Variation of the Axillary Arch Muscle with Multiple Insertions Loukas M, Noordeh N, Tubbs R S, Jordan R
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomical Variations of Brachial Plexus in Fetal Cadavers
DOI: 10.5137/1019-5149.JTN.21339-17.2 Received: 27.07.2017 / Accepted: 18.10.2017 Published Online: 13.11.2017 Original Investigation Anatomical Variations of Brachial Plexus in Fetal Cadavers Alparslan KIRIK1, Senem Ertugrul MUT2, Mehmet Kadri DANEYEMEZ3, Halil Ibrahim SECER4 1Etimesgut Sehit Sait Erturk State Hospital, Neurosurgery Clinic, Ankara, Turkey 2University of Kyrenia, Faculty of Medicine, Visiting Professor, Near East University, Faculty of Medicine, Department of Neurology, Girne, Turkish Republic of Northern Cyprus 3University of Health Sciences, Gulhane Training and Research Hospital, Department of Neurosurgery, Ankara, Turkey 4University of Kyrenia, Faculty of Medicine, Visiting Professor, Near East University, Faculty of Medicine, Department of Neurosurgery, Girne, Turkish Republic of Northern Cyprus This study has been presented as an oral presentation at the 25th Scientific Congress of the Turkish Neurosurgical Society between 22 and 26 April 2011 at Antalya, Turkey. ABSTRACT AIM: The plexus brachialis is a complex structure with anatomical variations and connections with neighboring tissues. These variations may cause disparity in the motor and sensorial innervations of the upper extremity. The knowledge of anatomy and possible variations are important for performing surgical procedures in the neck, shoulder and axilla. This study was planned to demonstrate the anatomical variations of the infantile brachial plexus. MaterIAL and METHODS: A total of 20 plexus brachialis from 11 fetal cadavers were dissected and examined microscopically. The branching patterns and variations were evaluated. The width of the nerves was assessed at the level of the nerve root, trunk and cord on the basis of all brachial plexuses and they were arranged in terms of thickness. -

Accessory Subscapularis Muscle – a Forgotten Variation?
+Model MORPHO-307; No. of Pages 4 ARTICLE IN PRESS Morphologie (2017) xxx, xxx—xxx Disponible en ligne sur ScienceDirect www.sciencedirect.com CASE REPORT Accessory subscapularis muscle — A forgotten variation? Muscle subscapulaire accessoire — Une variation oubliée ? a a a b L.A.S. Pires , C.F.C. Souza , A.R. Teixeira , T.F.O. Leite , a a,∗ M.A. Babinski , C.A.A. Chagas a Department of morphology, biomedical institute, Fluminense Federal university, Niterói, Rio de Janeiro, Brazil b Interventional radiology unit, radiology institute, medical school, university of São Paulo, São Paulo, Brazil KEYWORDS Summary The quadrangular space is a space in the axilla bounded by the inferior margin of Anatomic variations; the teres minor muscle, the superior margin of the teres major muscle, the lateral margin of Accessory the long head of the triceps brachii muscle and the surgical neck of the humerus, medially. subscapularis muscle; The axillary nerve (C5-C6) and the posterior circumflex humeral artery and veins pass through Axillary nerve; this space in order to supply their territories. The subscapularis muscle is situated into the Subscapularis muscle scapular fossa and inserts itself into the lesser tubercle of the humerus, thus helping stabilize the shoulder joint. A supernumerary muscle known as accessory subscapularis muscle originates from the anterior surface of the muscle and usually inserts itself into the shoulder joint. It is a rare variation with few reports of its existence and incidence. We present a case of the accessory subscapularis muscle in a male cadaver fixated with a 10% formalin solution. The muscle passed anteriorly to the axillary nerve, thus, predisposing an individual to quadrangular space compression syndrome. -

Thoracic Outlet and Pectoralis Minor Syndromes
S EMINARS IN V ASCULAR S URGERY 27 (2014) 86– 117 Available online at www.sciencedirect.com www.elsevier.com/locate/semvascsurg Thoracic outlet and pectoralis minor syndromes n Richard J. Sanders, MD , and Stephen J. Annest, MD Presbyterian/St. Luke's Medical Center, 1719 Gilpin, Denver, CO 80218 article info abstract Compression of the neurovascular bundle to the upper extremity can occur above or below the clavicle; thoracic outlet syndrome (TOS) is above the clavicle and pectoralis minor syndrome is below. More than 90% of cases involve the brachial plexus, 5% involve venous obstruction, and 1% are associate with arterial obstruction. The clinical presentation, including symptoms, physical examination, pathology, etiology, and treatment differences among neurogenic, venous, and arterial TOS syndromes. This review details the diagnostic testing required to differentiate among the associated conditions and recommends appropriate medical or surgical treatment for each compression syndrome. The long- term outcomes of patients with TOS and pectoralis minor syndrome also vary and depend on duration of symptoms before initiation of physical therapy and surgical intervention. Overall, it can be expected that 480% of patients with these compression syndromes can experience functional improvement of their upper extremity; higher for arterial and venous TOS than for neurogenic compression. & 2015 Published by Elsevier Inc. 1. Introduction compression giving rise to neurogenic TOS (NTOS) and/or neurogenic PMS (NPMS). Much less common is subclavian Compression of the neurovascular bundle of the upper and axillary vein obstruction giving rise to venous TOS (VTOS) extremity can occur above or below the clavicle. Above the or venous PMS (VPMS). -

Pectoral Muscles 1. Remove the Superficial Fascia Overlying the Pectoralis Major Muscle (Fig
BREAST, PECTORAL REGION, AND AXILLA LAB (Grant's Dissector (16th Ed.) pp. 28-38) TODAY’S GOALS: 1. Identify the major structural and tissue components of the female breast, including its blood supply. 2. Identify examples of axillary lymph nodes and understand the lymphatic drainage of the breast. 3. Identify the pectoralis major, pectoralis minor, and serratus anterior muscles. Demonstrate their bony attachments, nerve supply, and actions. 4. Identify the walls and associated muscles of the axilla. 5. Identify the axillary sheath, axillary vein, and the 6 major branches of the axillary artery. 6. Identify and trace the cords of the brachial plexus and their branches. DISSECTION NOTES: The donor should be in the supine position. Breast 1. The breast or mammary gland is a modified sweat gland embedded in the superficial fascia overlying the anterior chest wall. Refer to Fig. 2.5A for incisions for reflecting skin of the pectoral region to the mid-arm. Do this bilaterally. Within the superficial fascia in front of the shoulder and along the lateral and lower medial portions of the arm locate the cephalic and basilic veins and preserve these for now. Observe the course of the cephalic vein from the arm into the deltopectoral groove between the deltoid and pectoralis major muscles. 2. For those who have a female donor, mobilize the breast by inserting your fingers behind it within the retromammary space and separate it from the underlying deep fascia of the pectoralis major (see Fig. 2.7). An extension of breast tissue (axillary tail) from the superolateral (upper outer) quadrant often extends around the lateral border of the pectoralis major muscle into the axilla. -

Comparative Anatomy of the Pectoral Girdle and Upper Forelimb in Man and the Lower Primates
Comparative anatomy of the pectoral girdle and upper forelimb in man and the lower primates Item Type text; Thesis-Reproduction (electronic) Authors Barter, James T. Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 06/10/2021 05:49:51 Link to Item http://hdl.handle.net/10150/551254 COMPARATIVE ANATOMY OF THE PECTORAL GIRDLE AND UPPER FORELIMB IN MAN AND THE LOWER PRIMATES by James T. Barter A Thesis submitted to the faculty of the Department of Anthropology in partial fulfillment of the requirements for the degree of MASTER OF ARTS in the Graduate College, University of Arizona 1955 Approved: Director of Thesis ET'-H " r n s r - r This thesis has been submitted in partial fnlfillment o f' require ments for an advanced, degree at the University of Arizona and is deposited in the Library to be made available to borrowers under rules of the Library» Brief quotations from this thesis are allowable without special permission, provided that accurate- acknowledgment of source is made* Requests for permission for extended quotation from or reproduction of this manuscript in whole or in part may be granted by the head of the major depart ment or the dean of the Graduate College when in their judgment the proposed use of the; material is in the interests of scholar ship* In a ll other instances, however, permission must be obtained from the author* SIGEBDg T- : i Table of Contents: ' : " . -

A Narrative Review of Poland's Syndrome
Review Article A narrative review of Poland’s syndrome: theories of its genesis, evolution and its diagnosis and treatment Eman Awadh Abduladheem Hashim1,2^, Bin Huey Quek1,3,4^, Suresh Chandran1,3,4,5^ 1Department of Neonatology, KK Women’s and Children’s Hospital, Singapore, Singapore; 2Department of Neonatology, Salmanya Medical Complex, Manama, Kingdom of Bahrain; 3Department of Neonatology, Duke-NUS Medical School, Singapore, Singapore; 4Department of Neonatology, NUS Yong Loo Lin School of Medicine, Singapore, Singapore; 5Department of Neonatology, NTU Lee Kong Chian School of Medicine, Singapore, Singapore Contributions: (I) Conception and design: EAA Hashim, S Chandran; (II) Administrative support: S Chandran, BH Quek; (III) Provision of study materials: EAA Hashim, S Chandran; (IV) Collection and assembly: All authors; (V) Data analysis and interpretation: BH Quek, S Chandran; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: A/Prof. Suresh Chandran. Senior Consultant, Department of Neonatology, KK Women’s and Children’s Hospital, Singapore 229899, Singapore. Email: [email protected]. Abstract: Poland’s syndrome (PS) is a rare musculoskeletal congenital anomaly with a wide spectrum of presentations. It is typically characterized by hypoplasia or aplasia of pectoral muscles, mammary hypoplasia and variably associated ipsilateral limb anomalies. Limb defects can vary in severity, ranging from syndactyly to phocomelia. Most cases are sporadic but familial cases with intrafamilial variability have been reported. Several theories have been proposed regarding the genesis of PS. Vascular disruption theory, “the subclavian artery supply disruption sequence” (SASDS) remains the most accepted pathogenic mechanism. Clinical presentations can vary in severity from syndactyly to phocomelia in the limbs and in the thorax, rib defects to severe chest wall anomalies with impaired lung function. -

Familial Absenceof the Pectoralis Major, Serratus Anterior, And
J Med Genet: first published as 10.1136/jmg.22.5.390 on 1 October 1985. Downloaded from Journal of Medical Genetics, 1985, 22, 390-392 Familial absence of the pectoralis major, serratus anterior, and latissimus dorsi muscles T J DAVID* AND R M WINTERt From *the Department of Child Health, University ofManchester; and tthe Kennedy-Galton Centrefor Clinical Genetics, Harperbury Hospital, Hertfordshire. SUMMARY Congenital absence of shoulder girdle muscles is described in three generations of a family. The proband, a 3 year old boy, had absence of the sternocostal head of the right pectoralis major. His father had absence of the left serratus anterior and part of the left latissimus dorsi and his paternal grandfather had absence of the lower two-thirds of the left pectoralis major, with absence of the left serratus anterior and latissimus dorsi muscles. The condition is probably the result of a dominant gene. These observations show that absence of the pectoralis major is part of a wider spectrum of shoulder girdle defects. Where genetic advice is sought by persons with apparently sporadic absence of the pectoralis major, examination of the relatives is necessary. The Poland anomaly comprises unilateral absence of of the Poland anomaly or isolated absence of the the pectoralis major combined with an ipsilateral pectoralis. The pedigree is shown in fig 1. malformation of the hand which usually includes syndactyly. It is currently unclear whether isolated Case reports absence of the pectoralis major muscle and the CASE 1 Poland anomaly are part of the same spectrum of IV.3 was a male infant, the product of the first defects or are separate entities.1 Both are consis- 30 year old http://jmg.bmj.com/ tently unilateral and both are usually sporadic pregnancy of a 29 year old mother and 2 father, who had been married for seven years. -

Thoracic Outlet Syndrome of Pectoralis Minor Etiology Mimicking Cardiac
0008-3194/2012/311–315/$2.00/©JCCA 2012 Thoracic outlet syndrome of pectoralis minor etiology mimicking cardiac symptoms on activity: a case report Gary Fitzgerald BSc(NUI), BSc(Hons)(Chiro), MSc(Chiro), ICSSD* Thoracic outlet syndrome is the result of compression Le syndrome de la traversée thoracobrachial est le or irritation of neurovascular bundles as they pass résultat de la compression ou de l’irritation d’un from the lower cervical spine into the arm, via the paquet vasculonerveux au cours de son trajet entre axilla. If the pectoralis minor muscle is involved the la colonne cervicale inférieure et le bras, en passant patient may present with chest pain, along with pain par l’aisselle. Si le muscle petit pectoral est sollicité, and paraesthesia into the arm. These symptoms are also le patient peut subir de la douleur à la poitrine ainsi commonly seen in patients with chest pain of a cardiac que de la douleur et de la paresthésie dans le bras. origin. In this case, a patient presents with a history of On voit souvent ces symptômes aussi chez des patients left sided chest pain with pain and paraesthesia into the souffrant de douleurs thoraciques d’origine cardiaque. left upper limb, which only occurs whilst running. The Dans de tels cas, le patient présente des antécédents de symptoms were reproduced on both digital pressure over douleurs thoraciques du côté gauche, accompagnées the pectoralis minor muscle and on provocative testing de douleur et de paresthésie dans le membre supérieur for thoracic outlet syndrome. The patient’s treatment gauche, qui survient uniquement pendant que le patient therefore focused on the pectoralis minor muscle, with court. -

Download PDF File
Folia Morphol. Vol. 79, No. 1, pp. 1–14 DOI: 10.5603/FM.a2019.0047 R E V I E W A R T I C L E Copyright © 2020 Via Medica ISSN 0015–5659 journals.viamedica.pl Should Terminologia Anatomica be revised and extended? A critical literature review P.P. Chmielewski1, B. Strzelec2, 3 1Division of Anatomy, Department of Human Morphology and Embryology, Faculty of Medicine, Wroclaw Medical University, Wroclaw, Poland 2Department and Clinic of Vascular, General and Transplantation Surgery, Jan Mikulicz-Radecki Medical University Hospital, Wroclaw Medical University, Wroclaw, Poland 3Department and Clinic of Gastrointestinal and General Surgery, Wroclaw Medical University, Wroclaw, Poland [Received: 14 November 2018; Accepted: 31 December 2018] The first edition of the Terminologia Anatomica was published in 1998 by the Federative Committee for Anatomical Terminology, whereas the second edition was issued in 2011 by the Federative International Programme for Anatomical Terminologies. Since then many attempts have been made to revise and extend the official terminology as several inconsistencies have been noted. Moreover, numerous crucial terms were either omitted or deliberately excluded from the official terminology, like sulcus popliteus and diaphragma urogenitale, respec- tively. Furthermore, several synonyms are to be discarded. Notwithstanding the criticism, the use of the current version of terminology is strongly recommended. Although the Terminologia Anatomica is open to future expansion and revision, every change should be made after a thorough discussion of the historical context and scientific legitimacy of a given term. The anatomical nomenclature must be as simple as possible but also precise and coherent. It is generally accepted that hasty innovation ought not to be endorsed. -

Pectoral Region and Axilla Doctors Notes Notes/Extra Explanation Editing File Objectives
Color Code Important Pectoral Region and Axilla Doctors Notes Notes/Extra explanation Editing File Objectives By the end of the lecture the students should be able to : Identify and describe the muscles of the pectoral region. I. Pectoralis major. II. Pectoralis minor. III. Subclavius. IV. Serratus anterior. Describe and demonstrate the boundaries and contents of the axilla. Describe the formation of the brachial plexus and its branches. The movements of the upper limb Note: differentiate between the different regions Flexion & extension of Flexion & extension of Flexion & extension of wrist = hand elbow = forearm shoulder = arm = humerus I. Pectoralis Major Origin 2 heads Clavicular head: From Medial ½ of the front of the clavicle. Sternocostal head: From; Sternum. Upper 6 costal cartilages. Aponeurosis of the external oblique muscle. Insertion Lateral lip of bicipital groove (humerus)* Costal cartilage (hyaline Nerve Supply Medial & lateral pectoral nerves. cartilage that connects the ribs to the sternum) Action Adduction and medial rotation of the arm. Recall what we took in foundation: Only the clavicular head helps in flexion of arm Muscles are attached to bones / (shoulder). ligaments / cartilage by 1) tendons * 3 muscles are attached at the bicipital groove: 2) aponeurosis Latissimus dorsi, pectoral major, teres major 3) raphe Extra Extra picture for understanding II. Pectoralis Minor Origin From 3rd ,4th, & 5th ribs close to their costal cartilages. Insertion Coracoid process (scapula)* 3 Nerve Supply Medial pectoral nerve. 4 Action 1. Depression of the shoulder. 5 2. Draw the ribs upward and outwards during deep inspiration. *Don’t confuse the coracoid process on the scapula with the coronoid process on the ulna Extra III. -

Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain
International Journal of Science and Research (IJSR) ISSN: 2319-7064 ResearchGate Impact Factor (2018): 0.28 | SJIF (2019): 7.583 Effect of Latissimus Dorsi Muscle Strengthening in Mechanical Low Back Pain 1 2 Vishakha Vishwakarma , Dr. P. R. Suresh 1, 2PCPS & RC, People’s University, Bhopal (M.P.), India Abstract: Mechanical low back pain (MLBP) is one of the most common musculoskeletal pain syndromes, affecting up to 80% of people at some point during their lifetime. Sources of back pain are numerous, usually sought in as lesion of disc or facet joints at L4- L5 and L5-S1 levels. Studies have shown that 40% of all back pain is of thoracolumbar origin. The term meachnical low back pain also gives reassurance that there is no damage to the nerves or spinal pathology. The clinical presentation of mechanical low back pain usually the ages 18-55 years is in the lumbo sacral region. A study was conducted to evaluate the designed to check the effectiveness of Conventional Exercises alone in Mechanical low back pain and along with the latissimus dorsi muscle strengthening, data was collected from People’s hospital, Bhopal (age group-30-45 yr both male and female randomly) Keywords: Visual analog scale, Assessment chart, Treatment table, Data collection sheets, Essential stationery materials, Computer, SPSS Software etc. 1. Introduction Back pain is a primary to seek medical advice considering 80% of people suffering from back pain. Mechanical low back pain is defined as a result of minor intervertebral dysfunction and referred pain in the low back The latissimus dorsi is a large, flat muscle on the back that and hip region, and can often be confused with the other stretches to the sides, behind the arm, and is partly covered pathologies that may cause these symptoms.18 by the trapezius on the back near the midline, the word latissimus dorsi comes from Latin and its means, broadest muscle of the back dorsum means back. -
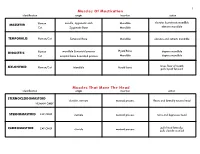
Muscles of Mastication Muscles That Move the Head
1 Muscles Of Mastication identification origin insertion action maxilla, zygomatic arch Mandible elevates & protracts mandible MASSETER Human Cat Zygomatic Bone Mandible elevates mandible TEMPORALIS Human/Cat Temporal Bone Mandible elevates and retracts mandible Hyoid Bone DIGASTRIC Human mandible & mastoid process depress mandible Cat occipital bone & mastoid process Mandible depress mandible raises floor of mouth; MYLOHYOID Human/Cat Mandible Hyoid bone pulls hyoid forward Muscles That Move The Head identification origin insertion action STERNOCLEIDOMAStoID clavicle, sternum mastoid process flexes and laterally rotates head HUMAN ONLY STERNOMAStoID CAT ONLY sternum mastoid process turns and depresses head pulls head laterally; CLEIDOMAStoID CAT ONLY clavicle mastoid process pulls clavicle craniad 2 Muscles Of The Hyoid, Larynx And Tongue identification origin insertion action Human Sternum Hyoid depresses hyoid bone STERNOHYOID Cat costal cartilage 1st rib Hyoid pulls hyoid caudally; raises ribs and sternum sternum Throid cartilage of larynx Human depresses thyroid cartilage STERNothYROID Cat costal cartilage 1st rib Throid cartilage of larynx pulls larynx caudad elevates thyroid cartilage and Human thyroid cartilage of larynx Hyoid THYROHYOID depresses hyoid bone Cat thyroid cartilage of larynx Hyoid raises larynx GENIOHYOID Human/Cat Mandible Hyoid pulls hyoid craniad 3 Muscles That Attach Pectoral Appendages To Vertebral Column identification origin insertion action Human Occipital bone; Thoracic and Cervical raises clavicle; adducts,