Evaluation of the Fetal Face Disclaimer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -

59. Lateral Facial Clefts
59 LATERAL FACIAL CLEFTS LI OR TRANSVERSE CLEFTS ARE CONSIDERED THE RESULT OF FAILURE OF MESODERM MIGRATION OR MERGING TO OBLITERATE MANDIBULAR THE EMBRYONIC GROOVES BETWEEN THE MAXILLARY AND PROMINENCES TRANSVERSE CLEFTS AS THESE CLEFTS ARE RARE AND ALMOST EVERYBODY HAVING ONE HAS AND REPORTED IT IT IS POSSIBLE TO REVIEW MOST OF THE REPORTED CASES 769 DESCRIBED THE AFTER WHEN NOTE TREATMENT SPECIFIC CASE RECORDINGS IN WHAT MAY SEEM HELTERSKELTER ARRANGEMENT GENERALIZATIONS MAY BE OF VALUE IN 1891 ROSE NOTED FOR LONG THE VERY EXISTENCE OF THIS MACROSROMATOUS DEFORMITY WAS DOUBTED BUT CASES HAVE BEEN RECOGNIZED MORE OR LESS SINCE 1715 WHEN MURALT PICTURED IT FOR THE FIRST TIME ONE OF THE FIRST CASES REPORTED WAS BY VROLIK WHOIN HIS 1849 CLEFTS WORK GAVE SEVERAL ILLUSTRATIONS OF COMMISSURAL AS WELL AS OTHER DEFORMITIES OF THE FACE OTHER CASES WERE REPORTED BY REISSMANN IN 1869 AND MORGAN IN 1882 MACROSTOMIA OR COMMISSURAL HARELIP ACCORDING TO ROSE IS DIAMETER OF WHICH EVIDENCED BY AN INCREASED THE MOUTH MAY VARY IN FROM SLIGHT INCREASE TO CONSIDERABLE DISTANCE CASE RE PORTED BY RYND IN 1862 THE MOUTH OPENING EXTENDED AS FAR AS THE THE LEFT FIRST MOLAR ON THE RIGHT SIDE AND TO THE LAST MOLAR ON IN 1887 SUTTON PUBLISHED THE DRAWING OF CHILD WITH VERY LARGE RED CICATRIX THIS CLEFT THE ANGLES OF WHICH GRADUALLY PASSED INTO SCAR ENDED IN GAPING WOUND OVER THE TEMPORAL REGION EXTEND ING TO THE DURA MATER ROSE ALSO POINTED OUT MACROSROMA IS NOR ONLY ATTENDED BY GREAT DISFIGUREMENT HUT IS ALSO TROU BLESOME FROM THE IMPOSSIBILITY OF THE CHILD RETAINING -

The Evolutionary History of the Human Face
This is a repository copy of The evolutionary history of the human face. White Rose Research Online URL for this paper: https://eprints.whiterose.ac.uk/145560/ Version: Accepted Version Article: Lacruz, Rodrigo S, Stringer, Chris B, Kimbel, William H et al. (5 more authors) (2019) The evolutionary history of the human face. Nature Ecology and Evolution. pp. 726-736. ISSN 2397-334X https://doi.org/10.1038/s41559-019-0865-7 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ THE EVOLUTIONARY HISTORY OF THE HUMAN FACE Rodrigo S. Lacruz1*, Chris B. Stringer2, William H. Kimbel3, Bernard Wood4, Katerina Harvati5, Paul O’Higgins6, Timothy G. Bromage7, Juan-Luis Arsuaga8 1* Department of Basic Science and Craniofacial Biology, New York University College of Dentistry; and NYCEP, New York, USA. 2 Department of Earth Sciences, Natural History Museum, London, UK 3 Institute of Human Origins and School of Human Evolution and Social Change, Arizona State University, Tempe, AZ. -

OCSHCN-10G, Medical Eligibility List for Clinical and Case Management Services.Pdf
OCSHCN-10g (01 2019) (Rev 7-15-2017) Office for Children with Special Health Care Needs Medical Eligibility List for Clinical and Case Management Services BODY SYSTEM ELIGIBLE DISEASES/CONDITIONS ICD-10-CM CODES AFFECTED AUTISM SPECTRUM Autistic disorder, current or active state F84.0 Autistic disorder DISORDER (ASD) F84.3 Other childhood disintegrative disorder Autistic disorder, residual state F84.5 Asperger’s Syndrome F84.8 Other pervasive developmental disorder Other specified pervasive developmental disorders, current or active state Other specified pervasive developmental disorders, residual state Unspecified pervasive development disorder, current or active Unspecified pervasive development disorder, residual state CARDIOVASCULAR Cardiac Dysrhythmias I47.0 Ventricular/Arrhythmia SYSTEM I47.1 Supraventricular/Tachycardia I47.2 Ventricular/Tachycardia I47.9 Paroxysmal/Tachycardia I48.0 Paroxysmal atrial fibrillation I48.1 Persistent atrial fibrillationar I48.2 Chronic atrial fibrillation I48.3 Typical atrial flutter I48.4 Atypical atrial flutter I49.0 Ventricular fibrillation and flutter I49.1 Atrial premature depolarization I49.2 Junctional premature depolarization I49.3 Ventricular premature depolarization I49.49 Ectopic beats Extrasystoles Extrasystolic arrhythmias Premature contractions Page 1 of 28 OCSHCN-10g (01 2019) (Rev 7-15-2017) Office for Children with Special Health Care Needs Medical Eligibility List for Clinical and Case Management Services I49.5 Tachycardia-Bradycardia Syndrome CARDIOVASCULAR Chronic pericarditis -

Effects of Glans Penis Augmentation Using Hyaluronic Acid Gel for Premature Ejaculation
International Journal of Impotence Research (2004) 16, 547–551 & 2004 Nature Publishing Group All rights reserved 0955-9930/04 $30.00 www.nature.com/ijir Effects of glans penis augmentation using hyaluronic acid gel for premature ejaculation JJ Kim1, TI Kwak1, BG Jeon1, J Cheon1 and DG Moon1* 1Department of Urology, Korea University College of Medicine, Sungbuk-ku, Seoul, Korea The main limitation of medical treatment for premature ejaculation is recurrence after withdrawal of medication. We evaluated the effect of glans penis augmentation using injectable hyaluronic acid (HA) gel for the treatment of premature ejaculation via blocking accessibility of tactile stimuli to nerve receptors. In 139 patients of premature ejaculation, dorsal neurectomy (Group I, n ¼ 25), dorsal neurectomy with glandular augmentation (Group II, n ¼ 49) and glandular augmentation (Group III, n ¼ 65) were carried out, respectively. Two branches of dorsal nerve preserving that of midline were cut at 2 cm proximal to coronal sulcus. For glandular augmentation, 2 cc of HA was injected into the glans penis, subcutaneously. At 6 months after each procedure, changes of glandular circumference were measured by tapeline in Groups II and III. In each groups, ejaculation time, patient’s satisfaction and partner’s satisfaction were also assessed. There was no significant difference in preoperative ejaculation time among three groups. Preoperative ejaculation times were 89.2740.29, 101.54759.42 and 96.5752.32 s in Groups I, II and III, respectively. Postoperative ejaculation times were significantly increased to 235.6758.6, 324.247107.58 and 281.9793.2 s in Groups I, II and III, respectively (Po0.01). -
Instruction Manual for Citizen Digital Forehead And
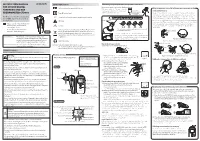
INSTRUCTION MANUAL Symbol Explanations Measuring body temperature (temperature detection) Remove the probe cap and check the probe tip. FOR CITIZEN DIGITAL Refer to instruction manual before use. How to measure correctly in the ear measurement mode * When using it for the first time, open the FOREHEAD AND EAR battery cap and remove the insulation Open the Temperature basics battery cap to THERMOMETER CTD710 Type BF applied part sheet under the battery cap. remove the All objects radiate heat. This device consists of a probe with a built-in insulation sheet. infrared sensor that measures body temperature by detecting the heat Thank you very much for purchasing IP22 Classification for water ingress and particulate matter. radiated by the eardrum and surrounding tissue. Figure 4 shows the the CITIZEN digital forehead and ear Keeping the probe window clean tortuous anatomy of a normal ear canal. As shown in Figure 5, hold the thermometer. Warning Probe window ear and gently pull it back at an angle or pull it straight back to straighten out the ear canal. The shape of the ear canal differs from individual, check • Please read all of the information in before measurement. Accurate temperature measurements make it this instruction manual before Caution essential to straighten the ear canal so that the probe tip directly faces operating the device. the eardrum. • Be sure to have this instruction Indicates this device is subject to the Waste Electrical and Dirt in the probe window will impact the accuracy of temperature detection. External auditory manual to hand during use. 1902LA Electronic Equipment Directive in the European Union. -

Standard Human Facial Proportions
Name:_____________________________________________ Date:__________________Period: __________________ Standard Human Facial Proportions: The standard proportions for the human head can help you place facial features and find their orientation. The list below gives an idea of ideal proportions. • The eyes are halfway between the top of the head and the chin. • The face is divided into 3 parts from the hairline to the eyebrow, from the eyebrow to the bottom of the nose, and from the nose to the chin. • The bottom of the nose is halfway between the eyes and the chin. • The mouth is one third of the distance between the nose and the chin. • The distance between the eyes is equal to the width of one eye. • The face is about the width of five eyes and about the height of about seven eyes. • The base of the nose is about the width of the eye. • The mouth at rest is about the width of an eye. • The corners of the mouth line up with the centers of the eye. Their width is the distance between the pupils of the eye. • The top of the ears line up slightly above the eyes in line with the outer tips of the eyebrows. • The bottom of the ears line up with the bottom of the nose. • The width of the shoulders is equal to two head lengths. • The width of the neck is about ½ a head. Facial Feature Examples.docx Page 1 of 13 Name:_____________________________________________ Date:__________________Period: __________________ PROFILE FACIAL PROPORTIONS Facial Feature Examples.docx Page 2 of 13 Name:_____________________________________________ Date:__________________Period: -
How to Create the Perfect Eyebrow
Creating the Perfect Brows . As a make-up artist, I was acutely aware of the fact that my mother had a need that conventional cosmetics could not meet. She suffered from a type of alopecia (hair loss) of the eyebrows and lashes ever since I could remember. I would draw the eyebrows on for her, but it was often a painstaking process for her to draw the eyebrows on herself on a daily basis. After my mom described the embarrassment of swimming and having the pencil wash off her eyebrows, and another afternoon when a neighbor stopped by after she had been napping and one eyebrow was completely wiped off when she answered the door, it clearly was time for a solution. After completing my certification with the Academy of Micropigmentation, I had one of the most fulfilling days of my life, the day I was able to give a gift of eyebrows to my mother. This was a life changing experience for her and an incredible boost to her self-image. She went on to do her eyeliner, which was especially beneficial to her due to the absence of eyelashes, and I was able to give her lips a fuller appearance with the permanent lipliner. It is said that the facial feature models spend the most time on is their eyebrows and most women, at some point, have altered their eyebrows by tweezing, waxing or electrolysis. As women grow older, the hair on the outer half of their brows tend to become sparse or even non-existent. In ancient China, royalty were the only ones adorned with “tattooed” eyebrows. -

Oral Lesions in Leprosy
Study Oral lesions in leprosy Ana Paula Fucci da Costa, José Augusto da Costa Nery, Maria Leide Wan-del-Rey de Oliveira, Tullia Cuzzi,* Marcia Ramos-e-Silva Departments of Dermatology & *Pathology, HUCFF-UFRJ and School of Medicine, Federal University of Rio de Janeiro, Brazil. Address for correspondence: Marcia Ramos-e-Silva, Rua Sorocaba 464/205, 22271-110, Rio de Janeiro, Brazil. E-mail: [email protected] ABSTRACT Background: Leprotic oral lesions are more common in the lepromatous form of leprosy, indicate a late manifestation, and have a great epidemiological importance as a source of infection. Methods: Patients with leprosy were examined searching for oral lesions. Biopsies of the left buccal mucosa in all patients, and of oral lesions, were performed and were stained with H&E and Wade. Results: Oral lesions were found in 26 patients, 11 lepromatous leprosy, 14 borderline leprosy, and one tuberculoid leprosy. Clinically 5 patients had enanthem of the anterior pillars, 3 of the uvula and 3 of the palate. Two had palatal infiltration. Viable bacilli were found in two lepromatous patients. Biopsies of the buccal mucosa showed no change or a nonspecific inflammatory infiltrate. Oral clinical alterations were present in 69% of the patients; of these 50% showed histopathological features in an area without any lesion. Discussion: Our clinical and histopathological findings corroborate earlier reports that there is a reduced incidence of oral changes, which is probably due to early treatment. The maintenance of oral infection in this area can also lead to and maintain lepra reactions, while they may also act as possible infection sources. -

Ear and Forehead Thermometer
Ear and Forehead Thermometer INSTRUCTION MANUAL Item No. 91807 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 USAD TABLE OF CONTENTS No. Topic Page 1.0 Definition of symbols 5 2.0 Application and functionality 6 2.1 Intended use 6 2.2 Field of application 7 3.0 Safety instructions 7 3.1 General safety instructions 7 3.3 Environment for which the DSO 364 device is not suited 9 3.4 Usage by children and adolescents 10 3.5 Information on the application of the device 10 4.0 Questions concerning body temperature 13 4.1 What is body temperature? 13 4.2 Advantages of measuring the body tempera- ture in the ear 14 4.3 Information on measuring the body tempera- ture in the ear 15 5.0 Scope of delivery / contents 16 6.0 Designation of device parts 17 7.0 LCD display 18 8.0 Basic functions 19 8.1 Commissioning of the device 19 8.2 Warning indicator if the body temperature is 21 too high 2 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. Juli 2014 14:37:38 TABLE OF CONTENTS USA No. Topic Page 8.3 Backlighting / torch function 21 8.4 Energy saving mode 22 8.5 Setting °Celsius / °Fahrenheit 22 9.0 Display / setting time and date 23 9.1 Display of time and date 23 9.2 Setting time and date 23 10.0 Memory mode 26 11.0 Measuring the temperature in the ear 28 12.0 Measuring the temperature on the forehead 30 13.0 Object temperature measurement 32 14.0 Disposal of the device 33 15.0 Battery change and information concerning batteries 33 16.0 Cleaning and care 36 17.0 “Cleaning” warning indicator 37 18.0 Calibration 38 19.0 Malfunctions 39 20.0 Technical specification 41 21.0 Warranty 44 3 19.PJN174-14_GA-USA_HHD-Ohrthermometer_DSO364_28.07.14 Montag, 28. -

Ackerman's Tumour of Buccal Mucosa in a Leprosy Patient
Lepr Rev (2013) 84, 151–157 CASE REPORT Ackerman’s tumour of buccal mucosa in a leprosy patient MANU DHILLON*, RAVIPRAKASH S. MOHAN**, SRINIVASA M. RAJU***, BHUVANA KRISHNAMOORTHY* & MANISHA LAKHANPAL* *Department of Oral Medicine and Radiology, ITS Centre for Dental Studies and Research, Ghaziabad, India **Department of Oral Medicine and Radiology, Kothiwal Dental College and Research Centre, Moradabad, India ***Department of Oral Medicine and Radiology, Saraswati Dental College, Lucknow, India Accepted for publication 23 April 2013 Summary Leprosy (Hansen’s disease) is a chronic granulomatous disease caused by Mycobacterium leprae (Hansen’s bacillus). Oral manifestations occur in 20–60% of cases, usually in lepromatous leprosy, and are well documented. They may involve both the oral hard and soft tissues. Incidence of verrucous carcinoma/Ackerman’s tumour developing in anogenital region and plantar surfaces of feet in lepromatous leprosy has been sufficiently documented in the literature. However, association of oral verrucous carcinoma with lepromatous leprosy has not been established. We report for the first time a case of verrucous carcinoma of the buccal mucosa occurring in a leprotic patient, with brief review of literature on orofacial manifestations of leprosy. Introduction Leprosy (Hansen’s disease) is a chronic, contagious granulomatous disease caused by Mycobacterium leprae (Hansen’s bacillus). The disease presents polar clinical forms (the ‘multibacillary’ or lepromatous leprosy, and ‘paucibacillary’ or tuberculoid leprosy),