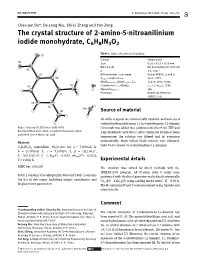
The Crystal Structure of 2-Amino-5-Nitroanilinium Iodide Monohydrate, C6H8IN3O2
Z. Kristallogr. NCS 2021; 236(4): 725–726 Chao-Jun Du*, De-Long Niu, Shi-Li Zheng and Yan Zeng The crystal structure of 2-amino-5-nitroanilinium iodide monohydrate, C6H8IN3O2 Table : Data collection and handling. Crystal: Yellow block Size: . × . × . mm Wavelength: Mo Kα radiation (. Å) μ: . mm− Diffractometer, scan mode: Bruker APEX-II, φ and ω θmax, completeness: .°,>% N(hkl)measured,N(hkl)unique, Rint: , , . Criterion for Iobs, N(hkl)gt: Iobs > σ(Iobs), N(param)refined: Programs: Bruker [], Olex [], SHELX [, ] Source of material All of the reagents are commercially available and were used without further purification. 1.53 g 4-nitrobenzene-1,2-diamine https://doi.org/10.1515/ncrs-2021-0058 (10mmol)wasaddedtoasolutionmixedby9mLTHFand Received February 8, 2021; accepted February 25, 2021; 1 mL hydroiodic acid (40%). Afterstirringfor10minatroom published online March 19, 2021 temperature, the solution was filtered and let evaporate automatically. Many yellow block crystals were obtained, Abstract yield 74.6% (based on 4-nitrobenzene-1,2-diamine). C6H8IN3O2, monoclinic, P21/n (no. 14), a = 7.0704(3) Å, b = 15.7781(6) Å, c = 9.1495(4) Å, β = 112.114(1)°, 3 2 V = 945.61(7) Å , Z =4,Rgt(F) = 0.0187, wRref(F ) = 0.0522, T = 150(2) K. Experimental details CCDC no.: 2065269 The structure was solved by direct methods with the SHELXS-2018 program. All H-atoms from C atoms were Table 1 contains crystallographic data and Table 2 contains positioned with idealized geometry and refined isotropically the list of the atoms including atomic coordinates and (Uiso(H) = 1.2Ueq(C)) using a riding model with C–H=0.95Å. -

Highlightes Pf Environmental Impact Assessment
E-174 VOL. 6 Public Disclosure Authorized National Highway Project Upgrading Xinxiang--Zhengzhou class I ° highway to Expressway Standard Highlightes pf Environmental Impact Public Disclosure Authorized Assessment (Third Revised Version) SCAt4INEDV1E6F Public Disclosure Authorized FILE(Cola g LrG r 6WTENW SA P Henan Provincial Environmental Protection Institute Public Disclosure Authorized October, 1998 1. Description of the Proposed Project 1) Upgrading work on Xinxiang--Zhengzhou class I highway is a temporary work to achieve original capacity of the existing class I highway before building of Xinxiang-- zhengzhou Expressway. The proposed section for upgrading, till year 2004 , will take two in one" status between BeiJing--shenzhen National Trunk Highway and National highway 107 . After year 2004 upon completion of Xinxiang--zhengzhou expressway and the second Zhengzhou Yellow River Bridge at new alternative alignment , the upgraded section will mainly take the traffic volume on National highway 107 2) Based upon the recommended alignment , Upgrading work on Xinxiang--zhengzhou class I highway consist of : North section of the Yellow River Bridge(starting from the terminal point on Anxin expressway ending to the north bank of YR ): this section is 39.326km long with fully-access-controled and service road being built . There need to be newly built 1 simple interchange, 24 overpass separation interchanges, to reconstruct 1 toll station, 9 passageways ,newly built 9 small bridges, and 7 middle bridges ,150 culverts as well as 29.848km of approach road and service road and 43.5km of continuous road ; the section from the north bank of YR to Longhai railway interchange (south section.to north bank of YR involves the Yellow River Bridge itself ): this section is 30.447km in total and will be provided with barrier (fence) for isolating motorized and non-motorized vehicle lane . -

World Bank Document
February 28, 2000 Governor Li Kegiang People’s Government of Henan Province Public Disclosure Authorized No. 10 Wei-er road Zhengzhou 450003 Henan Province People’s Republic of China Dear Governor Li: RE: National Highway Project (LN 3748-CHA) Amendment to Henan Project Agreement 1. I refer to (i) the Loan Agreement between People’s Republic of China (the Borrower) and the International Bank for Reconstruction and Development (the Bank) dated July 20, 1994 for the above-mentioned Project, as amended by a Letter of Amendment dated August 18, 1997 (together the Loan Agreement), and (ii) the Project Agreement between the Bank and Henan Province (Henan) dated July 20, 1994, for the Henan Part of the Project (the Henan Project Agreement). I also refer to the letter dated January 31, 2000 from Mr. Wu Gang, Deputy Director-General, International Department, Ministry of Finance, on behalf of the Borrower, requesting a re-allocation Public Disclosure Authorized of the proceeds of the Loan to allow the upgrading of the Xinxiang- Zhengzhou Highway to be included in the Henan Part of the Project. 2. I am pleased to inform you that the Bank hereby concurs with the Borrower’s proposal to modify the Project and re-allocate the proceeds of the Loan. To give effect to such proposal, the Bank hereby agrees to amend the Project Agreement in accordance with the following paragraphs. 3. Section 1.01 of the Henan Project Agreement is amended as follows: “Section 1.01. […] (a) “Environmental Action Plan” means collecctively (i) the Anyang-Xinxiang Expressway Environmental Protection Measures, Management and Monitoring Action Plan, dated September 1993, and (ii) the Environmental Action Plan for the Upgrading Works Between Xinxiang and Zhengzhou, dated November 1998, both prepared by Henan Environmental Protection Research Institute; as the same may be revised from time to time with the prior agreement of the Bank. -

Asymmetric Α-Alkylation of Β-Keto Esters and Β-Keto Amides by Phase-Transfer Catalysis
Electronic Supplementary Material (ESI) for Organic & Biomolecular Chemistry. This journal is © The Royal Society of Chemistry 2018 Asymmetric α-Alkylation of β-keto esters and β-keto amides by Phase-transfer catalysis Yakun Wang,a* Yueyun Li,b Mingming Lian,c Jixia Zhang,a Zhaomin a d d d Liu, Xiaofei Tang, Hang Yin and Qingwei Meng a School of Pharmacy, Xinxiang Medical University, Xinxiang, Henan 453003, PR China. E-mail: [email protected]. Fax: (+86)-0373-3029879 b Xinxiang Central Hospital, Xinxiang Medical University, Xinxiang, Henan 453003, PR China. c Department of Pharmaceutics, Daqing Campus, Harbin Medical University, Daqing, Heilongjiang 163319, P. R. China d School of Pharmaceutical Science and Technology, Dalian University of Technology, Dalian, Liaoning 116024, P. R. China. A. General Information ........................................................................................... 2-3 B. NMR spectra and HPLC .................................................................................. 4-96 1 A. General Information: Unless otherwise stated, all commercial reagents and solvents were used without further additional purification. Analytical TLC was visualized with UV light at 254 nm. Thin layer chromatography was carried out on TLC aluminum sheets with silica gel 60 F254. Purification of reaction products was carried out with chromatography on silica gel 60 (200-300 mesh)... 1H NMR (400 MHz) spectra was obtained at 25 °C ; 13C NMR (100 MHz) were recorded on a VARIAN INOVA-400M and AVANCE II 400 spectrometer at 25 °C. Chemical shifts are reported as δ (ppm) values relative to TMS as internal standard and coupling constants (J) in Hz. The enantiomeric excesses (ee) were determined by HPLC. HPLC analyses were performed on equipped with Diacel Chiralpak AD-H, OJ-H and AS-H chiral column (0.46 cm × 25 cm), using mixtures of n-hexane/isopropyl alcohol as mobile phase, at 25 °C . -
Henan WLAN Area
Henan WLAN area NO. SSID Location_Name Location_Type Location_Address City Province Xuchang College East Campus Ningyuan Dormitory Building No.1, Jinglu 1 ChinaNet School No.88 Bayi Road, Xuchang City ,Henan Province Xuchang City Henan Province Dormitory Building No.1,4,5 2 ChinaNet Henan University Student Apartment School Jinming Road North Section, Kaifeng City, Henan Province Kaifeng City Henan Province North of 500 Meters West Intersection between Jianshe Road and Muye Road 3 ChinaNet Henan Province, Xinxiang City, Henan Normal University Old campus School Xinxiang City Henan Province ,Xinxiang City, Henan Province Physical Education College of Zhengzhou University Dormitory Building 4 ChinaNet School Intersection between Sanquan Road and Suoling Road Zhengzhou City Henan Province 1# Physical Education College of Zhengzhou University Dormitory Building 5 ChinaNet School Intersection between Sanquan Road and Suoling Road Zhengzhou City Henan Province 2# Physical Education College of Zhengzhou University Dormitory Building 6 ChinaNet School Intersection between Sanquan Road and Suoling Road Zhengzhou City Henan Province 5# Zhengzhou Railway Vocational Technology College Tieying Street 7 ChinaNet School Tieying Street ,Erqi District, Zhengzhou City Zhengzhou City Henan Province Campus Dormitory Building No.4 8 ChinaNet Henan Industry and Trade Vocational College Dormitory Building No.3 School No.1,Jianshe Road,Longhu Town Zhengzhou City Henan Province Zhengzhou Broadcasting Movie and Television College Administration 9 ChinaNet School -

HR Water Consumption Marginal Benefits and Its Spatial–Temporal Disparities in Henan Province, China
Desalination and Water Treatment 114 (2018) 101–108 www.deswater.com May doi: 10.5004/dwt.2018.22345 HR water consumption marginal benefits and its spatial–temporal disparities in Henan Province, China Subing Lüa,b, Huan Yanga, Fuqiang Wanga,b,c,*, Pingping Kanga,b aNorth China University of Water Resources and Electric Power, Henan Province 450046, China, email: [email protected] (F. Wang) bCollaborative Innovation Center of Water Resources Efficient Utilization and Support Engineering, Henan Province 450046, China cHenan Key Laboratory of Water Environment Simulation and Treatment, Henan Province 450046, China Received 7 November 2017; Accepted 4 February 2018 abstract Water is one of the essential resources to production and living. Agriculture, industry, and living are considered as the direct water consumption. This paper employs the concept of marginal product value to estimate the water consumption marginal benefits in Henan Province. We use data on agri- cultural water consumption, industrial water consumption, and domestic water consumption of 18 cities in Henan Province surveyed from 2006 to 2013 and considered the Cobb–Douglas production function. The results showed that, during the study period, except for the marginal benefit of agricul- ture in high developed area, the industrial and domestic water use increased, and the industrial and domestic water use benefits were much higher than agricultural. At the same time, the benefit of the developed area was higher than the developing area. The benefits of agricultural water consumption and industrial water consumption in high developed area have made great improvements gradually, while benefits in low developed area have made small changes; but the benefits of domestic water con- sumption presented the opposite trend. -

Announcement of Interim Results for the Six Months Ended 30 June 2021
Hong Kong Exchanges and Clearing Limited and The Stock Exchange of Hong Kong Limited take no responsibility for the contents of this announcement, make no representation as to its accuracy or completeness and expressly disclaim any liability whatsoever for any loss howsoever arising from or in reliance upon the whole or any part of the contents of this announcement. (Stock Code: 0832) ANNOUNCEMENT OF INTERIM RESULTS FOR THE SIX MONTHS ENDED 30 JUNE 2021 FINANCIAL HIGHLIGHTS • Revenue for the six months ended 30 June 2021 amounted to RMB20,357 million, an increase of 56.4% compared with the corresponding period in 2020. • Gross profit margin for the period was 17.9%, a decrease of 5.8 percentage points compared with 23.7% for the corresponding period in 2020. • Profit attributable to equity shareholders of the Company for the period amounted to RMB729 million, an increase of 0.3% compared with the corresponding period in 2020. • Profit for the period was RMB1,025 million, representing an increase of 30.4% compared with the corresponding period in 2020. • Net profit margin for the period was 5.0%, a decrease of 1.0 percentage point compared with 6.0% for the corresponding period in 2020. • Basic earnings per share for the period was RMB25.63 cents, a decrease of 3.0% compared with the corresponding period in 2020. • Declaration of an interim dividend of HK14.75 cents per share for the six months ended 30 June 2021. 1 INTERIM RESULTS The board (the “Board”) of directors (the “Directors” and each a “Director”) of Central China Real Estate -
Spatiotemporal Evolution Analysis of NO2 Column Density Before and After COVID-19 Pandemic in Henan Province Based on SI-APSTE Model
Spatiotemporal Evolution Analysis of NO 2 Column Density before and after COVID-19 Pandemic in Henan Province Based on SI-APSTE Model Yang Liu Henan University Jinhuan Zhao Henan University Kunlin Song Beijing Institute of Technology Cheng Cheng Henan University Shenshen Li Chinese Academy of Sciences Kun Cai ( [email protected] ) Henan University Research Article Keywords: Swarm Intelligence based Air Pollution SpatioTemporal Evolution (SI-APSTE), air pollution Posted Date: April 16th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-403101/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Spatiotemporal Evolution Analysis of NO2 Column Density before and after COVID-19 Pandemic in Henan Province Based on SI-APSTE Model Yang Liu 1 , Jinhuan Zhao1, Kunlin Song3, Cheng Cheng1, Shenshen Li2 , Kun Cai1 1Henan Engineering Laboratory of Spatial Information Processing, Henan Key Laboratory of Big Data Analysis and Processing, School of Computer and Information Engineering, Henan University, Kaifeng 475004, PR China 2State Key Laboratory of Remote Sensing Science, Aerospace Information Research Institute, Chinese Academy of Sciences, Beijing 100101, PR China 3School of Information and Electronics, Beijing Institute of Technology, Beijing 100081, PR China corresponding.author: K. Cai ([email protected]), S. Li ([email protected]), Y. Liu ([email protected]) Abstract Air pollution is the result of comprehensive evolution of a dynamic and complex system composed of emission sources, topography, meteorology and other environmental factors. The establishment of spatiotemporal evolution model is of great significance for the study of air pollution mechanism, trend prediction, identification of pollution sources and pollution control. -

Performance of Alfalfa Varieties with Different Fall Dormancy Across Different Production Areas of Henan Province of China
African Journal of Agricultural Research Vol. 7(46), pp. 6197-6203, 5 December, 2012 Available online at http://www.academicjournals.org/AJAR DOI: 10.5897/AJAR12.644 ISSN 1991-637X ©2012 Academic Journals Full Length Research Paper Performance of alfalfa varieties with different fall dormancy across different production areas of Henan Province of China Gong-min Xu, Xue-bing Yan, Cheng-zhang Wang*, Yan-hua Wang and Wen-na Fan College of Animal Science and Veterinary Medicine, Henan Agricultural University, 450002, Zhengzhou, China. Accepted 23 July, 2012 Nineteen alfalfa varieties of seven different fall dormancy (FD) classes (2 to 8) over three years in five different eco-agricultural areas with mild climates in Henan Province of China was studied. The results showed that almost all of the varieties exhibited nearly perfect survival rates, while the variety ‘Siriver’ had a slightly lower survival rate of 98.5%. The variety ‘WL414’ (FD 6) produced the greatest average dry matter (DM) yield across the regions, while the lowest yield was found in ‘Golden Empress’ (FD 2). In addition, the total dry matter (DM) yields of the three years were affected by location and variety and there was significant location × variety interaction. The FD classes and total DM yields were significantly correlated, indicating that FD class should be used as one of the main criterion for alfalfa variety improvement or introduction of new varieties into a temperate region, such as Central China. Beside, special attention should also be paid to the selection of varieties suitable to local conditions because other factors have important influence on DM yields, including the characteristics of a varieties and environmental conditions. -

Download Article
International Conference on Economics, Management, Law and Education (EMLE 2015) Comparative Analysis on Economic Competitiveness of Kaifeng Based on Henan Province Shuang Qiu Yanfang Li China West Normal University China West Normal University Nanchong, Sichuan, China 637009 Nanchong, Sichuan, China 637009 Abstract—Although Kaifeng has achieved some remarkable also a famous historical city with thousands of years culture. results in recent years, in terms of comparing with other cities in Henan province the development of Kaifeng is relatively In recent years, although the economic and social backward. Based on the municipal economic data of Henan programs of Kaifeng developed rapidly, and the tourism and province from 2006 to2013, by using the Factor Analysis, we business of Kaifeng has made remarkable achievements, its demonstrate a comparative and research on urban infrastructure construction in Henan province is still in the competitiveness of Kaifeng in Henan province. Through comparison of low-ranking, comprehensive competitiveness comparative analysis, we find that the economy of Kaifeng is of the capital, such as: talent capital, financial capital, relatively lag, comparing with the other 16 cities in Henan science and technology, economic structure and enterprise province Kaifeng's ranking are basically after ten, finally we management etc. is weakness 【 4 】 .Now along with our put forward some suggestions on the development of Kaifeng. country proposed "Proposal on Rise of the Central Region" and the strategy of "Zhongyuan urban agglomeration Keywords—Kaifeng; economic competitiveness; comparative construction strategy" in Henan province, Kaifeng has analysis ushered in the good opportunities for development. So It has been an important task for how to effectively grasp the I. -

Propofol Suppresses Proliferation and Invasion of Gastric Cancer Cells Via Downregulation of Microrna-221 Expression
Propofol suppresses proliferation and invasion of gastric cancer cells via downregulation of microRNA-221 expression Z.T. Wang1, H.Y. Gong2, F. Zheng3, D.J. Liu1 and X.Q. Yue2 1Department of Anesthesiology, The Second Affiliated Hospital of Zhengzhou University, Jinshui District, Zhengzhou, China 2Department of Anesthesiology, The First Affiliated Hospital of Xinxiang Medical University, Weihui, Xinxiang, Henan, China 3Department of Medical Ultrasonics, The First Affiliated Hospital of Xinxiang Medical University, Weihui, Xinxiang, Henan, China Corresponding author: X.Q. Yue E-mail: [email protected] Genet. Mol. Res. 14 (3): 8117-8124 (2015) Received January 26, 2015 Accepted April 17, 2015 Published July 17, 2015 DOI http://dx.doi.org/10.4238/2015.July.17.20 ABSTRACT. Propofol is one of the extensively and commonly used intravenous anesthetic agents. The current study aimed to evaluate the effects of propofol on the behavior of human gastric cancer cells and the molecular mechanisms of this activity. The effects of propofol on SGC7901 and AGS cell proliferation, apoptosis, and invasion Genetics and Molecular Research 14 (3): 8117-8124 (2014) ©FUNPEC-RP www.funpecrp.com.br Z.T. Wang et al. 8118 were detected by MTT assay, flow cytometric analysis, and matrigel invasion assay. Real-time polymerase chain reaction (PCR) was used to assess microRNA (miR)-221 expression. miR-221 mimics were transfected into SGC7901 and AGS cells to assess the role of miR- 221 in propofol-induced anti-tumor activity. Propofol significantly inhibited cell proliferation and invasion and promoted apoptosis of SGC7901 and AGS cells. Propofol also efficiently reduced miR-221 expression. Moreover, transfection of miR-221 mimics reversed the effects of propofol on the biological behavior of gastric cancer cells. -

Sashenanformatted240810 1.Pdf
China Climate Change Partnership Framework - Enhanced strategies for climate-proofed and environmentally sound agricultural production in the Yellow River Basin (C-PESAP) Situation Analysis Report of Agriculture Production and Climate Change in Henan Province Compiled and Written by Zhang Canjun, Yao Yuqin, Lu Junjie, Shen Dongfeng, Zhang Jie Luoyang Academy of Agricultural Sciences Shen Alin, Zheng Feng Henan Academy of Agricultural Sciences China Climate Change Partnership Framework - Enhanced strategies for climate-proofed and environmentally sound agricultural production in the Yellow River Basin (C-PESAP) Contents 1 Introduction............................................................................................................................. 3 1.1 Background and rationale of the study............................................................................ 3 1.2 General description of the study area.............................................................................. 4 2 Agricultural situation in the Yellow River Basin ................................................................. 5 2.1 Middle region - Henan ..................................................................................................... 5 2.1.1 Production and cropping systems.............................................................................. 5 2.1.2 Socio-economic aspects............................................................................................ 9 2.1.3 Partners and stakeholder institutions......................................................................