Biallelic Truncating FANCM Mutations Cause Early-Onset Cancer but Not Fanconi Anemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Structure and Function of the Human Recq DNA Helicases
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2005 Structure and function of the human RecQ DNA helicases Garcia, P L Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-34420 Dissertation Published Version Originally published at: Garcia, P L. Structure and function of the human RecQ DNA helicases. 2005, University of Zurich, Faculty of Science. Structure and Function of the Human RecQ DNA Helicases Dissertation zur Erlangung der naturwissenschaftlichen Doktorw¨urde (Dr. sc. nat.) vorgelegt der Mathematisch-naturwissenschaftlichen Fakultat¨ der Universitat¨ Z ¨urich von Patrick L. Garcia aus Unterseen BE Promotionskomitee Prof. Dr. Josef Jiricny (Vorsitz) Prof. Dr. Ulrich H ¨ubscher Dr. Pavel Janscak (Leitung der Dissertation) Z ¨urich, 2005 For my parents ii Summary The RecQ DNA helicases are highly conserved from bacteria to man and are required for the maintenance of genomic stability. All unicellular organisms contain a single RecQ helicase, whereas the number of RecQ homologues in higher organisms can vary. Mu- tations in the genes encoding three of the five human members of the RecQ family give rise to autosomal recessive disorders called Bloom syndrome, Werner syndrome and Rothmund-Thomson syndrome. These diseases manifest commonly with genomic in- stability and a high predisposition to cancer. However, the genetic alterations vary as well as the types of tumours in these syndromes. Furthermore, distinct clinical features are observed, like short stature and immunodeficiency in Bloom syndrome patients or premature ageing in Werner Syndrome patients. Also, the biochemical features of the human RecQ-like DNA helicases are diverse, pointing to different roles in the mainte- nance of genomic stability. -
Fanconi Anemia: Guidelines for Diagnosis and Management
Fanconi Anemia: Guidelines for Diagnosis and Management Fourth Edition • 2014 We are deeply grateful to the following generous donors, who made this publication possible: Pat and Stephanie Kilkenny Phil and Penny Knight Disclaimer Information provided in this handbook about medications, treatments or products should not be construed as medical instruction or scientific endorsement. Always consult your physician before taking any action based on this information. copyright© 1999; second edition 2003; third edition 2008; fourth edition 2014 Fanconi Anemia: Guidelines for Diagnosis and Management Fourth Edition • 2014 Managing Editor: Laura Hays, PhD Editors: Dave Frohnmayer, JD, Lynn Frohnmayer, MSW, Eva Guinan, MD, Teresa Kennedy, MA, and Kim Larsen Scientific Writers: SciScripter, LLC These guidelines for the clinical care of Fanconi anemia (FA) were developed at a conference held April 5-6, 2013 in Herndon, VA. We owe a tremendous debt of gratitude to Eva Guinan, MD, for serving as moderator of the conference, as she did for the consensus conferences for the first three editions, and for her skill in helping the participants arrive at consensus. We would like to thank all the participants for donating their time and expertise to develop these guidelines. The names and contact information of all participants appear in the Appendix. These guidelines are posted on our Web site and are available from: Fanconi Anemia Research Fund, Inc. Phone: 541-687-4658 or 888-326-2664 (US only) 1801 Willamette Street, Suite 200 FAX: 541-687-0548 Eugene, Oregon 97401 E-mail: [email protected] Web site: www.fanconi.org Facebook: www.facebook.com/fanconianemiaresearchfund Twitter: https://twitter.com/FAresearchfund Material from this book may be reprinted with the permission of the Fanconi Anemia Research Fund, Inc. -

Regulation of DNA Cross-Link Repair by the Fanconi Anemia/BRCA Pathway
Downloaded from genesdev.cshlp.org on September 29, 2021 - Published by Cold Spring Harbor Laboratory Press REVIEW Regulation of DNA cross-link repair by the Fanconi anemia/BRCA pathway Hyungjin Kim and Alan D. D’Andrea1 Department of Radiation Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, Massachusetts 02215, USA The maintenance of genome stability is critical for sur- and quadradials, a phenotype widely used as a diagnostic vival, and its failure is often associated with tumorigen- test for FA. esis. The Fanconi anemia (FA) pathway is essential for At least 15 FA gene products constitute a common the repair of DNA interstrand cross-links (ICLs), and a DNA repair pathway, the FA pathway, which resolves germline defect in the pathway results in FA, a cancer ICLs encountered during replication (Fig. 1A). Specifi- predisposition syndrome driven by genome instability. cally, eight FA proteins (FANCA/B/C/E/F/G/L/M) form Central to this pathway is the monoubiquitination of a multisubunit ubiquitin E3 ligase complex, the FA core FANCD2, which coordinates multiple DNA repair activ- complex, which activates the monoubiquitination of ities required for the resolution of ICLs. Recent studies FANCD2 and FANCI after genotoxic stress or in S phase have demonstrated how the FA pathway coordinates three (Wang 2007). The FANCM subunit initiates the pathway critical DNA repair processes, including nucleolytic in- (Fig. 1B). It forms a heterodimeric complex with FAAP24 cision, translesion DNA synthesis (TLS), and homologous (FA-associated protein 24 kDa), and the complex resem- recombination (HR). Here, we review recent advances in bles an XPF–ERCC1 structure-specific endonuclease pair our understanding of the downstream ICL repair steps (Ciccia et al. -

Open Full Page
CCR PEDIATRIC ONCOLOGY SERIES CCR Pediatric Oncology Series Recommendations for Childhood Cancer Screening and Surveillance in DNA Repair Disorders Michael F. Walsh1, Vivian Y. Chang2, Wendy K. Kohlmann3, Hamish S. Scott4, Christopher Cunniff5, Franck Bourdeaut6, Jan J. Molenaar7, Christopher C. Porter8, John T. Sandlund9, Sharon E. Plon10, Lisa L. Wang10, and Sharon A. Savage11 Abstract DNA repair syndromes are heterogeneous disorders caused by around the world to discuss and develop cancer surveillance pathogenic variants in genes encoding proteins key in DNA guidelines for children with cancer-prone disorders. Herein, replication and/or the cellular response to DNA damage. The we focus on the more common of the rare DNA repair dis- majority of these syndromes are inherited in an autosomal- orders: ataxia telangiectasia, Bloom syndrome, Fanconi ane- recessive manner, but autosomal-dominant and X-linked reces- mia, dyskeratosis congenita, Nijmegen breakage syndrome, sive disorders also exist. The clinical features of patients with DNA Rothmund–Thomson syndrome, and Xeroderma pigmento- repair syndromes are highly varied and dependent on the under- sum. Dedicated syndrome registries and a combination of lying genetic cause. Notably, all patients have elevated risks of basic science and clinical research have led to important in- syndrome-associated cancers, and many of these cancers present sights into the underlying biology of these disorders. Given the in childhood. Although it is clear that the risk of cancer is rarity of these disorders, it is recommended that centralized increased, there are limited data defining the true incidence of centers of excellence be involved directly or through consulta- cancer and almost no evidence-based approaches to cancer tion in caring for patients with heritable DNA repair syn- surveillance in patients with DNA repair disorders. -

The Role of SLX4 and Its Associated Nucleases in DNA Interstrand Crosslink Repair Wouter S
Nucleic Acids Research, 2018 1 doi: 10.1093/nar/gky1276 The role of SLX4 and its associated nucleases in DNA interstrand crosslink repair Wouter S. Hoogenboom, Rick A.C.M. Boonen and Puck Knipscheer* Downloaded from https://academic.oup.com/nar/advance-article-abstract/doi/10.1093/nar/gky1276/5255686 by guest on 28 December 2018 Oncode Institute, Hubrecht Institute–KNAW and University Medical Center Utrecht, Utrecht, The Netherlands Received May 17, 2018; Revised December 11, 2018; Editorial Decision December 12, 2018; Accepted December 13, 2018 ABSTRACT the cancer predisposition syndrome Fanconi anemia (FA) that is caused by biallelic mutations in any one of the 22 A key step in the Fanconi anemia pathway of DNA currently known FA genes. Cells from FA patients are re- interstrand crosslink (ICL) repair is the ICL unhook- markably sensitive to ICL inducing agents, consistent with ing by dual endonucleolytic incisions. SLX4/FANCP the FA proteins being involved in the repair of DNA inter- is a large scaffold protein that plays a central role strand crosslinks (6,7). Indeed, it has been shown that ex- in ICL unhooking. It contains multiple domains that ogenous ICLs, for example caused by cisplatin, are repaired interact with many proteins including three different by the FA pathway (8). Although the source of the endoge- endonucleases and also acts in several other DNA nous ICL that requires the FA pathway for its repair is cur- repair pathways. While it is known that its interaction rently not known, genetic evidence points towards reactive with the endonuclease XPF-ERCC1 is required for its aldehydes (9–13). -

Review of Cancer Genetics
Review of Cancer Genetics Genes are pieces of information in the cells that make up the body. Cells are the basic units of life. Normally, cells grow, divide and make more cells in a controlled way as the body needs them to stay healthy. Cancer happens when a cell grows out of control in an abnormal way. All cancer is caused by a buildup of mutations (changes) in specific genes. Normally, these genes help the cell grow and divide in a controlled manner. The mutation in the gene damages this process and, as a result, the cell can grow out of control and become cancer. In most people who have cancer, the gene mutations that lead to their cancer cannot be passed on to their children. However, some families have a gene mutation that can get passed on from one generation to another. The differences between sporadic (non-hereditary) and hereditary forms of cancer are reviewed below. Additionally, some families have more cancer than would be expected by chance, but the cancer does not seem to be hereditary. This “familial” form of cancer is also discussed below. Sporadic Cancer Most cancer – 75% to 80% – is sporadic. In sporadic cancer, the gene mutations that cause the cancer are acquired (occur only in the tumor cells) and are not inherited. Risk for acquired gene mutations increases with age and is often influenced by environmental, lifestyle or medical factors. Cancer can sometimes happen by chance. Everyone has some risk of developing cancer in his or her lifetime. Because cancer is common, it is possible for a family to have more than one member who has cancer by chance. -

Hereditary Breast and Ovarian Cancer Syndrome
Page 1 of 4 Hereditary Breast and Ovarian Cancer Syndrome Hereditary breast and/or ovarian cancer (HBOC) is an autosomal dominant cancer susceptibility syndrome, most commonly associated with an inherited BRCA1 or BRCA2 gene mutation. Approximately 1 in 300 to 1 in 400 people in the general population are born with an inherited mutation in either the BRCA1 or BRCA2 genes. The frequency of BRCA1 or BRCA2 gene mutations is approximately 1 in 40 for people with Ashkenazi Jewish heritage. Other high-risk genes associated with hereditary breast and/or ovarian cancers include: PALB2, TP53, PTEN, STK11, CDH1. Additional genes may also be discussed in the context of Hereditary Cancer Program assessment. Confirmation of HBOC is important both for people with cancer, because of the associated risk for another cancer, and to inform appropriate cancer risk management for their adult family members. Note to oncologists/GPOs: if your regular practice includes women who are eligible for BRCA1/BRCA2 testing, we offer training to prepare you to initiate genetic testing for patients whose personal history meets specific criteria. Please contact the Hereditary Cancer Program’s Clinical Coordinator (604-877- 6000 local 672198) if you are interested in this oncology clinic based genetic testing (GENONC) process. Referral Criteria Notes: 1. breast cancer includes DCIS (ductal carcinoma in situ) and excludes LCIS (lobular carcinoma in situ) 2. ovarian cancer refers to invasive non-mucinous epithelial ovarian cancer; includes cancer of the fallopian tubes, primary peritoneal cancer and STIC (serous tubal intraepithelial carcinoma); excludes borderline/LMP ovarian tumours 3. close relatives include: children, brothers, sisters, parents, aunts, uncles, grandchildren & grandparents on the same side of the family. -
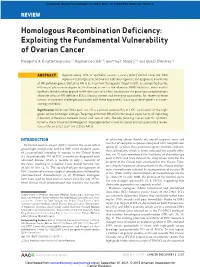
Homologous Recombination Deficiency: Exploiting the Fundamental Vulnerability of Ovarian Cancer
Published OnlineFirst October 13, 2015; DOI: 10.1158/2159-8290.CD-15-0714 Review Homologous Recombination Deficiency: Exploiting the Fundamental Vulnerability of Ovarian Cancer Panagiotis A. Konstantinopoulos1,2, Raphael Ceccaldi2,3, Geoffrey I. Shapiro2,4, and Alan D. D’Andrea2,3 AbstAt R c Approximately 50% of epithelial ovarian cancers (EOC) exhibit defective DNA repair via homologous recombination (HR) due to genetic and epigenetic alterations of HR pathway genes. Defective HR is an important therapeutic target in EOC as exemplified by the efficacy of platinum analogues in this disease, as well as the advent of PARP inhibitors, which exhibit synthetic lethality when applied to HR-deficient cells. Here, we describe the genotypic and phenotypic characteristics of HR-deficient EOCs, discuss current and emerging approaches for targeting these tumors, and present challenges associated with these approaches, focusing on development and over- coming resistance. Significance: Defective DNA repair via HR is a pivotal vulnerability of EOC, particularly of the high- grade serous histologic subtype. Targeting defective HR offers the unique opportunity of exploiting molecular differences between tumor and normal cells, thereby inducing cancer-specific synthetic lethality; the promise and challenges of these approaches in ovarian cancer are discussed in this review. Cancer Discov; 5(11); 1137–54. ©2015 AACR. iNtRODUctiON of achieving almost double the overall response rates and number of complete responses compared with nonplatinum Epithelial ovarian cancer (EOC) remains the most lethal agents (5, 6). Since then, platinum agents (initially cisplatin, gynecologic malignancy and the fifth most frequent cause then carboplatin, which is better tolerated but equally effec- of cancer-related mortality in women in the United States tive; ref. -

Role of Deubiquitinating Enzymes in DNA Repair Younghoon Kee University of South Florida, [email protected]
University of South Florida Scholar Commons Cell Biology, Microbiology, and Molecular Biology Cell Biology, Microbiology, and Molecular Biology Faculty Publications 2-15-2016 Role of Deubiquitinating Enzymes in DNA Repair Younghoon Kee University of South Florida, [email protected] Tony T. Huang New York University School of Medicine Follow this and additional works at: http://scholarcommons.usf.edu/bcm_facpub Part of the Biology Commons, and the Cell and Developmental Biology Commons Scholar Commons Citation Kee, Younghoon and Huang, Tony T., "Role of Deubiquitinating Enzymes in DNA Repair" (2016). Cell Biology, Microbiology, and Molecular Biology Faculty Publications. 30. http://scholarcommons.usf.edu/bcm_facpub/30 This Article is brought to you for free and open access by the Cell Biology, Microbiology, and Molecular Biology at Scholar Commons. It has been accepted for inclusion in Cell Biology, Microbiology, and Molecular Biology Faculty Publications by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. crossmark MINIREVIEW Role of Deubiquitinating Enzymes in DNA Repair Younghoon Kee,a Tony T Huangb Department of Cell Biology, Microbiology, and Molecular Biology, College of Arts and Sciences, University of South Florida, Tampa, Florida, USAa; Department of Biochemistry and Molecular Pharmacology, New York University School of Medicine, New York, New York, USAb Both proteolytic and nonproteolytic functions of ubiquitination are essential regulatory mechanisms for promoting DNA repair and the DNA damage response in mammalian cells. Deubiquitinating enzymes (DUBs) have emerged as key players in the main- tenance of genome stability. In this minireview, we discuss the recent findings on human DUBs that participate in genome main- tenance, with a focus on the role of DUBs in the modulation of DNA repair and DNA damage signaling. -
FANCJ Regulates the Stability of FANCD2/FANCI Proteins and Protects Them from Proteasome and Caspase-3 Dependent Degradation
FANCJ regulates the stability of FANCD2/FANCI proteins and protects them from proteasome and caspase-3 dependent degradation Komaraiah Palle, Ph.D. (Kumar) Assistant Professor of Oncologic Sciences Abraham Mitchell Cancer Research Scholar Mitchell Cancer Institute University of South Alabama Outline • Fanconi anemia (FA) pathway • Role of FA pathway in Genome maintenance • FANCJ and FANCD2 functional relationship • FANCJ-mediated DDR in response to Fork-stalling Fanconi Anemia • Rare, inherited blood disorder. • 1:130,000 births Guido Fanconi 1892-1979 • Affects men and women equally. • Affects all racial and ethnic groups – higher incidence in Ashkenazi Jews and Afrikaners Birth Defects Fanconi anemia pathway • FA is a rare chromosome instability syndrome • Autosomal recessive disorder (or X-linked) • Developmental abnormalities • 17 complementation groups identified to date • FA pathway is involved in DNA repair • Increased cancer susceptibility - many patients develop AML - in adults solid tumors Fanconi Anemia is an aplastic anemia FA patients are prone to multiple types of solid tumors • Increased incidence and earlier onset cancers: oral cavity, GI and genital and reproductive tract head and neck breast esophagus skin liver brain Why? FA is a DNA repair disorder • FA caused by mutations in 17 genes: FANCA FANCF FANCM FANCB FANCG/XRCC9 FANCN/PALB2 FANCC FANCI RAD51C/FANCO FANCD1/BRCA2 FANCJ SLX4/FANCP FANCD2 FANCL ERCC2/XPF/FANCQ FANCE BRCA1/FANCS • FA genes function in DNA repair processes • FA patient cells are highly sensitive -

Fanconi Anemia, Bloom Syndrome and Breast Cancer
A multiprotein complex in DNA damage response network of Fanconi anemia, Bloom syndrome and Breast cancer Weidong Wang Lab of Genetics, NIA A Multi-protein Complex Connects Two Genomic Instability Diseases: Bloom Syndrome and Fanconi Anemia Bloom Syndrome . Genomic Instability: -sister-chromatid exchange . Cancer predisposition . Mutation in BLM, a RecQ DNA Helicase . BLM participates in: HR-dependent DSB repair Recovery of stalled replication forks . BLM works with Topo IIIa and RMI to Suppress crossover recombination Courtesy of Dr. Ian Hickson A Multi-protein Complex Connects Two Genomic Instability Diseases: Bloom Syndrome and Fanconi Anemia P I l o r t n o BLM IP kDa C HeLa BLAP 250 Nuclear Extract 200- BLM* FANCA* 116- TOPO IIIα* 97- BLAP 100 MLH1* BLM IP BLAP 75 * 66- RPA 70 IgG H 45- * 30- RPA32 IgG L 20- * 12- RPA14 Meetei et al. MCB 2003 A Multi-protein Complex Connects Two Genomic Instability Diseases: Bloom Syndrome and Fanconi Anemia P I A C N A F BLM IP HeLa FANCM= FAAP 250 BLAP 250 Nuclear Extract BLM* BLM* * FANCA* FANCA TOPO IIIα* TOPO IIIα* FAAP 100 BLAP 100 FANCB= FAAP 95 MLH1 FANCA IP BLM IP BLAP 75 BLAP 75 RPA70*/FANCG* RPA 70* FANCC*/FANCE* IgG H FANCL= FAAP 43 FANCF* RPA32* IgG L Meetei et al. MCB 2003 Meetei et al. Nat Genet. 2003, 2004, 2005 BRAFT-a Multisubunit Machine that Maintains Genome Stability and is defective in Fanconi anemia and Bloom syndrome BRAFT Super-complex Fanconi Anemia Bloom Syndrome Core Complex Complex 12 polypeptides 7 polypeptides FANCA BLM Helicase (HJ, fork, D-loop), fork FANCC regression, dHJ dissolution Topo IIIα Topoisomerase, FANCE dHJ dissolution FANCF BLAP75 RMI1 FANCG Stimulates dHJ dissolution. -

HEREDITARY CANCER PANELS Part I
Pathology and Laboratory Medicine Clinic Building, K6, Core Lab, E-655 2799 W. Grand Blvd. HEREDITARY CANCER PANELS Detroit, MI 48202 855.916.4DNA (4362) Part I- REQUISITION Required Patient Information Ordering Physician Information Name: _________________________________________________ Gender: M F Name: _____________________________________________________________ MRN: _________________________ DOB: _______MM / _______DD / _______YYYY Address: ___________________________________________________________ ICD10 Code(s): _________________/_________________/_________________ City: _______________________________ State: ________ Zip: __________ ICD-10 Codes are required for billing. When ordering tests for which reimbursement will be sought, order only those tests that are medically necessary for the diagnosis and treatment of the patient. Phone: _________________________ Fax: ___________________________ Billing & Collection Information NPI: _____________________________________ Patient Demographic/Billing/Insurance Form is required to be submitted with this form. Most genetic testing requires insurance prior authorization. Due to high insurance deductibles and member policy benefits, patients may elect to self-pay. Call for more information (855.916.4362) Bill Client or Institution Client Name: ______________________________________________________ Client Code/Number: _____________ Bill Insurance Prior authorization or reference number: __________________________________________ Patient Self-Pay Call for pricing and payment options Toll