The Health of the People of Helensburgh and Lomond
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Argyll & Bute M&G
Argyll & Bute M&G 15/09/2017 09:54 Page 1 A to Tarbert to Port Bannatyne Frequency in minutes Campbeltown 8 3 Ring and Ride Campbeltown Rothesay T operates throughout A 443 BUS and COACH SERVICES Mondays R this map B 449 90 . E L 0 250 500 metres Rothesay P R 477 Guildford Square Y Service to Fridays Saturdays Sundays T 926 Bay R E Please note that the frequency of services generally applies to school terms. During school holidays T to H terminating: T ILL R 0 200 400 yards 479 A A S O B Ascog, Number Operator Route Days Eves Days Eves ID A R E A 490 G 90.477.479.488 .491.492 some services are reduced and these frequencies are shown in brackets, for example "4(2) jnys" CRAIG K C . Mount Stuart D G NO A Y T ROA OW CK D L calling: S Calton SC E 493 and Kilchattan D RD AL M E S . BE Y E shows that there are 4 journeys during school terms and 2 journeys during school holidays. R S 490.493 C Bay 471 TSS Tighnabruaich - Kames (Tues & Thurs only) 4(5) jnys - - - - VE T R 90 A . W D T N 100 I D W 100 A EST . R R . L LAND E 488 R AR 440 A S ROA E P E D Tighnabruaich - Portavadie (Tues & Thurs only) 2 jnys - - - - A UA Y T T 440 N S V Frequency in minutes A ST 100. A 490 V D . E A 300 A A . -
Weekly List of Valid Planning Applications Week Ending 13 June 2014
Weekly Planning list for 13 June 2014 Page 1 Argyll and Bute Council Planning Weekly List of Valid Planning Applications Week ending 13 June 2014 13/6/2014 10:5 Weekly Planning list for 13 June 2014 Page 2 Bute and Cowal Reference: 14/01057/PPP Officer: Br ian Close Telephone: 01546 605518 Ward Details: 20 - Cowal Community Council: Dunoon Community Council Proposal: Redevelopment of for mer garden centre to for m amixed resi- dential development with associated amenity and parking spa- ces along with a newpublic square Location: Former Garden Centre,6Mar ine Parade,Kir n, Dunoon, Argyll And Bute,PA23 8HE Applicant: Dr ummond Park Dev elopments Ltd Ecclesmachan House,Ecclesmachan, EH52 6NJ,West Loth- ian Ag ent: Mosaic Architecture 100 West Regent Street, Glasgow, G22QD Development Type: 03B - Housing - Local Grid Ref: 218428 - 677983 Reference: 14/01088/PP Officer: Br ian Close Telephone: 01546 605518 Ward Details: 20 - Dunoon Community Council: South CowalCommunity Council Proposal: Erection of dwellinghouse including for mation of vehicular access and installation of private water supply and drainage systems. Location: Land ToSouth Of Glenstriven House,Toward, Dunoon, Argyll And Bute,PA23 7UN Applicant: Mr P Blacker Glenstr iven House,Toward, Dunoon, Argyll And Bute,PA23 7UN Ag ent: CDenovan 19 Eccles Road, Hunters Quay, Dunoon, PA23 8LA Development Type: 03B - Housing - Local Grid Ref: 208216 - 678149 Reference: 14/01193/PP Officer: Allocated ToArea Office Telephone: 01546 605518 Ward Details: 20 - Dunoon Community Council: South CowalCommunity -
View Preliminary Assessment Report Appendix C
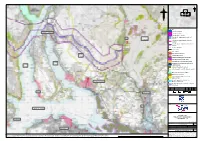
N N ? ? d c b a Legend Corrid or 4 e xte nts GARELOCHHEAD Corrid or 5 e xte nts Corrid or 4 & 5 e xte nts Corrid or 4 – ap p roxim ate c e ntre of A82 LOCH c orrid or LOMOND Corrid or 5 – ap p roxim ate c e ntre of c orrid or Corrid or 4 & 5 – ap p roxim ate c e ntre of c orrid or G A L iste d Build ing Gre at T rails Core Paths Sc he d ule d Monum e nt GLEN Conse rvation Are a FRUIN Gard e n and De signe d L and sc ap e Sp e c ial Prote c tion Are a (SPA) Sp e c ial Are a of Conse rvation (SAC) GARE LOCH W e tland s of Inte rnational Im p ortanc e LOCH (Ram sar Site s) LONG Anc ie nt W ood land Inve ntory Site of Sp e c ial Sc ie ntific Inte re st (SSSI) Marine Prote c te d Are a (MPA) ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! National Sc e nic Are a L oc h L om ond and the T rossac hs National Park Flood Map p ing Coastal Exte nts – HELENSBURGH Me d ium L ike lihood Flood Map p ing Rive r Exte nts – Me d ium L ike lihood P01 12/02/2021 For Information TS RC SB DR Re v. Re v. Date Purp ose of re vision Orig/Dwn Che c kd Re v'd Ap p rv'd COVE BALLOCH Clie nt Proje c t A82 FIRTH OF CLYDE Drawing title FIGU RE C.2A PREL IMINARY ASSESSMENT CORRIDORS 4, 5 DUNOON She e t 01 of 04 Drawing Status Suitab ility FOR INFORMATION S2 Sc ale 1:75,000 @ A3 DO NOT SCALE Jac ob s No. -

Post 17.08.11 Updates
June 2015 Willow Wind Farm Community Liaison Group - Terms of Reference 1. Role of Liaison Group 1.1 The group will be known as the Willow Wind Farm Community Liaison Group (WWFCLG), hereafter referred to in this document as “the CLG”. The proposed Good Energy Project will be referred to as the “project” for the remainder of this document. 1.2 The aim of the CLG is to provide a forum for discussion and the exchange of information in regards to the development, construction and operation of the proposed project. The CLG will provide an important channel of communication between Good Energy representatives, elected representatives and the local community, initially during the pre- application phase of the project. 1.3 The Group will: Receive progress updates from Good Energy about the site and proposals; Address questions and concerns arising from the surrounding communities; and Establish workshop discussions on key specific elements of the proposals, development and operation of the site (such as construction periods, ecological impact, traffic management and community benefits). 1.4 The local community is defined by those living or working in the vicinity of the proposed site. 1.5 Discussions undertaken by the CLG are restricted to matters relating to the proposed project. 2. The Group Membership 2.1 The following people have been invited to join the CLG: Mr David Love (Senior Planning Officer, Argyll & Bute Council) Cllr Anne Horn (Ward councillor, Kintyre and the Islands) Cllr John McAlpine (Ward councillor, Kintyre and the Islands) -

THE DEMOGRAPHY of SCOTLAND and the IMPLICATIONS for DEVOLUTION — EVIDENCE from POPULATION Mattersi
THE DEMOGRAPHY OF SCOTLAND AND THE IMPLICATIONS FOR DEVOLUTION — EVIDENCE FROM POPULATION MATTERSi Key Points • Scotland’s population is growing, but more slowly and ageing more quickly than the remainder of the United Kingdom. • Scotland has lower fertility than the remainder of the United Kingdom. • Both the United Kingdom and Scottish populations are consuming ecological resources at an unsustainable rate. • The focus should be on managing the transition to a sustainable, stable population with a different demographic profile, not on trying artificially to maintain an existing demographic profile. • Responses to demographic change require long-term policies and plans. • Population must be given more attention in government through the appointment of senior ministers who have responsibility for this across departments. • Policies to encourage more efficient use of the existing labour pool and to reduce unintended pregnancies should be introduced. • The Scottish Government has significant policy levers; however, the devolving of powers over employment should be considered because of the differing nature of the demographic challenges in Scotland and the remainder of the United Kingdom. Reasons for Revision A first version of this evidence paper was submitted to the Scottish Affairs Committee in February 2016. Since this time, new population data for Scotland and the UK has become available, and the UK has voted in a national referendum to leave the European Union. In light of these recent developments, Population Matters has decided that it is appropriate that we revise our evidence report, including the most recent data, and the impact that the EU referendum result is likely to have on Scottish and UK demographics. -

Historic Arts and Crafts House with Separate Cottage and Views Over the Gare Loch
Historic Arts and Crafts house with separate cottage and views over the Gare Loch Ferry Inn, Rosneath, By Helensburgh, G84 0RS Lower ground floor: Sitting room, bedroom/gym, WC. Ground floor: Reception hall, drawing room, dining room, kitchen, study, morning room, pantry First floor: Principal bedroom with en suite bathroom, 3 further bedrooms, 2 further bathrooms. Ferry Inn Cottage: Detached cottage with living room/bedroom/bedroom, kitchen and shower room Garden & Grounds of around 4 acres. Local Information and both local authority and Ferry Inn is set in around 4 acres private schools. of its own grounds on the Rosneath Peninsula. The grounds The accessibility of the Rosneath form the corner of the promontory Peninsula has been greatly on the edge of Rosneath which improved by the opening of the juts out into the sea loch. There new Ministry of Defence road are magnificent views from the over the hills to Loch Lomond. house over the loch and to the The journey time to Loch marina at Rhu on the opposite. Lomond, the Erskine Bridge and Glasgow Airport has been The Rosneath Peninsula lies to significantly reduced by the new the north of the Firth of Clyde. road which bypasses Shandon, The peninsula is reached by the Rhu and Helensburgh on the road from Garelochhead in its A814 on the other side of the neck to the north. The peninsula loch. is bounded by Loch Long to the northwest, Gare Loch to the east About this property and the Firth of Clyde to the south The original Ferry Inn stood next and is connected to the mainland to the main jetty for the ferry by a narrow isthmus at its which ran between Rosneath and northern end. -
Guide to Services Links and Resources for Health and Wellbeing
Guide to Services Links and Resources for Health and Wellbeing 2! ! ! ! ! Health!is!a!state!of! complete!physical,! mental!and!social! wellbeing!and!not! merely!the!absence! of!disease!or! infirmity! ! ! ! (World'Health'Organisation)' ! ! ! ! 3! Guide to Services Links and Resources For Health & Wellbeing Contents ! Introduction - Keeping Well 4 - 7 Emergency and Crisis Contacts 8 - 19 Who’s Who in the Community Mental Health Service 20 - 28 'Self Help Resources and Websites 29 - 42 Local Services and Agencies 43 - 68 List of Local Directories 69 - 73 Information on Local Groups and Activities 74 - 86 Index 87 - 94 Survey This is for You - Relaxation CD 4! 1. Eat a balanced diet and drink sensibly: Improving your diet can protect against feelings of anxiety and depression. 2. Maintain friendships: Just listening and talking to friends who are feeling down can make a huge difference. So make sure your devote time to maintaining your friendships both for their sake and your own. 3. Maintain close relationships: Close relationships affect how we feel - so nurture them and if there is a problem within a relationship, try and resolve it. 4. Take exercise: The effects of exercise on mood are immediate. Whether it is a workout in the gym or a simple walk or bike ride, it can be uplifting. Exercise can also be great fun socially. 5. Sleep: Sleep has both physical and mental benefits. Physically it is the time when the body can renew its energy store but sleep also helps us to rebuild our mental energy. 6. Laugh: A good laugh does wonders for the mind and soul. -

BCS Paper 2017/74 2018 Review of UK Parliament Constituencies Draft
Boundary Commission for Scotland BCS Paper 2017/74 2018 Review of UK Parliament Constituencies Draft Revised Proposals for Argyll and Bute, Highland and Moray council areas Action required 1. The Commission is invited to consider responses to the initial and secondary consultation on its Initial Proposals and whether it wishes to make changes to its proposals for Argyll and Bute, Highland and Moray council areas. Background 2. These constituency designs are based on a UK electoral quota of 74,769.2 electors and parliamentary electorate figures from the December 2015 Electoral Register. The electorate of constituencies has to be within 5% of the electoral quota, namely no fewer than 71,031 and no more than 78,507, unless the area of a constituency exceeds 12,000 square kilometres. No constituency may exceed 13,000 square kilometres. 3. The total electorate in the 3 council areas is 307,418, giving a theoretical entitlement to 4.11 constituencies. It is possible, therefore, to design 4 constituencies, exactly covering the combined council areas, the electorates of which are within the limits set by the legislation. 4. The Commission's Initial Proposals for this area comprise 4 constituencies which exactly cover the combined extent of these 3 council areas. A map of the constituencies is at Appendix A. Wards Difference Constituency Council areas Area (km2) Electorate (2007–2017) from EQ Argyll, Bute and Argyll and Bute All 10,302 77,574 3.8% Lochaber Highland 12(part),22 Highland Highland 1-5,6(part),7-10,13(part) 12,985 73,147 -2.2% North Inverness 6(part),11,12(part),13(part),14- Highland 9,995 78,220 4.6% and Skye 18,20,21 Moray Moray All 2,612 78,477 5.0% and Nairn Highland 19 Table 1. -

Argyll and Bute Council Council Legal and Regulatory Support 24 June 2021 Boundaries Scotland
ARGYLL AND BUTE COUNCIL COUNCIL LEGAL AND REGULATORY SUPPORT 24 JUNE 2021 BOUNDARIES SCOTLAND - REVIEW OF ELECTORAL ARRANGEMENTS 1. EXECUTIVE SUMMARY 1.1 A report was submitted to the Council meeting held on 24 September 2020, detailing the terms of a proposed response to Boundaries Scotland’s initial consultation, which ran for a 2 month period from 16th July to 30th September 2020, in regard to the 2019 Review of Electoral Arrangements for Argyll and Bute Council area. The Council agreed the response and this was submitted in accordance with the 30th September 2020 deadline. 1.2 Following the initial consultation with the Council, Boundaries Scotland considered our response and developed proposals for public consultation, which ran for a 12 week period between November 2020 and January 2021. 1.3 Having considered all the comments submitted as part of the public consultation, Boundaries Scotland have now published their final proposals for Argyll and Bute Council area and a copy of the report to Scottish Ministers is attached at appendix 1. If Scottish Ministers are content with the report, it is anticipated that the proposals will be implemented ready for the Local Government elections in May 2022. 1.4 In line with section 18(3) of the Local Government (Scotland) Act 1973 the Council will make copies of the report available for public inspection at suitable locations and will be publicised on the Council website from 10 June 2021 until 6 months after the making of an Order in the Scottish Parliament giving effect to any proposals in the report. 2. -
Battrum's Guide and Directory to Helensburgh and Neighbourhood
ii t^^ =»». fl,\l)\ National Library of Scotland ^6000261860' Digitized by tine Internet Arciiive in 2010 with funding from National Library of Scotland http://www.archive.org/details/battrumsguidedir1875batt u : MACNEUR & BRYDEN'S (31.-A.TE ""w. :b.aji}t:rtji^'&] GUIDE AND DIRECTORY TO HELENSBURGH AND NEIGHBOURHOOD, SEVENTH EDITIOK. ;^<A0MSjdi^ HELENSBUEGH MACNEUE & BUT & 52 East Princes Street, aad 19 West Clyde Street, 1875. 7. PREFACE. In issning the seventh edition of the Helensburgh Direc- tory, the publishers, remembering the kind apprecia- tion it received when published by the late Mr Battrum, trust that it will meet with a similar reception. Although imperfect in many respects, considerabie care has been expended in its compiling. It is now larger than anj^ previous issue, and the publishers doubt not it will be found useful as a book of reference in this daily increasing district. The map this year has been improved, showing the new feus, houses, and streets that have been made ; and, altogether, every effort has been made to render tbe Directory worthy of the town and neighbourhood. September' 1875. NAMES OF THE NEW POLICE COMMISSIONERS, Steveu, Mag. Wilhaiii Bryson. Thomas Chief j J. W. M'Culloch, Jun. Mag. John Crauib. John Stuart, Jun. Mag. Donald Murray. Einlay Campbell. John Dingwall, Alexander Breingan. B. S. MFarlane. Andrew Provan. Martin M' Kay. Towii-CJerk—Geo, Maclachlan. Treasurer—K. D, Orr. Macneur & Bkyden (successors to the late W. Battrum), House Factors and Accountants. House Register published as formerly. CONTENTS OF GUIDE. HELENSBURGH— page ITS ORIGIN, ..,.,..., 9 OLD RECORDS, H PROVOSTS, 14 CHURCHES, 22 BANKS, 26 TOWN HALL, . -

Argyll and Bute Council
APPENDIX 1 PROPOSED KILPATRICK HILLS LOCAL LANDSCAPE AREA – DRAFT STATEMENT OF IMPORTANCE September 2013 Contents 1. Introduction 2. Policy context 3. Background and study approach 4. Statement of Importance 4.1 Overview 4.2 Landscape Description 4.3 Proposed Local Landscape Area boundary 4.4 Landscape change 4.5 Other designations and interests 1. INTRODUCTION The Kilpatrick Hills are a range of hills north of the River Clyde stretching from Dumbarton and the Vale of Leven in the west to Strathblane in the east. The rugged upland landscape provides a stunning backdrop to the settlements which fringe them, including Balloch, Dumbarton, Bowling, Old Kilpatrick, Clydebank, Bearsden and Milngavie, creating a unique sense of place. To the north of the hills lies the Loch Lomond and the Trossachs National Park. The majority of the range is within West Dunbartonshire, although it extends into East Dunbartonshire and Stirling. In addition to the Kilpatrick Hills’ special landscape qualities, the area is home to an important habitat network and provides recreational opportunities for local communities. West Dunbartonshire Council and East Dunbartonshire Council propose to designate the Kilpatrick Hills as a Local Landscape Area (LLA) in their respective Local Development Plans. This document explains the reasons why the Kilpatrick Hills have been selected for this designation. It will provide the basis for Supplementary Guidance for the Kilpatrick Hills which will establish a framework for managing change and the protection and enhancement of the area’s special qualities. Figure 1 – The location of the Kilpatrick Hills within central Scotland 2 2. POLICY CONTEXT Scotland’s landscapes are recognised as a major asset, contributing to national, regional and local identities, adding to the quality of many people’s lives and providing attractive settings which help to promote social and economic development. -

Electoral Review of Island Council Areas
Agenda 14 Item Report HC/18/19 No The Highland Council Date: 9 May, 2019 Report title: Electoral Review of Island Council Areas Report by: The Chief Executive Purpose/Executive Summary The purpose of this report is to provide the Council with an overview of the provisions of the Islands (Scotland) Act 2018 that relate to the requirement for the Local Government Boundary Commission for Scotland to review the electoral arrangements for Argyll and Bute Council, Comhairle Nan Eilean Siar, Highland Council, North Ayrshire Council, Orkney Islands Council and Shetland Islands Council. 1. Recommendations 1.1 Council is invited to • Agree that the Chief Executive write to the Local Government Boundary Commission seeking a meeting to explore the possibility of the Commission broadening the scope of their current review to include rural wards of super sparsity. • Agree that the Council write to the Cabinet Secretary for Communities and Local Government to highlight issues around the methodology used in boundary reviews and to make the case for additional flexibility over the number of members for rural wards. 2. Background 2.1 The Local Government Boundary Commission for Scotland and the Scottish Ministers are obliged, under section 28(2) of the Local Government (Scotland) Act 1973 to implement electoral arrangements in accordance with section 1 of the Local Governance (Scotland) Act 2004. Currently this includes the requirement for there to be three or four councillors returned per electoral ward in Scotland. 2.2 The Islands (Scotland) Act 2018 amends the 2004 Act to provide an exception to the usual three or four member rule for electoral wards in relation to wards which consist either wholly or partly of one or more inhabited islands.