Volume of Distribution
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1: Clinical Pharmacokinetics 1
1: CLINICAL PHARMACOKINETICS 1 General overview: clinical pharmacokinetics, 2 Pharmacokinetics, 4 Drug clearance (CL), 6 Volume of distribution (Vd), 8 The half-life (t½), 10 Oral availability (F), 12 Protein binding (PB), 14 pH and pharmacokinetics, 16 1 Clinical pharmacokinetics General overview General overview: clinical pharmacokinetics 1 The ultimate aim of drug therapy is to achieve effi cacy without toxicity. This involves achieving a plasma concentration (Cp) within the ‘therapeutic window’, i.e. above the min- imal effective concentration (MEC), but below the minimal toxic concentration (MTC). Clinical pharmacokinetics is about all the factors that determine variability in the Cp and its time-course. The various factors are dealt with in subsequent chapters. Ideal therapeutics: effi cacy without toxicity Minimum Toxic Concentration (MTC) Ideal dosing Minimum Effective Concentration (MEC) Drug concentration Time The graph shows a continuous IV infusion at steady state, where the dose-rate is exactly appropriate for the patient’s clearance (CL). Inappropriate dosing Dosing too high in relation to the patient’s CL – toxicity likely Minimum Toxic Concentration (MTC) Minimum Effective Concentration (MEC) Dosing too low in relation to the Drug concentration patient’s CL – drug may be ineffective Time Some reasons for variation in CL Low CL High CL Normal variation Normal variation Renal impairment Increased renal blood fl ow Genetic poor metabolism Genetic hypermetabolism Liver impairment Enzyme induction Enzyme inhibition Old age/neonate 2 General overview Clinical Pharmacokinetics Pharmacokinetic factors determining ideal therapeutics If immediate effect is needed, a loading dose (LD) must be given to achieve a desired 1 concentration. The LD is determined by the volume of distribution (Vd). -

Pharmacokinetics, Biodistribution, and Pharmacodynamics of Drug Delivery Systems
JPET Fast Forward. Published on March 5, 2019 as DOI: 10.1124/jpet.119.257113 This article has not been copyedited and formatted. The final version may differ from this version. JPET # 257113 Title: Pharmacokinetic and Pharmacodynamic Properties of Drug Delivery Systems Authors: Patrick M. Glassman, Vladimir R. Muzykantov Affiliation: Department of Systems Pharmacology and Translational Therapeutics, Perelman School of Medicine, University of Pennsylvania Address: 3400 Civic Center Boulevard, Bldg 421, Philadelphia, Pennsylvania 19104-5158, United States Downloaded from jpet.aspetjournals.org at ASPET Journals on September 24, 2021 1 JPET Fast Forward. Published on March 5, 2019 as DOI: 10.1124/jpet.119.257113 This article has not been copyedited and formatted. The final version may differ from this version. JPET # 257113 Running Title: PK/PD Properties of Drug Delivery Systems Corresponding Authors: Vladimir R. Muzykantov ([email protected], (215) 898-9823) and Patrick M. Glassman ([email protected]) # of Text Pages: 22 # of Tables: 2 # of Figures: 4 Word Count – Abstract: 144 Word Count – Introduction: 350 Word Count – Discussion: N/A Downloaded from Non-Standard Abbreviations: Absorption, Distribution, Metabolism, and Elimination (ADME) Biodistribution (BD) Drug Delivery Systems (DDSs) Enhanced Permeability & Retention (EPR) jpet.aspetjournals.org Gastrointestinal (GI) Intravenously (IV) Neonatal Fc Receptor (FcRn) Monoclonal Antibody (mAb) Reticuloendothelial System (RES) at ASPET Journals on September 24, 2021 Pharmacodynamics (PD) Pharmacokinetics (PK) Physiologically-Based Pharmacokinetic (PBPK) Subcutaneously (SC) Target-Mediated Drug Disposition (TMDD) Recommended Section: Drug Discovery and Translational Medicine 2 JPET Fast Forward. Published on March 5, 2019 as DOI: 10.1124/jpet.119.257113 This article has not been copyedited and formatted. -

Multidrug-Resistant Gram-Negative Bacteria
Multidrug-Resistant Gram-Negative Bacteria: Trends, Risk Factors, and Treatments A worldwide public health problem, antibiotic resistance leads to treatment-resistant infections associated with prolonged hospitalizations, increased cost, and greater risk for morbidity. Lee S. Engel MD, PhD CASE INTRODUCTION An 80-year-old female nursing home resident with Antibiotics have saved the lives of millions of people a history of dementia, anemia, atrial fibrillation, and have contributed to the major gains in life ex- hypertension, incontinence, and recurrent urinary pectancy over the last century. In US hospitals, 190 tract infections (UTIs), as well as a long-term Foley million doses of antibiotics are administered each catheter, is admitted because she was found to be day.1 Furthermore, more than 133 million courses febrile and less responsive than normal. The patient of antibiotics are prescribed each year for outpatients. has no drug allergies. Upon admission, she has a However, antibiotic use has also resulted in a major temperature of 38.9ºC, heart rate of 92 beats/min, health care challenge—the development and spread and blood pressure of 106/64 mm Hg. The patient of resistant bacteria. Worldwide, antimicrobial resis- opens her eyes to stimuli but does not speak. Aside tance is most evident in diarrheal diseases, respira- from poor dentition and an irregular heart rate, tory tract infections, meningitis, sexually transmitted findings on physical examination, which includes infections, and hospital and health care–acquired in- a pulmonary and abdominal examination, are nor- fections.2 Vancomycin-resistant enterococci, methi- mal. Serum chemistries demonstrate a white blood cillin-resistant Staphylococcus aureus, multidrug-resis- cell (WBC) count of 11,300 cells/mm3. -

Clinical Pharmacology 1: Phase 1 Studies and Early Drug Development
Clinical Pharmacology 1: Phase 1 Studies and Early Drug Development Gerlie Gieser, Ph.D. Office of Clinical Pharmacology, Div. IV Objectives • Outline the Phase 1 studies conducted to characterize the Clinical Pharmacology of a drug; describe important design elements of and the information gained from these studies. • List the Clinical Pharmacology characteristics of an Ideal Drug • Describe how the Clinical Pharmacology information from Phase 1 can help design Phase 2/3 trials • Discuss the timing of Clinical Pharmacology studies during drug development, and provide examples of how the information generated could impact the overall clinical development plan and product labeling. Phase 1 of Drug Development CLINICAL DEVELOPMENT RESEARCH PRE POST AND CLINICAL APPROVAL 1 DISCOVERY DEVELOPMENT 2 3 PHASE e e e s s s a a a h h h P P P Clinical Pharmacology Studies Initial IND (first in human) NDA/BLA SUBMISSION Phase 1 – studies designed mainly to investigate the safety/tolerability (if possible, identify MTD), pharmacokinetics and pharmacodynamics of an investigational drug in humans Clinical Pharmacology • Study of the Pharmacokinetics (PK) and Pharmacodynamics (PD) of the drug in humans – PK: what the body does to the drug (Absorption, Distribution, Metabolism, Excretion) – PD: what the drug does to the body • PK and PD profiles of the drug are influenced by physicochemical properties of the drug, product/formulation, administration route, patient’s intrinsic and extrinsic factors (e.g., organ dysfunction, diseases, concomitant medications, -

Platform for a Technological Leap in Antibiotics
Columns CHIMIA 2015, 69, No. 12 809 doi:10.2533/chimia.2015.809 Chimia 69 (2015) 809–811 © Schweizerische Chemische Gesellschaft biotechnet Switzerland Hot from the press! Platform for a Technological Leap in Antibiotics as the microbiologist Stewart Thomas Cole, Head of the Cole Laboratory at EPFL – are working on the development of drugs Elsbeth Heinzelmann, science + technology journalist to treat MDR-TB. In a joint start-up meeting in Bern in early au- tumn 2015, partners from academia and industry explained their Abstract: NTN Swiss Biotech™ brings together the Swiss views and objectives in forging plans for a common Antibiotics Biotech Association SBA, which is involved in regulatory, finan- Platform. cial and legal issues, and biotechnet Switzerland, which is ac- tive in translational R&D, to provide a technology base for joint projects. Biotechnet aims to push promising domains by creat- Everyone Contributes Individual Excellence ing topic-oriented platforms that enable academia and industry to work together to produce R&D results of major importance to The Center of Organic and Medicinal Chemistry (ZHW Wae- society and the economy. The first activity initiated by biotech- denswil) places particular emphasis on the design and synthesis net is the Antibiotics Platform that has now been launched. part of the drug discovery process. In order to improve the po- Keywords: Antimicrobial-resistant organisms · Gram-negative tency, selectivity and pharmacokinetic profiles of modulators of bacteria · Klebsiella pneumoniae · Multidrug-resistant strains · validated drug targets, the group rationally designs and synthe- Pathogenesis of tuberculosis sizes novel scaffolds and focused libraries based on X-ray data of co-crystal structures. -

Microrna Pharmacoepigenetics: Posttranscriptional Regulation Mechanisms Behind Variable Drug Disposition and Strategy to Develop More Effective Therapy
1521-009X/44/3/308–319$25.00 http://dx.doi.org/10.1124/dmd.115.067470 DRUG METABOLISM AND DISPOSITION Drug Metab Dispos 44:308–319, March 2016 Copyright ª 2016 by The American Society for Pharmacology and Experimental Therapeutics Minireview MicroRNA Pharmacoepigenetics: Posttranscriptional Regulation Mechanisms behind Variable Drug Disposition and Strategy to Develop More Effective Therapy Ai-Ming Yu, Ye Tian, Mei-Juan Tu, Pui Yan Ho, and Joseph L. Jilek Department of Biochemistry & Molecular Medicine, University of California Davis School of Medicine, Sacramento, California Received September 30, 2015; accepted November 12, 2015 Downloaded from ABSTRACT Knowledge of drug absorption, distribution, metabolism, and excre- we review the advances in miRNA pharmacoepigenetics including tion (ADME) or pharmacokinetics properties is essential for drug the mechanistic actions of miRNAs in the modulation of Phase I and development and safe use of medicine. Varied or altered ADME may II drug-metabolizing enzymes, efflux and uptake transporters, and lead to a loss of efficacy or adverse drug effects. Understanding the xenobiotic receptors or transcription factors after briefly introducing causes of variations in drug disposition and response has proven the characteristics of miRNA-mediated posttranscriptional gene dmd.aspetjournals.org critical for the practice of personalized or precision medicine. The regulation. Consequently, miRNAs may have significant influence rise of noncoding microRNA (miRNA) pharmacoepigenetics and on drug disposition and response. Therefore, research on miRNA pharmacoepigenomics has come with accumulating evidence sup- pharmacoepigenetics shall not only improve mechanistic under- porting the role of miRNAs in the modulation of ADME gene standing of variations in pharmacotherapy but also provide novel expression and then drug disposition and response. -

Stability of Zopiclone in Whole Blood Studies from a Forensic Perspective
Linköping Studies in Health Sciences, Thesis No. 113 Stability of zopiclone in whole blood ‐ Studies from a forensic perspective Gunnel Nilsson Division of Drug Research Department of Medical and Health Sciences Linköping University, Sweden Linköping 2010 Supervisors Robert Kronstrand, Associate Professor Department of Medical and Health Sciences, Faculty of Health Sciences, Linköping University, Sweden Johan Ahlner, Professor Department of Medical and Health Sciences, Faculty of Health Sciences, Linköping University, Sweden Fredrik C. Kugelberg, Associate Professor Department of Medical and Health Sciences, Faculty of Health Sciences, Linköping University, Sweden Gunnel Nilsson, 2010 Published article has been reprinted with permission of the copyright holder. Paper I © 2010 Elsevier, Forensic Science International Printed in Sweden by LiU‐Tryck, Linköping, Sweden, 2010 ISBN 978‐91‐7393‐339‐1 ISSN 1100‐6013 Dala‐Gård Ring the bells that still can ring Forget your perfect offering There is a crack in everything That’s how the light gets in Anthem by Leonard Cohen Contents CONTENTS ABSTRACT ............................................................................................................................. 1 POPULÄRVETENSKAPLIG SAMMANFATTNING..................................................... 3 LIST OF PAPERS ................................................................................................................... 5 ABBREVIATIONS ................................................................................................................ -

Toxicological Profile for Radon
RADON 205 10. GLOSSARY Some terms in this glossary are generic and may not be used in this profile. Absorbed Dose, Chemical—The amount of a substance that is either absorbed into the body or placed in contact with the skin. For oral or inhalation routes, this is normally the product of the intake quantity and the uptake fraction divided by the body weight and, if appropriate, the time, expressed as mg/kg for a single intake or mg/kg/day for multiple intakes. For dermal exposure, this is the amount of material applied to the skin, and is normally divided by the body mass and expressed as mg/kg. Absorbed Dose, Radiation—The mean energy imparted to the irradiated medium, per unit mass, by ionizing radiation. Units: rad (rad), gray (Gy). Absorbed Fraction—A term used in internal dosimetry. It is that fraction of the photon energy (emitted within a specified volume of material) which is absorbed by the volume. The absorbed fraction depends on the source distribution, the photon energy, and the size, shape and composition of the volume. Absorption—The process by which a chemical penetrates the exchange boundaries of an organism after contact, or the process by which radiation imparts some or all of its energy to any material through which it passes. Self-Absorption—Absorption of radiation (emitted by radioactive atoms) by the material in which the atoms are located; in particular, the absorption of radiation within a sample being assayed. Absorption Coefficient—Fractional absorption of the energy of an unscattered beam of x- or gamma- radiation per unit thickness (linear absorption coefficient), per unit mass (mass absorption coefficient), or per atom (atomic absorption coefficient) of absorber, due to transfer of energy to the absorber. -
No Slide Title
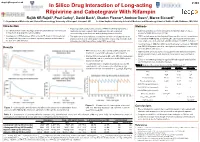
[email protected] In Silico Drug Interaction of Long-acting # 458 Rilpivirine and Cabotegravir With Rifampin Rajith KR Rajoli1, Paul Curley1, David Back1, Charles Flexner2, Andrew Owen1, Marco Siccardi1 1 - Department of Molecular and Clinical Pharmacology, University of Liverpool, Liverpool, UK 2- Johns Hopkins University School of Medicine and Bloomberg School of Public Health, Baltimore, MD, USA Introduction Methods • Physiologically-based pharmacokinetic (PBPK) modelling represents a • Co-administration of anti-TB drugs and many antiretrovirals (ARVs) result mathematical tool to predict DDI magnitude through a detailed • 100 virtual individuals were simulated using Simbiology v.4.3.1, a in important drug-drug interactions (DDIs) understanding of mechanisms underpinning pharmacokinetics product of MATLAB (version 2013b) • Investigation of DDIs between ARVs and anti-TB drugs in individuals can • The objective of this study was to simulate the effect of rifampicin on the • PBPK models were qualified against literature data for oral formulations be complicated by numerous clinical, logistical barriers and also due to pharmacokinetics of cabotegravir and rilpivirine long-acting injectable (LAI) of rifampicin (600 mg OD, at day 6 & 14), cabotegravir and rilpivirine the risk of treatment failure intramuscular (IM) formulations using PBPK modelling (oral, single dose & steady state and IM compared to LATTE-2 studies)1-4 • Loading doses of 800 mg, 900 mg and maintenance doses of 400/800 Results mg, 600/900 mg were used for cabotegravir -

Alcohol Withdrawal
Alcohol withdrawal TERMINOLOGY CLINICAL CLARIFICATION • Alcohol withdrawal may occur after cessation or reduction of heavy and prolonged alcohol use; manifestations are characterized by autonomic hyperactivity and central nervous system excitation 1, 2 • Severe symptom manifestations (eg, seizures, delirium tremens) may develop in up to 5% of patients 3 CLASSIFICATION • Based on severity ○ Minor alcohol withdrawal syndrome 4, 5 – Manifestations occur early, within the first 48 hours after last drink or decrease in consumption 6 □ Manifestations develop about 6 hours after last drink or decrease in consumption and usually peak about 24 to 36 hours; resolution occurs in 2 to 7 days 7 if withdrawal does not progress to major alcohol withdrawal syndrome 4 – Characterized by mild autonomic hyperactivity (eg, tachycardia, hypertension, diaphoresis, hyperreflexia), mild tremor, anxiety, irritability, sleep disturbances (eg, insomnia, vivid dreams), gastrointestinal symptoms (eg, anorexia, nausea, vomiting), headache, and craving alcohol 4 ○ Major alcohol withdrawal syndrome 5, 4 – Progression and worsening of withdrawal manifestations, usually after about 24 hours from the onset of initial manifestations 4 □ Manifestations often peak around 50 hours before gradual resolution or may continue to progress to severe (complicated) withdrawal, particularly without treatment 4 – Characterized by moderate to severe autonomic hyperactivity (eg, tachycardia, hypertension, diaphoresis, hyperreflexia, fever); marked tremor; pronounced anxiety, insomnia, -

Pharmacology Part 2: Introduction to Pharmacokinetics
J of Nuclear Medicine Technology, first published online May 3, 2018 as doi:10.2967/jnmt.117.199638 PHARMACOLOGY PART 2: INTRODUCTION TO PHARMACOKINETICS. Geoffrey M Currie Faculty of Science, Charles Sturt University, Wagga Wagga, Australia. Regis University, Boston, USA. Correspondence: Geoff Currie Faculty of Science Locked Bag 588 Charles Sturt University Wagga Wagga 2678 Australia Telephone: 02 69332822 Facsimile: 02 69332588 Email: [email protected] Foot line: Introduction to Pharmacokinetics 1 Abstract Pharmacology principles provide key understanding that underpins the clinical and research roles of nuclear medicine practitioners. This article is the second in a series of articles that aims to enhance the understanding of pharmacological principles relevant to nuclear medicine. This article will build on the introductory concepts, terminology and principles of pharmacodynamics explored in the first article in the series. Specifically, this article will focus on the basic principles associated with pharmacokinetics. Article 3 will outline pharmacology relevant to pharmaceutical interventions and adjunctive medications employed in general nuclear medicine, the fourth pharmacology relevant to pharmaceutical interventions and adjunctive medications employed in nuclear cardiology, the fifth the pharmacology related to contrast media associated with computed tomography (CT) and magnetic resonance imaging (MRI), and the final article will address drugs in the emergency trolley. 2 Introduction As previously outlined (1), pharmacology is the scientific study of the action and effects of drugs on living systems and the interaction of drugs with living systems (1-7). For general purposes, pharmacology is divided into pharmacodynamics and pharmacokinetics (Figure 1). The principle of pharmacokinetics is captured by philosophy of Paracelsus (medieval alchemist); “only the dose makes a thing not a poison” (1,8,9). -

Ontogeny of Plasma Proteins, Albumin and Binding of Diazepam, Cyclosporine, and Deltamethrin
nature publishing group Basic Science Investigation Articles Ontogeny of plasma proteins, albumin and binding of diazepam, cyclosporine, and deltamethrin Pankaj K. Sethi1,2, Catherine A. White1, Brian S. Cummings1, Ronald N. Hines3–5, Srinivasa Muralidhara1 and James V. Bruckner1 BACKGROUND: To characterize the ontogeny of plasma for example, have been attributed to significant elevations albumin and total proteins, due to the lack of a comprehensive in serum concentrations of unbound parent compound and pediatric database. Secondly, to establish the magnitude and N-desmethyldiazepam, its major active metabolite (7). duration of maturational changes in binding of highly-bound There are number of factors that influence plasma binding of drugs/chemicals. drugs and other chemicals, some of which can be age-related. METHODS: Anonymized plasma samples from 296 donors These include the drug and its concentration, the presence of were pooled in 6 age brackets from birth to adolescence. Total binding competitors, the type and quantity of plasma protein, protein and albumin levels were measured in each age group, and the proteins’ affinity for the drug. Nau et al. (7) observed a as was the age-dependency of plasma binding of diazepam twofold increase in the free fraction of diazepam in the serum (DZP), cyclosporine (CYC), and deltamethrin (DLM), a pyre- of neonates that accompanied marked increases in free fatty throid insecticide. acids and bilirubin, competitors for albumin-binding sites. RESULTS: Plasma levels of albumin and total proteins steadily Albumin levels progressively rose during a 6-d postgestation increased for the first 1–3 y of life. Unbound DZP and CYC monitoring period, but remained significantly lower than in fractions were elevated three- to fourfold in neonates, but adults.