2015 Senate Human Services
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

May State Legislation Update
May State Legislation Update Last Updated: June 04, 2019 Introduction LawView is a tool that will track state legislation on a monthly and as-needed basis. These reports cover state developments critical to the news media industry so that our members can affect policy decisions at a local level. We can add issues or bills to cover, pull reports on a specific piece of legislation upon request, and are open to suggestions for how we will shape this tool for you moving forward. Please email us at [email protected]. Bills by State Bills by Issue Anti-SLAPP 8 Drones 1199 0 10 20 30 FOIA 8 Political Ads 9 WA Public Notice 3355 ME MT ND OR MN Telemarketing 1100 ID WI VT SD MI NY WY NH Privacy 6688 NE IA PA NV OH MA UT IL IN CO WV VA RI KS MO KY CA CT TN NC AZ NM OK AR SC NJ MS AL GA DE TX LA MD DC AK FL HI US Congress Key Updates on Issues Privacy Related Bills: NY S 5575: Second Report Cal. 6/3/19 IL SB 2263: Failed Sine Die 5/31/19 CA AB 25: Read First Time in Senate 5/30/19 NY S 5575: First Report 5/30/19 ME LD 946 (SP 275): Passed House 5/30/19 CA AB 873: Referred to Senate Judiciary 5/29/19 CA AB 1416: Passed Assembly 5/29/19 TX HB 4390: Sent to the Governor 5/29/19 CA AB 846: Read First Time in Senate 5/29/19 IL SB 1624: Passed House 5/27/19 IL HB 3357: Added Chief Co-Sponsors 5/26/19 OR SB 684: Enacted 5/24/19 CA AB 1035: Read Second Time in Senate 5/23/19 CA AB 1355: Referred to Senate Judiciary 5/22/19 CA AB 1564: Referred to Senate Judiciary 5/22/19 CA AB 874: Referred to Senate Judiciary 5/22/19 NY A 5635: Recommitted to -

MEETING of the BOARD of CITY COMMISSIONERS December 16, 2020
MEETING OF THE BOARD OF CITY COMMISSIONERS December 16, 2020 On December 16, 2020, the Board of City Commission met for a Special Meeting, at 3:30 p.m. to discuss the City’s Legislative Agenda with the North Dakota State Legislators. Those present included: City Officials: City Administrator Keith Hunke, Assistant City Administrator Jason Tomanek, City Attorney Jannelle Combs, Public Information Officer Gloria David, Community Development Director Ben Ehreth, Event Center Director Charlie Jeske, Public Library Director Christine Kujawa, Police Chief Dave Draovitch, Finance Director Dmitriy Chernyak, City Engineer Gabe Schell, Airport Director Gregory Haug, Public Works Service Operations Director Jeff Heintz, Public Works Utility Operations Director Michelle Klose, Fire Chief Joel Boespflug, Clerk of Court Kathy Wangler, Public Health Director Renae Moch and Human Resources Director Robert McConnell. The Board of City Commissioners: Nancy Guy, Steve Marquardt, Greg Zenker, Mark Splonskowski and Mayor Steve Bakken, Legislators: Larry Klemin, Pat Heinert, Bob Martinson, Karen Karls, Erin Oban, Lisa Meier, Dick Dever, Glenn Bosch, Mike Nathe, Diane Larson, Jason Dockter, Nicole Poolman, Michael Dwyer and George Keiser. Others: Sam Nelson, a reporter with the Bismarck Tribune, Maddie Biertempfel, a reporter with KX News and Toni Haider, a design engineer with Barr Engineering Co., were also present. All parties participated via Microsoft Teams. Mayor Bakken and City Administrator Hunke provided a street utility update. The Street Utility Fee would replace the current City policy of utilizing special assessments as revenue for street maintenance projects with an alternative funding source such as a street utility fee. The update detailed the scope of work the City is currently undergoing with AE2S Nexus staff to begin the process of incorporating the street utility fee. -

Labor Townhall Posters 1-8-18.Xlsx
Official District Party 2013 2015 2017 Representative 60% 83% 48% Andrew 3 R Maragos Representative 0% 8% 17% Rosco Streyle 3 R Senator Oley 25% 9% 17% Larsen 3 R Official District Party 2013 2015 2017 Representative 26% Terry B. Jones 4 R Representative 27% Bill Oliver 4 R Senator Jordan Kannianen 4 R Official District Party 2013 2015 2017 Representative 0% 8% 4% Roger Brabandt 5 R Representative 0% 8% 17% Scott Louser 5 R Senator Randall 25% 36% 25% Burckhard 5 R Official District Party 2013 2015 2017 Representative 30% 27% 18% Dick Anderson 6 R Representative 26% Craig A. 6 R Johnson Senator Shawn Vedda 6 R Official District Party 2013 2015 2017 Representative 0% 16% 18% Rick Becker 7 R Representative 0% 25% 22% Jason Dockter 7 R Senator Nicole 25% 36% 83% Poolman 7 R Official District Party 2013 2015 2017 Representative 0% 25% 22% Jeff Delzer 8 R Representative 30% 25% 30% Vernon Laning 8 R Senator Howard 25% 27% 50% Anderson 8 R Official District Party 2013 2015 2017 Representative 100% 100% 91% Tracy Boe 9 D Representative 100% 100% 86% Marvin Nelson 9 D Senator Richard 100% 100% 83% Marcellais 9 D Official District Party 2013 2015 2017 Representative 100% 100% 100% Ron Guggisberg 11 D Representative 95% Gretchen 11 D Dobervich Senator Tim 100% 91% 100% Mathern 11 D Official District Party 2013 2015 2017 Representative 0% 10% 22% Kim Koppelman 13 R Representative 8% 14% Christopher 13 R Olson Senator Judy 63% 54% 83% Lee 13 R Official District Party 2013 2015 2017 Representative 50% 42% 48% Jon Nelson 14 R Representative 10% 16% 22% Robin Weisz 14 R Senator Jerry 13% 0% 67% Klein 14 R Official District Party 2013 2015 2017 Representative 5% Andrew 16 R Marschall Representative 0% 9% 18% Ben Koppelman 16 R Senator David a. -
ND 2020 Burleigh Pri Pub-20-5-14-15-53-49
STATE OF NORTH DAKOTA BURLEIGH COUNTY CONSOLIDATED PRIMARY ELECTION BALLOT PRIMARY ELECTION JUNE 9, 2020 ATTENTION! READ BEFORE VOTING POLITICAL PARTY BALLOT In a Political Party Primary Election, you may only vote for the candidates of one political party. This ballot contains three political parties; one in each section. If you vote in more than one political party's section, your Political Party Ballot will be rejected; however, all votes on the No Party and Measures Ballots will still be counted. To vote for the candidate of your choice, you must darken the oval ( ) next to the name of that candidate. To vote for a person whose name is not printed on the ballot, you must darken the oval ( ) next to the blank line provided and write that person's name on the blank line. REPUBLICAN REPUBLICAN DEMOCRATIC-NPL Representative in Congress State Representative State Senator Vote for no more than ONE name District 32 District 28 Vote for no more than TWO names Vote for no more than ONE name Kelly Armstrong Lisa Meier Pat Heinert State Senator State Senator District 08 District 30 Vote for no more than ONE name Vote for no more than ONE name Howard C Anderson Jr Governor and Lt. Governor Vote for no more than ONE set of names State Senator Doug Burgum and District 32 State Senator Brent Sanford Vote for no more than ONE name District 28 Vote for no more than ONE name Michael Coachman and Amelia Doll Joel H Hylden Robert S Erbele State Representative District 08 State Senator Vote for no more than TWO names District 30 State Auditor Vote for -
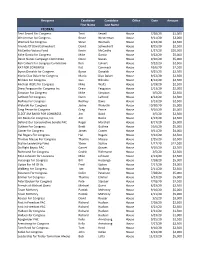
2020 PAC Contributions.Xlsx
Recipient Candidate Candidate Office Date Amount First Name Last Name FEDERAL Terri Sewell For Congress Terri Sewell House 7/28/20 $1,000 Westerman for Congress Bruce Westerman House 9/11/20 $3,000 Womack for Congress Steve Womack House 9/22/20 $2,500 Friends Of David Schweikert David Schweikert House 8/25/20 $2,500 McCarthy Victory Fund Kevin McCarthy House 1/27/20 $20,000 Mike Garcia for Congress Mike Garcia House 9/22/20 $5,000 Devin Nunes Campaign Committee Devin Nunes House 9/10/20 $5,000 Ken Calvert For Congress Committee Ken Calvert House 9/22/20 $2,500 KAT FOR CONGRESS Kat Cammack House 10/6/20 $2,500 Byron Donalds for Congress Byron Donalds House 9/25/20 $2,500 Mario Diaz‐Balart for Congress Mario Diaz‐Balart House 9/22/20 $2,500 Bilirakis For Congress Gus Bilirakis House 8/14/20 $2,500 Michael Waltz for Congress Mike Waltz House 3/19/20 $2,500 Drew Ferguson for Congress Inc. Drew Ferguson House 2/13/20 $2,000 Simpson For Congress Mike Simpson House 3/5/20 $2,500 LaHood For Congress Darin LaHood House 8/14/20 $2,500 Rodney For Congress Rodney Davis House 3/13/20 $2,500 Walorski For Congress Jackie Walorski House 10/30/20 $5,000 Greg Pence for Congress Greg Pence House 9/10/20 $5,000 ELECT JIM BAIRD FOR CONGRESS Jim Baird House 3/5/20 $2,500 Jim Banks for Congress, Inc. Jim Banks House 2/13/20 $2,500 Defend Our Conservative Senate PAC Roger Marshall House 8/17/20 $5,000 Guthrie For Congress Brett Guthrie House 10/6/20 $5,000 Comer for Congress James Comer House 9/11/20 $4,000 Hal Rogers For Congress Hal Rogers House 9/22/20 $2,500 -

Contest County Name Party Mailing Address Email / Web Phone
Contest County Name Party Mailing Address Email / Web Phone Representative in Congress Kelly Armstrong Republican 1515 Burnt Boat Dr Ste C #112 [email protected] (701) 471-6036 Bismarck ND 58503 armstrongnd.com Representative in Congress Steven James Peterson Libertarian 2808 HICKORY ST N [email protected] (701) 936-4362 FARGO ND 58102-1715 stevenjamespeterson.com Representative in Congress Zach Raknerud Democratic-NPL 304 5th St NW [email protected] Minot ND 58703 https://www.ZachForND.com Representative in Congress Roland Clifford Riemers Democratic-NPL 1024 UNIVERSITY AVE [email protected] (701) 317-1803 PO Box 14702 GRAND FORKS ND 58208 State Senator David S Rust Republican PO BOX 1198 [email protected] (701) 216-0270 District 02 TIOGA ND 58852-1198 State Senator Lisa Finley-DeVille Democratic-NPL 13 1ST AVE NE (701) 421-8020 District 04 PO Box 501 MANDAREE ND 58757 State Senator Jordan Kannianen Republican 8011 51ST ST NW [email protected] (701) 421-8813 District 04 STANLEY ND 58784-9562 State Senator Morris Holen Jr Democratic-NPL PRAIRIE VIEW ACRES #8 [email protected] (701) 228-3345 District 06 BOTTINEAU ND 58318 State Senator Shawn Vedaa Republican PO BOX 550 (701) 721-5346 District 06 VELVA ND 58790-0550 State Senator Howard C Anderson Jr Republican 2107 7TH ST NW [email protected] (701) 448-2235 District 08 TURTLE LAKE ND 58575-9667 State Senator Charlie Hart Democratic-NPL 15983 100TH ST NE (701) 520-2750 District 10 PEMBINA ND 58271-9712 State Senator Janne Myrdal Republican PO Box 153 (701) 331-0946 -

2019 NORTH DAKOTA LEGISLATIVE REPORT CARD 66Th LEGISLATIVE SESSION DEAR FRIENDS
2019 NORTH DAKOTA LEGISLATIVE REPORT CARD 66th LEGISLATIVE SESSION DEAR FRIENDS, I am pleased to share this report card for the most recent North Dakota state legislative session. Here is a snapshot of how lawmakers voted on key social and moral legislation related to the right to life, education, family, marriage and other issues. Guided by our mission of building a state where God is honored, religious liberty flourishes, families thrive, and life is cherished, this report card focuses on seven bills/resolutions (hereafter collectively called bills) in the North Dakota Senate and House of Representatives during the 2019 Legislative Session. All these are included in this report card. A bill is passed by a simple majority in the Senate (24 votes out of 47 senators) and the House (48 votes out of 94 Representatives.) Lawmakers earned percentage grades ranging from 0% to 100%, based on how they voted on the relevant bills coming before their chamber. This report card is not an endorsement of any candidate or political party. It does not measure any lawmakers’ integrity, commitment to their faith, work ethic, or rapport with Family Policy Alliance of North Dakota. It is only a report on how each lawmaker voted. One of the most common questions people ask is, “How did my legislator vote?” This report card should help you answer that question. Sincerely, Mark Jorritsma Executive Director, Family Policy Alliance of North Dakota CONTENTS Introduction Letter 2 About the Report Card 3 Bill and Resolution Descriptions 4 Legislator Votes 5-7 – 2 – ABOUT THE REPORT CARD Family Policy Alliance of North Dakota selected votes on key legislation from the North Dakota Senate and North Dakota House of Representatives based on our core belief in promoting, protecting, and strengthening traditional family values. -

House of Rep Daily Journal
Page 1 1st DAY TUESDAY, DECEMBER 1, 2020 1 Organizational and Orientation Session December 1, 2, 3, 2020 JOURNAL OF THE HOUSE Sixty-seventh Legislative Assembly * * * * * Bismarck, December 1, 2020 The House convened at 1:00 p.m., with Speaker Klemin presiding. The prayer was offered by Pastor Keith Ritchie, Cornerstone Community Church, Bismarck. COMMUNICATION FROM SECRETARY OF STATE ALVIN A. JAEGER December 1, 2020 In accordance with Section 54-03-03 of the North Dakota Century Code, I certify the attached list is a true and correct record of individuals elected to the Office of State Representative in the General Election held on November 3, 2020. The results of the election were certified by the State Canvassing Board on November 13, 2020. Then, as authorized in Section 16.1-15-45 of the North Dakota Century Code, Certificates of Election were prepared by the Secretary of State and signed by the Governor, the Clerk of the Supreme Court (as the designated representative of the State Canvassing Board), and the Secretary of State. A Certificate of Election was issued to each of the newly elected members of the legislative assembly, as directed in Section 16.1-15-46 of the North Dakota Century Code. In addition, as required by Section 4, Article XI, of the North Dakota Constitution, an Oath of Office (or affirmation) form was provided to each Representative, with instructions to execute the Oath before a Notary Public and file it with the Secretary of State before he or she assumes the duties of their office. IN TESTIMONY WHEREOF, I have set my hand and affixed the Great Seal of the State of North Dakota at the Capitol in the City of Bismarck on this date. -

Great Plains TRAC Sept. 2019 Legislative Update
Great Plains TRAC Sept. 2019 Legislative Update Last Updated: October 07, 2019 The Great Plains Telehealth Resource Center provides telehealth technical assistance to the states of Wisconsin, Iowa, Minnesota, South Dakota, North Dakota, and Nebraska. A few notes about this report: 1. Bills are organized into specific telehealth "topic area". 2. The Fiscal Note (FN) Outlook: The left hand column indicates the bill's Pre-Floor Score, and the right hand column indicates the bill's actual Floor Score of the last chamber it was in (either Senate or House). 3. Regulations are listed at the end in order of their publication date. 4. If you would like to learn more about any piece of legislation or regulation, the bill numbers and regulation titles are clickable and link out to additional information. Bills by Topic Bills by Issue Broadband 0 Cross-State Licensi… 9 9 Demonstrations, … 20 20 Medicaid Reimbur… 2 2 Medicare Reimbur… 0 Network Adequacy 1 1 Online Prescribing 6 Other 7 7 5 - Introduced Private Payer Rei… 1 1 1 - Passed First Chamber Provider-Patient R… 5 5 Regulatory, Licensi… 12 12 1 - Failed Substance Use Dis… 3 3 39 - Failed Sine Die 0 10 20 30 12 - Enacted High Medium Low None All Bills Cross-State Licensing (9) State Bill Number Last Action Status Position Priority FN Outlook WI AB 438 Fiscal Estimate Received 2019 09 25 In Assembly None None 13.7% 76.3% Title Bill Summary: Ratifies the Physical Therapy Licensure Compact. ratification of the Physical Therapy Licensure Compact, extending the time limit for emergency rule procedures, providing an exemption from emergency rule procedures, and granting rule- making authority. -

To View Entire Sample Ballot
11 STATE OF NORTH DAKOTA BURLEIGH COUNTY GENERAL ELECTION BALLOT NOVEMBER 3, 2020 To vote for the candidate of your choice, State Senator you must darken the oval ( ) next to the Governor and Lt. Governor name of that candidate. District 32 Vote for no more than ONE Vote for no more than ONE name set of names To vote for a person whose name is not 21 printed on the ballot, you must darken the Dick Dever Doug Burgum and oval ( ) next to the blank line provided Republican Party Brent Sanford and write that person's name on the blank Amelia Doll Republican Party line. Democratic-NPL Party PARTY BALLOT DuWayne Hendrickson and Joshua Voytek Libertarian Party President and Vice President State Representative District 08 of the United States Vote for no more than TWO names Shelley Lenz and Vote for no more than ONE name Ben Vig Linda Babb Democratic-NPL Party Presidential Electors Democratic-NPL Party Sandy J Boehler Dave Nehring Trump Ray Holmberg Republican Party Republican Party Robert Wefald Kathrin Volochenko Democratic-NPL Party Dustin Gawrylow David Andahl State Auditor Jorgensen Martin J Riske Republican Party Vote for no more than ONE name Libertarian Party Dylan Stuckey 40 Patrick Hart Democratic-NPL Party 41 Heidi Heitkamp Joshua C Gallion Biden Bernice Knutson Republican Party Democratic-NPL Party Warren Larson 42 State Representative District 28 State Treasurer 43 Vote for no more than TWO names Vote for no more than ONE name Mike Brandenburg Mark Haugen Republican Party Democratic-NPL Party Rebecca (Beckie) Phillips Thomas Beadle -

353 Bills / Regs.)
Available Bills / Regulations (353 bills / regs.) Bill/Reg. # Categories Summary Status Alabama Vehicle Finance: Motor vehicles and motor fuels, Rebuild Ala. Act., add'l tax on gasoline and diesel fuel of ten cents in 03/12/2019 - HB 2x Registration increments, add'l licensing tax on electric and hybrid electric automobiles, distribution of proceeds for Signed by 2019 state, county, municipal, and State Port Authority transportation purposes, floor stock tax provided, bond Governor; Enacted Poole of motor fuel terminal operators increased, taxes increased based on changes in National Highway History Construction Cost Index, portion to finance improvements to ship channel related to Ala. St. Docks, ATRIP-II Committee estab., authorized to enter agreements for debt financing, Secs. 11-6-4, 11-6-23, 40- 12-242, 40-17-331 am'd.; Sec. 11-6-6 repealed Alabama Vehicle Finance: Clay Co. Community Corrections Program, director and employees, power of arrest under certain 05/13/2019 - HB 219 Towing/Impoundment conditions Signed by 2019 Governor; Enacted Pringle History Alabama Vehicle Finance: Revenue Dept., agents of, further provided to include bonded title service providers, Secs. 32-8-2, 32-8- 05/23/2019 - HB 222 Franchise, Licensing, Titling 3, 32-8-34 am'd. Signed by 2019 & Liens Governor; Enacted Pettus History Alabama Vehicle Finance: Motor vehicles, Fleet vehicles, licensing and registration of, provided, Revenue Dept. required to 05/08/2019 - HB 278 Registration, Titling & Liens establish a fleet online tax system, Secs. 40-12-305 to 40-12-309, inclusive, added; Sec. 40-12-240 Signed by 2019 am'd. Governor; Enacted McCampbell History Alabama Vehicle Finance: Motor vehicle dealer licensing, master regulatory dealer license, provided, wholesale motor vehicle 05/23/2019 - HB 393 Franchise, Licensing, Titling auction license provided, Secs. -

ND Cropland Rents and Values Increase Modestly
Page 11 Mountrail County Promoter, Inc., Stanley, ND Wednesday, Apr. 21, 2021 want to leave that ultimate decision “Because it is under emergency North Dakota Weekly ND Universities Don’t Plan On up to our students, which is why the use doctrine it is not going to be a university isn’t requiring vaccina- requirement that we can foresee,” Gas Price Update Requiring COVID-19 Vaccine tions.” she said. “We are just going to con- North Dakota gas prices have Neighboring areas and their cur- By Dylan Sherman, “I think there are a lot of students Wilson added the numbers could tinue to follow guidelines from the risen 2.0 cents in the past week, av- rent gas prices: Sioux Falls- $2.76/g, NDNAEF and faculty that have, as soon as be higher from those who received a CDC.” eraging $2.76/g Monday, according down 0.4 cents per gallon from last Universities in North Dakota it has become available, gone and vaccine before the incentive or those Rostad said if certain universi- to GasBuddy’s daily survey of 493 week’s $2.77/g; Fargo- $2.78/g, up have required students to get certain gotten the vaccine,” he said. “It is who have not informed the school. ties wanted to require the vaccine, stations. Gas prices in North Dakota 5.9 cents per gallon from last week’s vaccines, but the COVID-19 vaccine probably similar to our society in She said the university does not it would have to be removed from are 2.6 cents per gallon lower than a $2.72/g; South Dakota- $2.82/g, up will not be one of them.