Glial Cells Shape Pathology and Repair After Spinal Cord Injury
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Individual Neuronal Subtypes Control Initial Myelin Sheath Growth and Stabilization Heather N
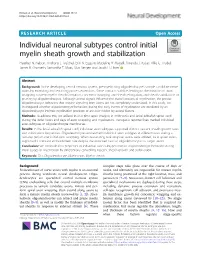
Nelson et al. Neural Development (2020) 15:12 https://doi.org/10.1186/s13064-020-00149-3 RESEARCH ARTICLE Open Access Individual neuronal subtypes control initial myelin sheath growth and stabilization Heather N. Nelson, Anthony J. Treichel, Erin N. Eggum, Madeline R. Martell, Amanda J. Kaiser, Allie G. Trudel, James R. Gronseth, Samantha T. Maas, Silas Bergen and Jacob H. Hines* Abstract Background: In the developing central nervous system, pre-myelinating oligodendrocytes sample candidate nerve axons by extending and retracting process extensions. Some contacts stabilize, leading to the initiation of axon wrapping, nascent myelin sheath formation, concentric wrapping and sheath elongation, and sheath stabilization or pruning by oligodendrocytes. Although axonal signals influence the overall process of myelination, the precise oligodendrocyte behaviors that require signaling from axons are not completely understood. In this study, we investigated whether oligodendrocyte behaviors during the early events of myelination are mediated by an oligodendrocyte-intrinsic myelination program or are over-ridden by axonal factors. Methods: To address this, we utilized in vivo time-lapse imaging in embryonic and larval zebrafish spinal cord during the initial hours and days of axon wrapping and myelination. Transgenic reporter lines marked individual axon subtypes or oligodendrocyte membranes. Results: In the larval zebrafish spinal cord, individual axon subtypes supported distinct nascent sheath growth rates and stabilization frequencies. Oligodendrocytes ensheathed individual axon subtypes at different rates during a two-day period after initial axon wrapping. When descending reticulospinal axons were ablated, local spinal axons supported a constant ensheathment rate despite the increased ratio of oligodendrocytes to target axons. Conclusion: We conclude that properties of individual axon subtypes instruct oligodendrocyte behaviors during initial stages of myelination by differentially controlling nascent sheath growth and stabilization. -

Whole-Organism Imaging of Spinal Motor Neurons and Musculature with the Cytation C10 Confocal Imaging Reader
Application Bulletin Whole-Organism Imaging of Spinal Motor Neurons and Musculature with the Cytation C10 Confocal Imaging Reader Introduction Zebrafish have long held an essential oler in developmental biology research due to their many and often cited advantages, both biological and practical. Recently, zebrafish amenability to genome editing techniques such as CRISPR, high-throughput screening, and predictive value in drug discovery toxicol- ogy studies1, combined with their exceptional accessibility to optogenetic manipulation and live-imaging techniques highlight the essential place zebrafish have in the toolkit of health-driven research. Indeed, zebrafish are lowering the barrier toin vivo research of devastating neurodegenerative diseases, such as amyotrophic lateral sclerosis (ALS, also known as Lou Gehrig’s disease)2, as their complete spinal neuron and muscle unit organization is entirely accessible to observation through light microscopy. This application bulletin demonstrates the capability of whole-organism imaging on the newly intro- duced BioTek Cytation C10 confocal imaging reader, with a focus on spinal motor neurons, neuromus- cular synapses, and musculature of the zebrafish model organism. The optical sectioning of the spin- ning disk confocal system is essential to resolving the deep tissue structures, such as the fine neuronal processes, and provides a literal clearer view of subcellular details when imaging thick samples. Materials and Methods Key Words: Unless otherwise noted, all chemicals were obtained from Sigma Aldrich (St. Louis, MO). General main- tenance of zebrafish followed established methods3. Wild-type male and female Danio rerio were main- Confocal Microscopy tained at 28 °C on a 14/10 hour light/dark cycle. Adults were crossed and eggs promptly collected in Optical Sectioning EM3 media4. -

Motor Circuits in Action: Specification, Connectivity, and Function
Neuron Review Motor Circuits in Action: Specification, Connectivity, and Function Silvia Arber1,2,* 1Biozentrum, Department of Cell Biology, University of Basel, Klingelbergstrasse 70, 4056 Basel, Switzerland 2Friedrich Miescher Institute for Biomedical Research, Maulbeerstrasse 66, 4058 Basel, Switzerland *Correspondence: [email protected] DOI 10.1016/j.neuron.2012.05.011 Mammalian motor behavior is enabled by a hierarchy of interleaved circuit modules constructed by interneu- rons in the spinal cord, sensory feedback loops, and bilateral communication with supraspinal centers. Neuronal subpopulations are specified through a process of precisely timed neurogenesis, acquisition of transcriptional programs, and migration to spatially confined domains. Developmental and genetic programs instruct stereotyped and highly specific connectivity patterns, binding functionally distinct neuronal subpop- ulations into motor circuit modules at all hierarchical levels. Recent work demonstrates that spatial organi- zation of motor circuits relates to precise connectivity patterns and that these patterns frequently correlate with specific behavioral functions of motor output. This Review highlights key examples of how develop- mental specification dictates organization of motor circuit connectivity and thereby controls movement. Introduction Through specific perturbations of functional or genetic differen- Movement is generated by the activity of neuronal circuits tiation programs in defined neuronal populations, recent studies collecting and integrating -

Glia Are a Unique Substrate for the in Vitro Growth of Central Nervous System Neurons1
0270.6474/84/0407-1892$02.00/O The Journal of Neuroscience Copyright 0 Society for Neuroscience Vol. 4, No. 7, pp. 1892-1903 Printed in U.S.A. July 1984 GLIA ARE A UNIQUE SUBSTRATE FOR THE IN VITRO GROWTH OF CENTRAL NERVOUS SYSTEM NEURONS1 MARK NOBLE,*s2 JUIN FOK-SEANG,$ AND 31M COHENS * Department of Clinical Neurology, Institute of Neurology, London WClN 3BG, England and $ Medical Research Council Neuroimmunology Project, Department of Zoology, University College London, London WClE 6BT, England Received July 6,1983; Revised November 29, 1983; Accepted February 7, 1984 Abstract We have examined the consequences of surface interactions with glial and nonglial cells on the in vitro growth of CNS neurons. When cerebellar or spinal cord cells were plated onto monolayers highly enriched in cortical astrocytes or sciatic nerve Schwann cells, neurons generally grew as single cells and showed relatively little tendency to aggregate. Similarly, neurites showed little tendency to fasciculate. In contrast, when plated onto fibroblast, heart muscle-fibroblast, or astrocyte-free meningeal monolayers, neurons rapidly aggregated, and neurite outgrowth was primarily in large fascicles. There were no glia detectable in the majority of aggregates or fascicles, suggesting that aggregation and fasciculation were due to interactions between neurons. Neurite outgrowth over 24 hr was also greater on astrocytes than on nonglia. Whether or not aggregation and fasciculation occurred was due to surface properties of the glial and nonglial cells. When neurons were added to astrocyte and nonglial monolayers growing in medium conditioned by a large excess of co-cultured nonglia or astrocytes, respectively, the pattern of neuronal growth was determined by the type of monolayer with which the neurons were in contact. -
Relating Reflex Gain Modulation in Posture Control to Underlying Neural Network Properties Using a Neuromusculoskeletal Model
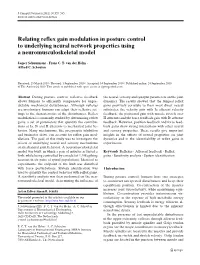
J Comput Neurosci (2011) 30:555–565 DOI 10.1007/s10827-010-0278-8 Relating reflex gain modulation in posture control to underlying neural network properties using a neuromusculoskeletal model Jasper Schuurmans · Frans C. T. van der Helm · Alfred C. Schouten Received: 25 March 2010 / Revised: 1 September 2010 / Accepted: 14 September 2010 / Published online: 24 September 2010 © The Author(s) 2010. This article is published with open access at Springerlink.com Abstract During posture control, reflexive feedback the neural, sensory and synaptic parameters on the joint allows humans to efficiently compensate for unpre- dynamics. The results showed that the lumped reflex dictable mechanical disturbances. Although reflexes gains positively correlate to their most direct neural are involuntary, humans can adapt their reflexive set- substrates: the velocity gain with Ia afferent velocity tings to the characteristics of the disturbances. Reflex feedback, the positional gain with muscle stretch over modulation is commonly studied by determining reflex II afferents and the force feedback gain with Ib afferent gains: a set of parameters that quantify the contribu- feedback. However, position feedback and force feed- tions of Ia, Ib and II afferents to mechanical joint be- back gains show strong interactions with other neural havior. Many mechanisms, like presynaptic inhibition and sensory properties. These results give important and fusimotor drive, can account for reflex gain mod- insights in the effects of neural properties on joint ulations. The goal of this study was to investigate the dynamics and in the identifiability of reflex gains in effects of underlying neural and sensory mechanisms experiments. on mechanical joint behavior. -

Synaptic Transmission Between Dorsal Root Ganglion and Dorsal
0270.6474/85/0508~2281$02.00/0 The Journal of Neuroscrence Copyright 0 Society for Neuroscrence Vol. 5, No 8, pp. 2281-2289 Printed rn U S.A. August 1985 Synaptic Transmission between Dorsal Root Ganglion and Dorsal Horn Neurons in Culture: Antagonism of Monosynaptic Excitatory Postsynaptic Potentials and Glutamate Excitation by Kynurenate’ C. E. JAHR AND T. M. JESSELL* Department of Neurobiology, Harvard Medical School, Boston, Massachusetts 02115 Abstract Randic, 1984). Several lines of evidence suggest that the fast EPSPs in spinal cord neurons evoked by primary afferent stimulation are intracellular recording techniques have been used to pro- mediated by L-glutamate or by compounds with similar postsynaptic vide information on the identity of excitatory sensory trans- actions. lontophoretic and pressure applications of L-glutamate de- mitters released at synapses formed between dorsal root polarize the majority of mammalian spinal neurons in vivo and in ganglion (DRG) and dorsal horn neurons maintained in cell vitro (Ransom et al., 1977b; Watkins and Evans, 1981; Salt and Hill, culture. Explants of embryonic rat DRG were added to dis- 1983) with a reversal potential (Mayer and Westbrook, 1984) similar sociated cultures of embryonic dorsal horn neurons and to that of the EPSP evoked by dorsal root ganglion (DRG) neuron synaptic potentials were recorded intracellularly from dorsal stimulation (Engberg and Marshall, 1979; Finkel and Redman, 1983; horn neurons after DRG explant stimulation. More than 80% MacDonald et al., 1983). Biochemical analysis has demonstrated a of dorsal horn neurons within 1 mm of DRG explants received higher concentration of L-glutamate in dorsal than in ventral roots at least one fast, DRG-evoked, monosynaptic input. -

Computational Models of Populations of Motor Neurons
Computational Models of Populations of Motor Neurons Jakob L. Dideriksen and Dario Farina Department of Neurorehabiliation Engineering, Bernstein Focus Neurotechnology Göttingen, Bernstein Center for Computational Neuroscience, Universitätsmedizin Göttingen, Göttingen, Germany 1 OBJECTIVES each of the objectives determined how the various sub-models were implemented. In this paper, we will provide examples of how computational models of motor neuron and muscle 2.1 Neuromechanical Models activity can support basic and applied research on human movement. Both examples focus on The model was designed to reflect the characteristics pathological tremor. Tremor is a rhythmic, of an antagonist muscle pair acting on one limb in involuntary oscillation of a limb and it is the most one degree of freedom and consisted of a number of prevalent movement disorder, symptomatic to e.g. sub-models interacting via one or more variables. Parkinson’s Disease (Wenning et al., 2005). Tremor First, the activity of the motor neuron population implies a serious worsening of the quality of life, (spike trains) was determined based on the synaptic also because the effect of the current treatments is input it received. Each motor neuron innervated a set variable(Rascol et al., 2000). of muscle fibers (the motor unit). Each motor unit First, we show how models can be applied in the was assigned a set of parameters describing its development of a rehabilitation device for contractile properties. Along with these properties, suppressing pathological tremor (Objective 1). The the discharge rate determined the motor unit force. proposed tremor rehabilitation system relied on The force of the muscles (the sum of the force modulation of spinal neuron excitability of the generated by all motor units) evoked the movement tremorogenic motor neurons using homonymous of the limb. -

A Single Cell Atlas of Spared Tissue Below a Spinal Cord Injury Reveals Cellular Mechanisms of Repair
bioRxiv preprint doi: https://doi.org/10.1101/2021.04.28.441862; this version posted April 29, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. This article is a US Government work. It is not subject to copyright under 17 USC 105 and is also made available for use under a CC0 license. 1 A Single Cell Atlas of Spared Tissue Below a Spinal Cord Injury Reveals Cellular Mechanisms of Repair 2 Kaya J.E. Matson1, Daniel E. Russ2, Claudia Kathe3,4, Dragan Maric5, Isabelle Hua1, Jonathan Krynitsky6, 3 Randall Pursley6, Anupama Sathyamurthy1,7, Jordan W. Squair3,4, Gregoire Courtine3,4, Ariel J. Levine1,* 4 5 1Spinal Circuits and Plasticity Unit, National Institute of Neurological Disorders and Stroke, National Institutes of Health, 6 Bethesda, MD, USA 7 2 Division of Cancer Epidemiology and Genetics, Data Science Research Group, National Cancer Institute, NIH, Rockville, MD, 8 USA 9 3 Center for Neuroprosthetics and Brain Mind Institute, Faculty of Life Sciences, École Polytechnique Fédérale de Lausanne 10 (EPFL), Lausanne, Switzerland 11 4 NeuroRestore, Department of Clinical Neuroscience, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), 12 Lausanne, Switzerland 13 5 National Institute of Neurological Disorders and Stroke, Bethesda, MD, USA 14 6 Signal Processing and Instrumentation Section, Center for Information Technology, National Institutes of Health, Bethesda, 15 MD, USA 16 7 Present address: Centre for Neuroscience, Indian Institute of Science, Bangalore, India 17 18 *Corresponding Author: [email protected] 19 20 Abstract: 21 After spinal cord injury (SCI), the “spared” tissue below the lesion contains undamaged cells that could 22 support or augment recovery, but targeting these cells requires a clearer understanding of their injury 23 responses and capacity for repair. -
Dynamic Regulation of the Cholinergic System in the Spinal Central Nervous System M
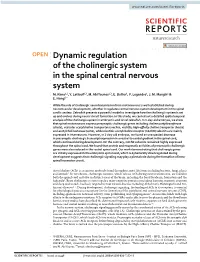
www.nature.com/scientificreports OPEN Dynamic regulation of the cholinergic system in the spinal central nervous system M. Rima1,2, Y. Lattouf1,3, M. Abi Younes1,3, E. Bullier1, P. Legendre1, J. M. Mangin1 & E. Hong1* While the role of cholinergic neurotransmission from motoneurons is well established during neuromuscular development, whether it regulates central nervous system development in the spinal cord is unclear. Zebrafsh presents a powerful model to investigate how the cholinergic system is set up and evolves during neural circuit formation. In this study, we carried out a detailed spatiotemporal analysis of the cholinergic system in embryonic and larval zebrafsh. In 1-day-old embryos, we show that spinal motoneurons express presynaptic cholinergic genes including choline acetyltransferase (chata), vesicular acetylcholine transporters (vachta, vachtb), high-afnity choline transporter (hacta) and acetylcholinesterase (ache), while nicotinic acetylcholine receptor (nAChR) subunits are mainly expressed in interneurons. However, in 3-day-old embryos, we found an unexpected decrease in presynaptic cholinergic transcript expression in a rostral to caudal gradient in the spinal cord, which continued during development. On the contrary, nAChR subunits remained highly expressed throughout the spinal cord. We found that protein and enzymatic activities of presynaptic cholinergic genes were also reduced in the rostral spinal cord. Our work demonstrating that cholinergic genes are initially expressed in the embryonic spinal cord, which is dynamically downregulated during development suggests that cholinergic signaling may play a pivotal role during the formation of intra- spinal locomotor circuit. Acetylcholine (ACh) is an ancient molecule found throughout most life forms including bacteria, fungi, plants and animals1. In vertebrates, cholinergic neurons, which release ACh during neurotransmission, are found in both the spinal cord and also in distinct areas of the brain, including the basal forebrain, brainstem and the habenula2. -

The Role of Satellite Glial Cells, Astrocytes, and Microglia in Oxaliplatin-Induced Neuropathic Pain
biomedicines Review The Role of Satellite Glial Cells, Astrocytes, and Microglia in Oxaliplatin-Induced Neuropathic Pain Ji Hwan Lee and Woojin Kim * Department of Physiology, College of Korean Medicine, Kyung Hee University, Seoul 02453, Korea; [email protected] * Correspondence: [email protected]; Tel.: +82-2-961-0334 Received: 15 August 2020; Accepted: 31 August 2020; Published: 2 September 2020 Abstract: Oxaliplatin is a third-generation platinum-based chemotherapeutic drug. Although its efficacy against colorectal cancer is well known, peripheral neuropathy that develops during and after infusion of the agents could decrease the quality of life of the patients. Various pathways have been reported to be the cause of the oxaliplatin-induced paresthesia and dysesthesia; however, its mechanism of action has not been fully understood yet. In recent years, researchers have investigated the function of glia in pain, and demonstrated that glia in the peripheral and central nervous system could play a critical role in the development and maintenance of neuropathic pain. These results suggest that targeting the glia may be an effective therapeutic option. In the past ten years, 20 more papers focused on the role of glia in oxaliplatin-induced thermal and mechanical hypersensitivity. However, to date no review has been written to summarize and discuss their results. Thus, in this study, by reviewing 23 studies that conducted in vivo experiments in rodents, the change of satellite glial cells, astrocytes, and microglia activation in the dorsal root ganglia, spinal cord, and the brain of oxaliplatin-induced neuropathic pain animals is discussed. Keywords: astrocytes; chemotherapy-induced neuropathic pain; glia; microglia; oxaliplatin 1. -

26 April 2010 TE Prepublication Page 1 Nomina Generalia General Terms
26 April 2010 TE PrePublication Page 1 Nomina generalia General terms E1.0.0.0.0.0.1 Modus reproductionis Reproductive mode E1.0.0.0.0.0.2 Reproductio sexualis Sexual reproduction E1.0.0.0.0.0.3 Viviparitas Viviparity E1.0.0.0.0.0.4 Heterogamia Heterogamy E1.0.0.0.0.0.5 Endogamia Endogamy E1.0.0.0.0.0.6 Sequentia reproductionis Reproductive sequence E1.0.0.0.0.0.7 Ovulatio Ovulation E1.0.0.0.0.0.8 Erectio Erection E1.0.0.0.0.0.9 Coitus Coitus; Sexual intercourse E1.0.0.0.0.0.10 Ejaculatio1 Ejaculation E1.0.0.0.0.0.11 Emissio Emission E1.0.0.0.0.0.12 Ejaculatio vera Ejaculation proper E1.0.0.0.0.0.13 Semen Semen; Ejaculate E1.0.0.0.0.0.14 Inseminatio Insemination E1.0.0.0.0.0.15 Fertilisatio Fertilization E1.0.0.0.0.0.16 Fecundatio Fecundation; Impregnation E1.0.0.0.0.0.17 Superfecundatio Superfecundation E1.0.0.0.0.0.18 Superimpregnatio Superimpregnation E1.0.0.0.0.0.19 Superfetatio Superfetation E1.0.0.0.0.0.20 Ontogenesis Ontogeny E1.0.0.0.0.0.21 Ontogenesis praenatalis Prenatal ontogeny E1.0.0.0.0.0.22 Tempus praenatale; Tempus gestationis Prenatal period; Gestation period E1.0.0.0.0.0.23 Vita praenatalis Prenatal life E1.0.0.0.0.0.24 Vita intrauterina Intra-uterine life E1.0.0.0.0.0.25 Embryogenesis2 Embryogenesis; Embryogeny E1.0.0.0.0.0.26 Fetogenesis3 Fetogenesis E1.0.0.0.0.0.27 Tempus natale Birth period E1.0.0.0.0.0.28 Ontogenesis postnatalis Postnatal ontogeny E1.0.0.0.0.0.29 Vita postnatalis Postnatal life E1.0.1.0.0.0.1 Mensurae embryonicae et fetales4 Embryonic and fetal measurements E1.0.1.0.0.0.2 Aetas a fecundatione5 Fertilization -

Current Concepts
Clinical Review: Current Concepts Central Nervous System Reorganization in a Variety of Chronic Pain States: A Review Douglas E. Henry, MD, Anthony E. Chiodo, MD, Weibin Yang, MD Abstract: Chronic pain can develop from numerous conditions and is one of the most widespread and disabling health problems today. Unfortunately, the pathophysiology of chronic pain in most of these conditions, along with consistently effective treatments, remain elusive. However, recent advances in neuroimaging and neurophysiology are rapidly expanding our understanding of these pain syndromes. It is now clear that substantial functional and structural changes, or plasticity, in the central nervous system (CNS) are associated with many chronic pain syndromes. A group of cortical and subcortical brain regions, often referred to as the “pain matrix,” often show abnormalities on functional imaging studies in persons with chronic pain, even with different pain locations and etiologies. Changes in the motor and sensory homunculus also are seen. Some of these CNS changes return to a normal state with resolution of the pain. It is hoped that this knowledge will lead to more effective treatments or even new preventative measures. The purpose of this article is to review recent advances in the understanding of the CNS changes associated with chronic pain in a number of clinical entities encountered in the field of physical medicine and rehabilitation. These clinical entities include nonspecific low back pain, fibromyalgia, complex regional pain syndrome, postamputation phantom pain, and chronic pain after spinal cord injury. PM R 2011;3:1116-1125 INTRODUCTION Central nervous system (CNS) plasticity refers to the ability of the CNS to reorganize over time.