Deakin Research Online
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Taylors Hill-Werribee South Sunbury-Gisborne Hurstbridge-Lilydale Wandin East-Cockatoo Pakenham-Mornington South West
TAYLORS HILL-WERRIBEE SOUTH SUNBURY-GISBORNE HURSTBRIDGE-LILYDALE WANDIN EAST-COCKATOO PAKENHAM-MORNINGTON SOUTH WEST Metro/Country Postcode Suburb Metro 3200 Frankston North Metro 3201 Carrum Downs Metro 3202 Heatherton Metro 3204 Bentleigh, McKinnon, Ormond Metro 3205 South Melbourne Metro 3206 Albert Park, Middle Park Metro 3207 Port Melbourne Country 3211 LiQle River Country 3212 Avalon, Lara, Point Wilson Country 3214 Corio, Norlane, North Shore Country 3215 Bell Park, Bell Post Hill, Drumcondra, Hamlyn Heights, North Geelong, Rippleside Country 3216 Belmont, Freshwater Creek, Grovedale, Highton, Marhsall, Mt Dunede, Wandana Heights, Waurn Ponds Country 3217 Deakin University - Geelong Country 3218 Geelong West, Herne Hill, Manifold Heights Country 3219 Breakwater, East Geelong, Newcomb, St Albans Park, Thomson, Whington Country 3220 Geelong, Newtown, South Geelong Anakie, Barrabool, Batesford, Bellarine, Ceres, Fyansford, Geelong MC, Gnarwarry, Grey River, KenneQ River, Lovely Banks, Moolap, Moorabool, Murgheboluc, Seperaon Creek, Country 3221 Staughtonvale, Stone Haven, Sugarloaf, Wallington, Wongarra, Wye River Country 3222 Clilon Springs, Curlewis, Drysdale, Mannerim, Marcus Hill Country 3223 Indented Head, Port Arlington, St Leonards Country 3224 Leopold Country 3225 Point Lonsdale, Queenscliffe, Swan Bay, Swan Island Country 3226 Ocean Grove Country 3227 Barwon Heads, Breamlea, Connewarre Country 3228 Bellbrae, Bells Beach, jan Juc, Torquay Country 3230 Anglesea Country 3231 Airleys Inlet, Big Hill, Eastern View, Fairhaven, Moggs -

Town and Country Planning Board of Victoria
1965-66 VICTORIA TWENTIETH ANNUAL REPORT OF THE TOWN AND COUNTRY PLANNING BOARD OF VICTORIA FOR THE PERIOD lsr JULY, 1964, TO 30rH JUNE, 1965 PRESENTED TO BOTH HOUSES OF PARLIAMENT PURSUANT TO SECTION 5 (2) OF THE TOWN AND COUNTRY PLANNING ACT 1961 [Appro:timate Cost of Report-Preparation, not given. Printing (225 copies), $736.00 By Authority A. C. BROOKS. GOVERNMENT PRINTER. MELBOURNE. No. 31.-[25 cents]-11377 /65. INDEX PAGE The Board s Regulations s Planning Schemes Examined by the Board 6 Hazelwood Joint Planning Scheme 7 City of Ringwood Planning Scheme 7 City of Maryborough Planning Scheme .. 8 Borough of Port Fairy Planning Scheme 8 Shire of Corio Planning Scheme-Lara Township Nos. 1 and 2 8 Shire of Sherbrooke Planning Scheme-Shire of Knox Planning Scheme 9 Eildon Reservoir .. 10 Eildon Reservoir Planning Scheme (Shire of Alexandra) 10 Eildon Reservoir Planning Scheme (Shire of Mansfield) 10 Eildon Sub-regional Planning Scheme, Extension A, 1963 11 Eppalock Planning Scheme 11 French Island Planning Scheme 12 Lake Bellfield Planning Scheme 13 Lake Buffalo Planning Scheme 13 Lake Glenmaggie Planning Scheme 14 Latrobe Valley Sub-regional Planning Scheme 1949, Extension A, 1964 15 Phillip Island Planning Scheme 15 Tower Hill Planning Scheme 16 Waratah Bay Planning Scheme 16 Planning Control for Victoria's Coastline 16 Lake Tyers to Cape Howe Coastal Planning Scheme 17 South-Western Coastal Planning Scheme (Shire of Portland) 18 South-Western Coastal Planning Scheme (Shire of Belfast) 18 South-Western Coastal Planning Scheme (Shire of Warrnambool) 18 South-Western Coastal Planning Scheme (Shire of Heytesbury) 18 South-Western Coastal Planning Scheme (Shire of Otway) 18 Wonthaggi Coastal Planning Scheme (Borough of Wonthaggi) 18 Melbourne Metropolitan Planning Scheme 19 Melbourne's Boulevards 20 Planning Control Around Victoria's Reservoirs 21 Uniform Building Regulations 21 INDEX-continued. -

List of Parishes in the State of Victoria
List of Parishes in the State of Victoria Showing the County, the Land District, and the Municipality in which each is situated. (extracted from Township and Parish Guide, Department of Crown Lands and Survey, 1955) Parish County Land District Municipality (Shire Unless Otherwise Stated) Acheron Anglesey Alexandra Alexandra Addington Talbot Ballaarat Ballaarat Adjie Benambra Beechworth Upper Murray Adzar Villiers Hamilton Mount Rouse Aire Polwarth Geelong Otway Albacutya Karkarooc; Mallee Dimboola Weeah Alberton East Buln Buln Melbourne Alberton Alberton West Buln Buln Melbourne Alberton Alexandra Anglesey Alexandra Alexandra Allambee East Buln Buln Melbourne Korumburra, Narracan, Woorayl Amherst Talbot St. Arnaud Talbot, Tullaroop Amphitheatre Gladstone; Ararat Lexton Kara Kara; Ripon Anakie Grant Geelong Corio Angahook Polwarth Geelong Corio Angora Dargo Omeo Omeo Annuello Karkarooc Mallee Swan Hill Annya Normanby Hamilton Portland Arapiles Lowan Horsham (P.M.) Arapiles Ararat Borung; Ararat Ararat (City); Ararat, Stawell Ripon Arcadia Moira Benalla Euroa, Goulburn, Shepparton Archdale Gladstone St. Arnaud Bet Bet Ardno Follett Hamilton Glenelg Ardonachie Normanby Hamilton Minhamite Areegra Borug Horsham (P.M.) Warracknabeal Argyle Grenville Ballaarat Grenville, Ripon Ascot Ripon; Ballaarat Ballaarat Talbot Ashens Borung Horsham Dunmunkle Audley Normanby Hamilton Dundas, Portland Avenel Anglesey; Seymour Goulburn, Seymour Delatite; Moira Avoca Gladstone; St. Arnaud Avoca Kara Kara Awonga Lowan Horsham Kowree Axedale Bendigo; Bendigo -

Surf-Coast-Shire-Map-Aireys-Inlet.Pdf
Bambra BAMBRA DVE TK RD Creek SURF COAST WALK Lookout Hill PONDS Ironbark Painkalac Gorge HOME OF THE SPLIT POINT CREEK Coast through living landscapes Creek RD IRONBARK Distillery LIGHTHOUSE DUCK Painkalac Offering natural beauty and easy Dam GENTLE DISTILLERY access, the 44km Surf Coast Distillery Creek Picnic Area Painkalac Walk lets you relax and enjoy a ANNIE world-class walking destination at Great Otway RD BOUNDARY National Park BAMBRA RD your own pace. Explore inspiring landscapes on foot or bike beyond Anglesea Moggs BIMBADEEN the edge of Victoria’s beautiful Great Creek MOGGS Ocean Road. N TK RD 0 1 km B100 Relish the rich ochre of the Bells DR Scale COACH Beach cliffs, the deep blue of Bass Moggs Creek Picnic Area Aireys BOYD Strait and the leafy green of eucalypt OLD TK Creek Inlet forests. Discover ancient Aboriginal AV DR traditions, fascinating surf culture FOREST LIALEETA YARRIN Coalmine SHEOAK Hang Gliding CR Surf and abundant wildlife as the Walk YANDANA GA Launching RD Coast RD Walk Place Pole RD connects you with the coastal town COALMINE TK Spion Kopp RD House Creek comforts of Torquay, Anglesea and B100 Fairhaven Fairhaven OCEAN Split Point Aireys Inlet. Eastern Beach AIREYSINLET.ORG.AU GREAT Moggs Creek View Great Ocean Road Whether you’re a nature lover or a Memorial Arch fun lover, whether you take an hour, Lorne BASS STRAIT ONE OF THE COAST’S OLDEST SETTLEMENTS, AIREYS INLET HAS a day or a week, the Surf Coast GROWN AROUND THE FAMOUS SPLIT POINT LIGHTHOUSE INTO A Walk puts a stunning and unique BEAUTIFUL HOLIDAY VILLAGE WITH BREATHTAKING SCENERY AND AN coastal environment within easy reach. -

The Croaker 2014 08 August
THE croaker Correspondence to: the Editors via email: [email protected] Volume 7 No. 4 August 2014 Editors Deb Campbell & Jane Gorman Telstra is coming to the Marsh: Meeting Wednesday August 20th at 5.00pm—7.00pm ADSL & 4G For Deans Marsh: Deans Marsh and district is embarking on a quest to work with Telstra to help us upgrade all our communica- tions systems so that they do actually communicate. We have already collected a list of 50 interested com- munity members to show we are serious. Now we need to assemble and ask questions and put our case. When I first moved to the Marsh from Lorne, I was told by Customer Service in rather triumphal tones ‘Deans Marsh doesn’t have ADSL and it never will’. But it appears this is not necessarily the case. Our neighbours in Lorne and Birregurra campaigned for ADSL and succeeded: now it is our turn. Deans Marsh is right in the middle of one of Victoria’s most fire-prone areas. We have increasing numbers of visitors travelling through whose phones and sat navs do not work here. We also have residents whose mo- biles do not work in their own homes, let alone anywhere outside. We also have expensive and inadequate internet. We are hoping to work with Telstra to make real changes; the first step is a demonstration of support from us all. Anyone who is around 5kms from the Deans Marsh exchange should be able to get ADSL, and a 4G tower would help everyone, including visitors and travellers. -
V I F M & P V I F M & P
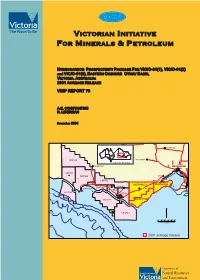
VMPi VIICTORIAN NITIATIVE FMOR INERALS &P ETROLEUM HYDROCARBON P ROSPECTIVITY P ACKAGE F OR VIC/O-01(1), VIC/O-01(2) andVIC/O-01(3) , E ASTERN O NSHORE O TWAY B ASIN, VAICTORIA, USTRALIA: 2001 ACREAGE R ELEASE VIMP REPORT 70 A.E. CONSTANTINE N. LIBERMAN November 2001 KYNETON PEP160 BALLARAT AREA OF INTEREST HAMILTON MELBOURNE PEP151 PEP150 LARA PEP159 GEELONG VIC/O-01(1) VIC/O-01(3) PEP152 (b) COBDEN 200m COLAC PORTLAND PEP154(a) VIC/P46 1000m PEP153 VIC/O-01(2) VIC/P44 2000m 3000m VIC/P43 0 10 20 30 40 50 Km 4000m 2001 acreage release . VIMP Report 70 Hydrocarbon prospectivity package for VIC/O-01(1), VIC/O-01(2) and VIC/O-01(3), Eastern Onshore Otway Basin, Victoria, Australia 2001 Acreage Release A. Constantine and N. Liberman November 2001 Bibliographic reference: CONSTANTINE, A. and LIBERMAN, N., 2001. Hydrocarbon Prospectivity Package for VIC/O-01(1), VIC/O-01(2) and VIC/O-01(3), Eastern Onshore Otway Basin, Victoria, Australia. 2001 Acreage Release. Victorian Initiative for Minerals and Petroleum Report 70. Department of Natural Resources and Environment. © Crown (State of Victoria) Copyright 2001 Petroleum Development ISSN 1323 4536 ISBN 0 7306 9472 0 (Hard Copy) ISBN 0 7306 9473 9 (CD-ROM) This report may be purchased from: Business Centre Minerals & Petroleum Department of Natural Resources and Environment 8th Floor, 240 Victoria Parade East Melbourne, Victoria 3002, Australia For further technical information contact: Manager Petroleum Development Department of Natural Resources and Environment PO Box 500 East Melbourne, Victoria 3002, Australia Website: www.nre.vic.gov.au/minpet/index.htm Authorship and Acknowledgments: The package was compiled and collated by the Basin Studies Group of the Petroleum Development Unit. -

Thomas Butson PEARSE 15 - 108
Thomas PEARSE Family Tree Family Tree of Thomas Pearse 1775 – 18?? & Mary Butson 1775 – 1827 and their descendants Revised – 7th December 2019 – V50 Copyright © - Stewart Robert McConachy 2016 – NO unauthorised use or reproduction permitted 1 Thomas PEARSE Family Tree INTRODUCTION The Pearse Family Tree has been created as a series of vertical charts. The lines on the left side of each page represent the generations. The relevant ancestors are listed at the top of each page. The names of children all touch the line coming directly from the name of their Pearse parent. This index includes all known people of the Pearse family. Women are indexed under their maiden/family name only. Where maiden/family names are not known, married names are used. These entries are indicated thus * Where two or more people have the same name, the year of birth is given. If further identification is required, the line from which they come is indicated, such as (J) for John. Descendants of Maxine Mauldin b 1944 and Baden Sylvester Hooper b 1929 are shown in the Samuel and George McConachy lines. Descendants of Sarah Taylor Pearse 1846 - 1920 and Robert McConachy 1829 - 1918 appear in the Robert McConachy line. Descendants of Robert William Scammell b 1935 and Betty Victoria McConachy b 1935 appear twice in the Thomas Butson line. Joanne Gai Scammell & Craig Norman Sheather appear twice in the Thomas Butson line. We now have 3000 plus people recorded in the Pearse family tree. We would like to continue recording the Pearse Family Tree and it would be appreciated if you would make a note in your diary each year to email or post to us an update of your section of the family. -

DEEP-WATER GIPPSLAND a New Frontier
DEEP-WATER GIPPSLAND A New Frontier • Deep water structures revealed by contemporary seismic and high resolution aeromagnetics • Gippsland petroleum systems extend into new acreage • Potential play-fairways identified PESA News April/May 2000 VICTORIAN SUPPLEMENT MINISTER’S STATEMENT VICTORIAN SUPPLEMENT he discovery of Australia's first giant petroleum fields in Bass Strait in the 1960's had a profound effect on both the Victorian and national economies. Major petrochemical industries and many other manufacturing and Tprofessional businesses are located in the State, largely because of the proximity to the oil and gas reserves in offshore Gippsland. As major a population and infrastructure base, the State provides employees and support for these companies as well as markets for their products. The Australian corporate headquarters of Exxon-Mobil, BP-Amoco and Shell are all located in Melbourne, as well as smaller active oil companies. Victoria is well served by its growing gas infrastructure. With coal fired electricity, the state has benefited from an abundance of energy sources, providing the most competitive energy pricing to business and domestic consumers in the nation. The value of the resource extracted from the basins within Victoria and its Adjacent Area offshore exceeds $3 Billion per year. Although the State realises only a small portion of direct revenue from royalties, it is in the indirect benefit of having a local supply of oil and gas providing the ongoing relatively inexpensive energy that adds so much value to the State. The Brack's Government was elected in 1999 with a mandate to increase energy supply security in the wake of the Longford tragedy in 1998. -

SCG Victorian Councils Post Amalgamation
Analysis of Victorian Councils Post Amalgamation September 2019 spence-consulting.com Spence Consulting 2 Analysis of Victorian Councils Post Amalgamation Analysis by Gavin Mahoney, September 2019 It’s been over 20 years since the historic Victorian Council amalgamations that saw the sacking of 1600 elected Councillors, the elimination of 210 Councils and the creation of 78 new Councils through an amalgamation process with each new entity being governed by State appointed Commissioners. The Borough of Queenscliffe went through the process unchanged and the Rural City of Benalla and the Shire of Mansfield after initially being amalgamated into the Shire of Delatite came into existence in 2002. A new City of Sunbury was proposed to be created from part of the City of Hume after the 2016 Council elections, but this was abandoned by the Victorian Government in October 2015. The amalgamation process and in particular the sacking of a democratically elected Council was referred to by some as revolutionary whilst regarded as a massacre by others. On the sacking of the Melbourne City Council, Cr Tim Costello, Mayor of St Kilda in 1993 said “ I personally think it’s a drastic and savage thing to sack a democratically elected Council. Before any such move is undertaken, there should be questions asked of what the real point of sacking them is”. Whilst Cr Liana Thompson Mayor of Port Melbourne at the time logically observed that “As an immutable principle, local government should be democratic like other forms of government and, therefore the State Government should not be able to dismiss any local Council without a ratepayers’ referendum. -

War-Related Heritage in Victoria
War-related heritage in Victoria The results of a heritage survey documenting the places and objects relating to Victorians’ experiences of war including war memorials, avenues of honour, commemorative places and buildings, honour rolls, memorabilia, objects and other heritage August 2011 This report is based on a veterans heritage survey For more information contact the Department of prepared by Dr David Rowe of Authentic Heritage Planning and Community Development on Services. It was edited, revised and prepared for (03) 9935 3041 or at www.veterans.vic.gov.au publication by Dr Marina Larsson, Veterans Unit, Disclaimer Department of Planning and Community Development, and Dr Janet Butler. This publication may be of assistance to you but the State of Victoria and its employees do not guarantee Dr David Rowe has a Bachelor of Arts (Architecture), that the publication is without flaw of any kind or is Bachelor of Architecture and a PhD (Architecture). He wholly appropriate for your particular purposes and is the Heritage Advisor to the City of Greater Geelong therefore disclaims all liability for any error, loss or other and Golden Plains Shire. David is also the Director of consequence which may arise from you relying on any Authentic Heritage Service Pty Ltd, a private heritage information in this publication. consultancy company. Over the past 17 years, David has prepared a large range of local government Copyright material heritage studies, conservation management plans and Where images are still within their copyright period, other heritage assessments on thousands of places all reasonable efforts have been made in order to across Victoria and has authored a number of heritage determine and acknowledge the identity of holders of publications. -
Fun and Adventure by the Sea
ANGLESEA Fun and adventure by the sea Anglesea Street Index ABC D E F G RD PORTREATH Arinya Cr. C13 Power Torquay & Geelong TANNERS Melbourne Eumeralla RD Station To Anglesea Landfill WOODLAND Belton St. B15 Scout FWY N CECIL Betleigh St. E11 M1 Walk Camp TRACKS WITHIN ANGLESEA HEATH 01020 30 km Port FOREST Great Otway (Dry Weather Only) Anglesea TK 10 PRINCES 10 Bingley Pde. D12 Phillip TK National Park RD GUNDRYS Heath MinorRD road Bay Birdie Ave. A14 Geelong Perimeter FIRETAIL 4WD unsurfaced Anglesea Heath hicle RD RD Winchelsea RD 4WD track (seasonal) Birkdale Cl. B14 Queenscliff sting A1 (Alcoa Lease Area) HARRISON Ferry ound Marshy GUNDRYS Walking track Torquay Great HONEY Butterworth Cr. C13 Deans Anglesea DEPI Office TK ALLARDYCE TK Seasonal road closure Marsh Primary School B100 Otway Anglesea POTS Cameron Rd. E13 6 Mountain Bike Park RD Alcoa Lease Boundary Aireys Inlet National FLAT Creek BASS STRAIT TK Camp Rd. D12 Lorne Park NTH TK PIPELINE DUSTY GUM HAGGARTS MINTER JAROSITE Charles St. C14 TK DR R 11 Perimeter Walk Ellimata 11 D TK TK MILLER RD Reserve Anglesea Chatswood Dr. C13 EYE OCEAN Ovals TK POINT SON ALCOA ELKINGTON Ironbark Heath TK B100 Clairville St. C14 BETLEIGH ST ELLIMATTA RD POWERLINE STH CREEK WILKINS TK EDWARDS Basin HARRI BALD VIEW RD ST Araluen SHINEY Burnside HILLS RIDGE ADDIS Coalmine Rd. B12 Coal Mine River TK Great Lutheran TK ST Camp TK RD RD PDE Camp RD BOUNDARY Otway RD Anglesea Eagle Ave. B14 ST ALCOA ERLINE HURST TK Landfill GREAT Power RAVENTK National CREEK POWRD Eighth Ave. -
Aireys Inlet to Eastern View Neighbourhood Character Study
Aireys Inlet to Eastern View Neighbourhood Character Study Table of Contents Executive Summary………………………………………………………………1 1. Background………………………………………………………………………..3 2. Methodology………………………………………………………………………5 3. Assessment of Key Character Elements……………………………………...11 4. Vegetation Assessment………………………………………………………....29 5. Current Planning Controls……………………………………………………...38 6. Review of Planning Controls…………………………………………………...51 7. Other Issues……………………………………………………………………..62 8. Recommendations………………………………………………………………64 Appendices……………………………………………………………………….65 Maps 1. Location of Precincts (street layout)…………………………………………….7 2. Location of Precincts (aerial photo)……………………………………………..9 3. Distribution of sealed/gravel roads……………………………………………..26 4. Vegetation Assessment.………………………………………………………...30 5. Existing Zones…………………………………………………………………....39 6. Existing Overlays………………………………………………………………...41 7. Proposed minimum lot sizes…………...……..………………………………...58 Appendices 1. “A Study of Resident Perceptions of Neighbourhood Character: Aireys Inlet to Eastern View” (Dr Ray Green, 2003) 2. “Aireys Inlet to Eastern View Neighbourhood Character Study - Vegetation Report” (Mark Trengove, September, 2003) 3. Indigenous Planting Guide (Surf Coast Shire, 2003) 4. Data collected from Physical Survey (Surf Coast Shire, 2003) 5. Precinct Descriptions 6. Case Studies of Existing Developments 7. Reported Sightings of Rufous Bristlebird (Department of Sustainability and Environment, 2004) Copyright The cover photograph of a Common Pink Heath is Copyright © by Dr. Ray Green,