The 50 Peaks That ‘Changed My Life’
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

FINAL Kimball 16-Page Marketing Piece.Indd
Kimball Welcomes You! As seen in the March/April 2008 issue of Nebraska Life MagazineKIMBALL. WELCOMES YOU School HOPE THAT THE FOLLOWING feature story, pictures and ads will be Superintendent of Schools helpful in familiarizing yourself with Kimball and our citizens. Since 1889, Troy L. Unzicker the town of Kimball has welcomed both travelers and settlers into the warm 901 S. Nadine St. embrace of its friendly and welcoming community nestled in the far southwestern Kimball, NE 69145 corner of Nebraska. (308) 235-2188 Safely secured under the brightest stars and the most spectacular sunsets, Kim- Fax: (308) 235-3269 ball has emerged as one of the most desirable destinations to live, work, raise a [email protected] family, retire and even start a business in the Great Plains. http://kimball.k12.ne.us Th ere’s so much to like about Kimball. Its natural, rural beauty. Close proximity to the Colorado Front Range, Interstate 80 and the future Heartland Expressway City make our location a huge attribute. City of Kimball Administrator Harold Farrar • Healthy living. 223 S. Chestnut St. Hospital University of • Top notch health care facilities. Kimball, NE 69145 Kimball Health Services Nebraska Extension • Assisted living and nursing home that are second to none. (308) 235-3639 or 235-2971 Julie Schnell - Chief Kimball-Banner Co. • Excellent schools. [email protected] Executive Offi cer Extension Offi ce • Welcoming churches. www.ci.kimball.ne.us 505 S. Burg St. 209 E. 3rd St. Kimball, NE 69145 • Unique shopping. Kimball, NE 69141-1401 (308) 235-1951 Hospital • Rich rail history and presence Economic (308) 235-3122 (308) 235-1966 Clinic (308) 235-3077 • Many dining options. -

Kimball Nebraska!
Kimball The High Point of Nebraska PC: Alisa Danae Photography Located at: 214 S Walnut St Kimball, Nebraska Phone: (308) 230-2111 Hours: Tuesday—Thursday (6:00 AM—2:00 PM) Friday & Saturday (6:00 AM— 8:00 PM) Karen’s Kitchen is a locally owned and operated family restaurant Offering Home cooked meals from the menu and daily specials. Karen’s Kitchen also offers pickup services. Table of Contents Quick Reference Phone Numbers Welcome Message History of Kimball Wheat Growers Hotel City of Kimball Government & Ordinances Agriculture in Kimball County Kimball Health Services Housing Utilities Education Oliver Reservoir State Recreation Area Four Winds Golf Course Gotte Park Panorama Point & Three State Corner Marker Plains Historical Museum Kimball Celebrations Kimball Organizations Transportation City of Kimball Map Kimball Businesses Quick Reference Phone Numbers Kimball City Offices…………………….308.235.3639 County Assessor………………...……….308.235.2362 County Attorney………………….....…..308.235.3678 County Clerk……………………………….308.235.2241 County Commissioners..……………....308.235.4056 County Court………..………………….....308.235.2831 County District Court………………...308.235.3591 County Highway Department……...308.235.2681 County Treasurer…………………...…..308.235.2242 District 10 Probation Office….…...308.235.4046 Fairgrounds………………………………...308.235.8886 Kimball Health Services……………..308.235.1952 Kimball Landfill...……………………….308.235.3540 Kimball Municipal Airport……........308.235.4008 Kimball Parks & Recreation…….....308.235.4241 Kimball Police Department..……....308.235.3608 -

Mount Rainier National Park, Washington
NATIONAL PARK . WASHINGTON MOUNT RAINIER WASHINGTON CONTENTS "The Mountain" 1 Wealth of Gorgeous Flowers 3 The Forests 5 How To Reach the Park 8 By Automobile 8 By Railroad and Bus 11 By Airplane 11 Administration 11 Free Public Campgrounds 11 Post Offices 12 Communication and Express Service 12 Medical Service 12 Gasoline Service 12 What To Wear 12 Trails 13 Fishing 13 Mount Rainier Summit Climb 13 Accommodations and Expenses 15 Summer Season 18 Winter Season 18 Ohanapecosh Hot Springs 20 Horseback Trips and Guide Service 20 Transportation 21 Tables of Distances 23 Principal Points of Interest 28 References 32 Rules and Regulations 33 Events of Historical Importance 34 Government Publications 35 UNITED STATES DEPARTMENT OF THE INTERIOR • Harold L. Ickes, Secretary NATIONAL PARK SERVICE Arno B. Cammerer, Director UNITED STATES GOVERNMENT PRINTING OFFICE • 1938 AN ALL-YEAR PARK Museums.—The park museum, headquarters for educational activities, MOUNT RAINIER NATIONAL PARK may be fully enjoyed throughout the and office of the park naturalist are located in the museum building at year. The summer season extends from early June to early November; the Longmire. Natural history displays and wild flower exhibits are main winter ski season, from late November well into May. All-year roads make tained at Paradise Community House, Yakima Park Blockhouse, and the park always accessible. Longmire Museum. Nisquaiiy Road is open to Paradise Valley throughout the year. During Hikes from Longmire.—Free hikes, requiring 1 day for the round trip the winter months this road is open to general traffic to Narada Falls, 1.5 are conducted by ranger naturalists from the museum to Van Trump Park, miles by trail from Paradise Valley. -

Geography and Environment
Section 6 Geography and Environment This section presents a variety of informa- In a joint project with the U.S. Census tion on the physical environment of the Bureau, during the 1980s, the USGS pro- United States, starting with basic area vided the basic information on geo- measurement data and ending with cli- graphic features for input into a national matic data for selected weather stations geographic and cartographic database around the country. The subjects covered prepared by the Census Bureau, called between those points are mostly con- TIGER® database. Since then, using a vari- cerned with environmental trends but ety of sources, the Census Bureau has include related subjects such as land use, updated these features and their related water consumption, air pollutant emis- attributes (names, descriptions, etc.) and sions, toxic releases, oil spills, hazardous inserted current information on the waste sites, municipal waste and recy- boundaries, names, and codes of legal cling, threatened and endangered wildlife, and statistical geographic entities; very and the environmental industry. few of these updates added aerial water features. Maps prepared by the Census The information in this section is selected Bureau using the TIGER® database show from a wide range of federal agencies the names and boundaries of entities and that compile the data for various adminis- are available on a current basis. trative or regulatory purposes, such as the Environmental Protection Agency An inventory of the nation’s land (EPA), U.S. Geological Survey (USGS), resources by type of use/cover was con- National Oceanic and Atmospheric Admin- ducted by the National Resources Inven- istration (NOAA), Natural Resources Con- tory Conservation Services (NRCS) every 5 servation Service (NRCS), and General Ser- years beginning in 1977 through 1997. -
PRINT 48-Peak Challenge
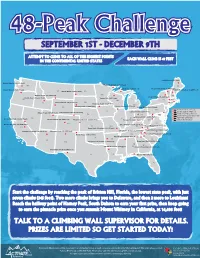
48-Peak Challenge SEPTEMBER 1ST - DECEMBER 9TH ATTEMPT TO CLIMB TO ALL OF THE HIGHEST POINTS EACH WALL CLIMB IS 47 FEET IN THE CONTINENTAL UNITED STATES Katahdin (5,268 feet) Mount Rainier (14,411 feet) WA Eagle Mountain (2,301 feet) ME Mount Arvon (1,978 feet) Mount Mansfield (4,393 feet) Mount Hood (11,239 feet) Mount Washington (6,288 feet) MT White Butte (3,506 feet) ND VT MN Granite Peak (12,799 feet) NH Mount Marcy (5,344 feet) Borah Peak (12,662 feet) OR Timms Hill (1,951 feet) WI NY MA ID Gannett Peak (13,804 feet) SD CT Hawkeye Point (1,670 feet) RI MI Charles Mount (1,235 feet) WY Harney Peak (7,242 feet) Mount Davis (3,213 feet) PA CT: Mount Frissell (2,372 feet) IA NJ DE: Ebright Azimuth (442 feet) Panorama Point (5,426 feet) Campbell Hill (1,549 feet) Kings Peak (13,528 feet) MA: Mount Greylock (3,487 feet) NE OH MD DE MD: Backbone Mountain (3360 feet) Spruce Knob (4,861 feet) NV IN NJ: High Point (1,803 feet) Boundary Peak (13,140 feet) IL Mount Elbert (14,433 feet) Mount Sunflower (4,039 feet) Hoosier Hill (1,257 feet) WV RI: Jerimoth Hill (812 feet) UT CO VA Mount Whitney (14,498 feet) Black Mountain (4,139 feet) KS Mount Rogers (5,729 feet) CA MO KY Taum Sauk Mountain (1,772 feet) Mount Mitchell (6,684 feet) Humphreys Peak (12,633 feet) Wheeler Peak (12,633 feet) Clingmans Dome (6,643 feet) NC Sassafras Mountain (3,554 feet) Black Mesa (4,973 feet) TN Woodall Mountain (806 Feet) OK AR SC AZ NM Magazine Mountain (2,753 feet) Brasstown Bald (4,784 feet) GA AL Driskill Mountain (535MS feet) Cheaha Mountain (2,405 feet) Guadalupe Peak (8,749 feet) TX LA Britton Hill (345 feet) FL Start the challenge by reaching the peak of Britton Hill, Florida, the lowest state peak, with just seven climbs (345 feet). -

YOSEMITE National Park
YOSEMITE National Park UNITED STATES RAILROAD ADMINISTRATION N AT IONAL PARK. SERIES Glacier Point, Yosemite Valley. The Half Dome in background Pa£e two An Appreciation of Yosemite NationalPark By HARRIET MONROE, Editor of "Poetry, a Magazine of Verse" Written Especially for the United Slates Railroad Administration WICE—and each time through an entire July—I have tramped with the California Sierra Club through the grandest areas of the Yosemite National Park. I have camped in the Valley, in Tuolumne Meadows, and in the lost Hetch-Hetchy—sleeping to the sound of rushing waters with mountains towering around me. I have crossed Vogelsang Pass when the mountain hemlocks were just slipping off their wet mantles of snow; I have descended the formidable Tuolumne Canyon past the third fall; and under Mount Dana I have looked down over the red rocks of Bloody Canyon to Lake Mono, lying incredibly blue among the pink and lilac craters of dead volcanoes. My memories of this prismatically shattered earth are sharp in details of beauty, but all of them rise against white granite and falling waters. Never anywhere else can there be mountains so silver-white—El Capitan shouldering the sky, Cloud's Rest and the two great Domes giving back the sun, and Ritter, Lyell and Dana, fierce and jagged, guarding their inscrutable heights. And through the crevices of this gleaming granite run everywhere crystal streams—streams mad with joy that foam as they fly, and shout as they take enormous leaps over stark precipices. All kinds of falling waters—the delicate cascades of Illilouette; the wind-blown tulle of Bridal Veil; Nevada, lacy, white-fingered, taking her 600-foot leap like a step in a dance; Vernal, broad-shouldered, strong-bodied, massive, as he jumps like an athlete; and, most wonder ful of all, Yosemite, that Upper Yosemite Fall whose leap is 1,500 feet — a tall white living figure against the formidable cliff, a figure moving and breathing, tossing the spray from his eyes, shining tall and straight there like a young Greek god. -
Todd-Huston-Speech-Book.Pdf
MORE THAN MOUNTAINS The Speech Edited transcription of Todd Huston’s speech Editor Julie Dunbar Huston Copyright 2018 Todd Huston LLC Forward The beauty from the mountaintop can be a very spiritual experience, and very symbolic of our life journey. We all have greatness within us – it’s how we are created. Eventually we live that greatness, and it’s the most brilliant light we could ever imagine. It beams through all darkness, not only in our lives, but the lives of those with whom we come into contact, and even those upon whom our thoughts rest. Getting to that point can seem like quite a hike up a strenuous mountainside, because throughout our journey we cram our packs full of some dark and unnecessary debris. This debris may take the form of negativity others have said about us that we can’t seem to shake off. It may take the form of abuse we have suffered. We may find we have taken on an unfavorable and unhealthy self-image. The debris may even come in the form of impatience, anger, or greed, which don’t seem terribly harmful; however, these are the most toxic because we feel justified in holding these thoughts toward ourselves or others. But none of this has anything to do with our true selves and the greatness and light we all are. In fact, it’s the opposite of our true identity and will only shroud our light in empty darkness. The more we unload our pack of this vile debris and toss it to the wind the easier becomes our ascent, until we finally let go of every false suggestion about who we are, recognize our true, beautiful identity, and reach that incredible summit. -

Mount Rainier National Park Visitor Study Summer 2012
National Park Service U.S. Department of the Interior Natural Resource Stewardship and Science Mount Rainier National Park Visitor Study Summer 2012 Natural Resource Report NPS/NRSS/EQD/NRR—2013/376 ON THE COVER Small pond in the Tatoosh Range, Mount Rainier National Park Photograph courtesy of Mount Rainier National Park Mount Rainier National Park Visitor Study Summer 2012 Natural Resource Report NPS/NRSS/EQD/NRR—2013/376 Manni, M. F., Yen Le, Steven J. Hollenhorst Visitor Services Project Park Studies Unit College of Natural Resources University of Idaho 875 Perimeter Drive MS 1139 Moscow, ID 83844-1139 November 2013 U.S. Department of the Interior National Park Service Natural Resource Stewardship and Science Fort Collins, Colorado Mount Rainier National Park – VSP Visitor Study 259 August 4–10, 2012 The National Park Service, Natural Resource Stewardship and Science office in Fort Collins, Colorado, publishes a range of reports that address natural resource topics. These reports are of interest and applicability to a broad audience in the National Park Service and others in natural resource management, including scientists, conservation and environmental constituencies, and the public. The Natural Resource Report Series is used to disseminate high-priority, current natural resource management information with managerial application. The series targets a general, diverse audience, and may contain NPS policy considerations or address sensitive issues of management applicability. All manuscripts in the series receive the appropriate level of peer review to ensure that the information is scientifically credible, technically accurate, appropriately written for the intended audience, and designed and published in a professional manner. Data in this report were collected and analyzed using methods based on established, peer- reviewed protocols and were analyzed and interpreted within the guidelines of the protocols. -
MOUNT RAINIER NATIONAL PARK Q
;;:4 L' L*I ! THE GEOLOGY 0F MOUNT RAINIER NATIONAL PARK q BY HOWARD A. COOMBS 4 II UNIVERSiTY OF WASHINGTON PUBLICATION S IN GEOLOGY Vol.3.No.2, pp. 131-212 July, 1936 THE GEOLOGY OF MOUNT RAINIER NATIONAL PARK BY HOWARD A. COOMBS PUBLISHED BY THE UNIVERSITY OF WASHINGTON SEATTLE, WASHINGTON 1936 CONTENTS PAGE Introduction 141 Location 141 Routes of Approach 141 Field Work 142 Acknowledgments 143 History 143 Review of Literature 144 Topography 145 Drainage 146 Climate 147 Fauna and Flora 148 Geology 149 Distribution and Relative Ages of the Rocks 149 The Puget Group 149 Keechelus Andesitic Series 150 Mineral Mountain Andesite Porphyry 152 Sheepskull Gap Tufts 154 Sourdough Mountain Breccias 155 Chinook Pass Diorite Porphyry 157 Longmire Acid Breccias 157 Starbo Altered Tufts 160 Cayuse Pass Acid Hornfels 161 Mowich Rypersthene Basalt 163 Summary 165 Relations and Age 165 Snoqualmie Granodiorite 167 Areal Extent 167 Petrography 168 Relations and Age 170 The Mount Rainier Volcanics 172 Composition 174 Microscopical Petrography 175 Plagioclase 175 Hypersthene 180 Monoclinic Hypersthene 184 Augite 184 Olivine 185 Hornblende 185 Holohyaline Groundmass 187 Hypo- and Holocrystalline Groundmass 187 Miscellaneous Features of the Groundmass 188 (135) CONTENTSContinued PAGE Physiography and Geomorphology 191 Introduction 191 The Cascades 191 Previous Literature 191 Pre-Rainier Topography 195 Pre-Rainier River Pattern 196 Pre-Rainier Structure 198 Conclusions 200 Summary 201 The Cone of Mount Rainier 202 The Summit Area 202 Glacial Erosion 204 Cleavers 204 Wedges 204 Intergiaciers 206 Asymmetrical Topography as a Result of Selective Glaciation. 207 Bibliography 211 Appendix A. Geologic Map of Mount Rainier National Park 212 ILLUSTRATIONS FIG. -
John Muirtrail
WWW.MOUNTAINEERS.ORG NOVEMBER/DECEMBER 2013 • VOLUME 107 • NO. 6 MountaineerE X P L O R E • L E A R N • C O N S E R V E John Epic Run Muir Trail +Tips For Lightweight Backcountry Travel ‘Our Secret Rainier’ Yellowstone Cliffs Part IV and Natural Bridge Turns All Year A personal look at backcountry skiing Avalanche 7Myths how to find a Marbled Murrelet and bake one too! inside Nov/Dec 2013 » Volume 107 » Number 6 Enriching the community by helping people explore, conserve, learn about, and enjoy the lands and waters of the Pacific Northwest and beyond. 12 Marbled Murrelet A Bird on the Brink 17 Sense of Courage Gavin Woody’s Epic Run on the John Muir Trail 20 ‘Our Secret Rainier’ Part IV Yellowstone Cliffs and Natural Bridge 23 Turns All Year 20 A personal look at backcountry skiing 28 A Family on Ice Trekking the Malaspina Glacier with two small children 6 CONSERVATION CURRENTS Sustainable Roads Analysis and National Heritage 10 IMPACT GIVING Volunteers join Peak Society through Matching Gifts 16 MEMBER PROFILE 23 An interview with Yinan Zhao 30 BOOKMARKS 28 With a Special Recipe by Author Maria Mudd Ruth 37 GLOBAL ADVENTURES Trekking through History: the Peruvian Andes 38 OUTDOOR CENTERS The Patrol Race Revisited 46 OFF BELAY Tragedy on Forbidden Peak 47 LAST WORD New Courage by Tad Wilkins Mountaineer magazine would like to thank DISCOVER THE MOUNTAINEERS The Mountaineers Foundation for its financial assistance. The Foundation operates as a separate If you are thinking of joining—or have joined and aren’t sure where to organization from The Mountaineers, which has received about one-third of the Foundation’s gifts to start—why not set a date to Meet The Mountainers? Check the various nonprofit organizations. -
MOUNT RAINIER NATIONAL PARK L/Lsajjiswujjarns
MOUNT RAINIER NATIONAL PARK l/lsajJiswujJArns UNITED STATES DEPARTMENT OF THE INTERIOR NATIONAL PARK SERVICE Mount Rainier [WASHINGTON] National Park United States Department of the Interior Harold L. Ickes, Secretary NATIONAL PARK SERVICE Arno B. Cammerer, Director UNITED STATES GOVERNMENT PRINTING OFFICE WASHINGTON : 1937 RULES AND REGULATIONS • Briefed • Events OF HISTORICAL IMPORTANCE REGULATIONS are designed not only to protect the natural beauties of the park but to aid visitors in the full enjoyment of this scenic area. You are requested to assist the park administration by respecting both the simple rules and the rights of others. The following synopsis is for your guidance; 1792 May 8. Capt. George Vancouver of the Royal British Navy, first white man to record sight of "The Mountain", complete rules and regulations may be seen at the superintendent's office named it Mount Rainier in honor of his friend Admiral at Longmire or at all ranger stations. Park rangers are here to help and Peter Rainier. advise you as well as to enforce the regulations. Consult them freely. 1833 September 2. Dr. William Fraser Tolmie of Nisqually House, a Hudson's Bay post, entered the northwest corner Fires.—Build fires only in designated places; always extinguish COMPLETELY before leav of what is now the park. He was the first white man to penetrate this region. ing camp. Do not guess your fire is out—KNOW IT. DO not throw burning tobacco or matches along the sides of roads or trails. 1857 July 16. Lt. A. V. Kautz of the United States Army gar rison at Fort Stcilacoom, and four companions, made the Keep park clean.—Keep your camp clean. -

Exclusive Content
EXCLUSIVE CONTENT EDITORS’ PICKS GET INSPIRED, GET INFORMED, AND GET GOING WITH OUR FAVORITE LONG READS FROM 2014-2019. schoolteacher. Her shoulder-length brown hair bordered full, rose-colored cheeks and wild, hungry-looking eyes. She car- ried a small backpack, loaded with a beat-up sleeping bag, a one-person tent, a Therm-a-Rest, a wispy rain jacket and wool baselayers, a compact headlamp, 6 liters of water, and snack food pre-portioned into small meals. The next morning, June 8, 2013, Barney, Sandy, and Anish piled into the Manns’ Prius at 5 a.m., and drove the 75 miles to the trailhead in Campo, California, near the Mexican border. Nobody spoke as they pulled up to the monu- ment, four weathered pillars of wood at the start of the PCT. More than 2,500 trail miles—crossing desert, forest, canyons, and mountain after moun- tain—lie between this spot and Canada. As Anish had told the Manns, she planned to hike that dis- tance faster than anybody ever had. She gathered her belongings while Sandy took a few photos and said goodbye. “She seemed very confident, but there was no braggadocio,” Sandy recalls. At 6:27 a.m., Anish signed the trail register: Well, here goes. To Canada. –Anish. In the previous two months, hundreds of hik- ers had signed the register. But Anish wasn’t like them, and none of them knew she was coming. In time, everyone on the trail would know her name. She wasn’t like the rest of them. ¶ They knew that.