Cytochrome C Oxidase Deficiency
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prioritization of Variants Detected by Next Generation Sequencing According to the Mutation Tolerance and Mutational Architecture of the Corresponding Genes
International Journal of Molecular Sciences Review Prioritization of Variants Detected by Next Generation Sequencing According to the Mutation Tolerance and Mutational Architecture of the Corresponding Genes Iria Roca, Ana Fernández-Marmiesse, Sofía Gouveia, Marta Segovia and María L. Couce * Unit of Diagnosis and Treatment of Congenital Metabolic Diseases, Department of Pediatrics, Hospital Clínico Universitario de Santiago de Compostela, 15706 Santiago de Compostela, Spain; [email protected] (I.R.); [email protected] (A.F.-M.); sofi[email protected] (S.G.); [email protected] (M.S.) * Correspondence: [email protected]; Tel.: +34-981-950-102 Received: 3 April 2018; Accepted: 23 May 2018; Published: 27 May 2018 Abstract: The biggest challenge geneticists face when applying next-generation sequencing technology to the diagnosis of rare diseases is determining which rare variants, from the dozens or hundreds detected, are potentially implicated in the patient’s phenotype. Thus, variant prioritization is an essential step in the process of rare disease diagnosis. In addition to conducting the usual in-silico analyses to predict variant pathogenicity (based on nucleotide/amino-acid conservation and the differences between the physicochemical features of the amino-acid change), three important concepts should be borne in mind. The first is the “mutation tolerance” of the genes in which variants are located. This describes the susceptibility of a given gene to any functional mutation and depends on the strength of purifying selection acting against it. The second is the “mutational architecture” of each gene. This describes the type and location of mutations previously identified in the gene, and their association with different phenotypes or degrees of severity. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

A Genetic Dissection of Mitochondrial Respiratory Chain Biogenesis
A GENETIC DISSECTION OF MITOCHONDRIAL RESPIRATORY CHAIN BIOGENESIS An Undergraduate Research Scholars Thesis by AARON GRIFFIN, SARAH THERIAULT, SHRISHIV TIMBALIA Submitted to Honors and Undergraduate Research Texas A&M University in partial fulfillment of the requirements for the designation as an UNDERGRADUATE RESEARCH SCHOLAR Approved by Research Advisor: Dr. Vishal Gohil May 2014 Major: Biochemistry, Genetics Biochemistry Biochemistry TABLE OF CONTENTS Page ABSTRACT .....................................................................................................................................1 CHAPTER I INTRODUCTION ...............................................................................................................3 II MATERIALS AND METHODS .........................................................................................7 Yeast strains, plasmids, and culture conditions .......................................................7 Yeast growth measurements ..................................................................................10 Yeast oxygen consumption and mitochondrial isolation .......................................11 SDS-PAGE and Western blotting ..........................................................................11 Sporulation, tetrad dissection, and genotyping ......................................................12 High-throughput phenotypic analysis of yeast strains ...........................................15 III RESULTS ..........................................................................................................................16 -

An Automated Pipeline for Inferring Variant-Driven Gene
www.nature.com/scientificreports OPEN MAGPEL: an autoMated pipeline for inferring vAriant‑driven Gene PanEls from the full‑length biomedical literature Nafseh Saberian1, Adib Shaf 1, Azam Peyvandipour1 & Sorin Draghici 1,2* In spite of the eforts in developing and maintaining accurate variant databases, a large number of disease‑associated variants are still hidden in the biomedical literature. Curation of the biomedical literature in an efort to extract this information is a challenging task due to: (i) the complexity of natural language processing, (ii) inconsistent use of standard recommendations for variant description, and (iii) the lack of clarity and consistency in describing the variant-genotype-phenotype associations in the biomedical literature. In this article, we employ text mining and word cloud analysis techniques to address these challenges. The proposed framework extracts the variant- gene‑disease associations from the full‑length biomedical literature and designs an evidence‑based variant-driven gene panel for a given condition. We validate the identifed genes by showing their diagnostic abilities to predict the patients’ clinical outcome on several independent validation cohorts. As representative examples, we present our results for acute myeloid leukemia (AML), breast cancer and prostate cancer. We compare these panels with other variant‑driven gene panels obtained from Clinvar, Mastermind and others from literature, as well as with a panel identifed with a classical diferentially expressed genes (DEGs) approach. The results show that the panels obtained by the proposed framework yield better results than the other gene panels currently available in the literature. One crucial step in understanding the biological mechanism underlying a disease condition is to capture the relationship between the variants and the disease risk1. -
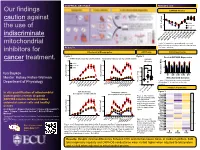
Boykov Our Findings Caution Against the Use of Indiscriminate
GRAPHICAL ABSTRACT RESULTS cont Our findings OXPHOS Kinetics 150 caution against 100 Colon 50 CT26.WT the use of of max JO2 % Heart 0 indiscriminate OligomycinFCCP FCCP[1µM] FCCP[2µM] FCCP[3µM] [4µM] GATPGATP (-54.16)GATP (-58.93)GATP (-60.64) (-61.49)FCCP [0.5µM] Δ Δ Δ Δ mitochondrial Figure 3 Respiration in permeabilized colon and heart strips and in permeabilized cells, depicted as a RESULTS % of max respiration. inhibitors for Mitochondrial Bioenergetics ATP/O ratio OXPHOS proteome Figure 1 Figure 2 Pooled OXPHOS Expression cancer treatment. OXPHOS Kinetics (per mg cellular protein) Respiratory Capacity (per mg cellular protein) OXPHOS 8000 8000 * Efficiency 100 * Colon * * * ns * * * 6000 CT26.WT 6000 * * ns 50 Heart * * 2.0 * * * ns 4000 * * 4000 * * * 1.5 (pmol/s/mg) 0 * Max of Percent (pmol/s/mg) 2 Ilya Boykov 2 2000 * * 2000 CI CII CIII CIV CV JO * JO * * * * * 1.0 * * Mentor: Kelsey Fisher-Wellman * (pmol/s/mg) Mitochondrial Complex * 2 0 0 0.5 Figure 4: Mitochondrial complex enrichment Department of Physiology JO depicted as % of max content for each P/M P/M CytC CytC PCRPCRPCR Basal BasalClamp Oligo complex Oct/Suc Rot/Anti Oct/Suc Rot/Anti 0.0 1uM FCCP2uM FCCP3uM FCCP4uM FCCP 1uM 2uMFCCP 3uMFCCP 4uMFCCP FCCP 0.5uM FCCP 0.5uM FCCP Complex IV proteome P/O Colon P/O Heart Figure 5 In situ quantification of mitochondrial OXPHOS Kinetics Respiratory Capacity P/O CT26.WT (per mg mitochondrial protein) (per mg mitochondrial protein) Cox7c 20000 Figure 2: Mitochondrial bioenergetics reveals disparate 20000 COX2 * * * * * P/O ratio in mitochondria Cox6b1 * * with 100uM ADP Cox6c OXPHOS kinetics between mouse 15000 * * 15000 * energized with Succinate Cox7a1 * * COX1 1 colorectal cancer cells and healthy * and Octanoyl-L-carnitine. -

Insights Towards FZ-CRD Folding and Therapeutic Landscape
Milhem and Ali Molecular Medicine (2020) 26:4 Molecular Medicine https://doi.org/10.1186/s10020-019-0129-7 REVIEW Open Access Disorders of FZ-CRD; insights towards FZ- CRD folding and therapeutic landscape Reham M. Milhem1* and Bassam R. Ali2,3 Abstract The ER is hub for protein folding. Proteins that harbor a Frizzled cysteine-rich domain (FZ-CRD) possess 10 conserved cysteine motifs held by a unique disulfide bridge pattern which attains a correct fold in the ER. Little is known about implications of disease-causing missense mutations within FZ-CRD families. Mutations in FZ-CRD of Frizzled class receptor 4 (FZD4) and Muscle, skeletal, receptor tyrosine kinase (MuSK) and Receptor tyrosine kinase- like orphan receptor 2 (ROR2) cause Familial Exudative Vitreoretinopathy (FEVR), Congenital Myasthenic Syndrome (CMS), and Robinow Syndrome (RS) respectively. We highlight reported pathogenic inherited missense mutations in FZ-CRD of FZD4, MuSK and ROR2 which misfold, and traffic abnormally in the ER, with ER-associated degradation (ERAD) as a common pathogenic mechanism for disease. Our review shows that all studied FZ-CRD mutants of RS, FEVR and CMS result in misfolded proteins and/or partially misfolded proteins with an ERAD fate, thus we coin them as “disorders of FZ-CRD”. Abnormal trafficking was demonstrated in 17 of 29 mutants studied; 16 mutants were within and/or surrounding the FZ-CRD with two mutants distant from FZ-CRD. These ER-retained mutants were improperly N-glycosylated confirming ER-localization. FZD4 and MuSK mutants were tagged with polyubiquitin chains confirming targeting for proteasomal degradation. Investigating the cellular and molecular mechanisms of these mutations is important since misfolded protein and ER-targeted therapies are in development. -

COA7 (C1orf163/RESA1) Mutations Associated With
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Apollo Mitochondrial genetics SHORT REPORT COA7 (C1orf163/RESA1) mutations associated with mitochondrial leukoencephalopathy and cytochrome c oxidase deficiency Anabel Martinez Lyons,1 Anna Ardissone,2 Aurelio Reyes,1 Alan J Robinson,1 Isabella Moroni,2 Daniele Ghezzi,3 Erika Fernandez-Vizarra,1 Massimo Zeviani1 1MRC-Mitochondrial Biology ABSTRACT mutations in mitochondrial DNA (mtDNA) or Unit, Cambridge, Background Assembly of cytochrome c oxidase (COX, nuclear DNA genes encoding structural COX subu- Cambridgeshire, UK 2Department of Child complex IV, cIV), the terminal component of the nits, but in most cases is due to recessive mutations Neurology, Milan, Italy mitochondrial respiratory chain, is assisted by several in nuclear genes encoding factors involved in COX 3Unit of Molecular factors, most of which are conserved from yeast to biogenesis.5 COA7 is a putative COX assembly Neurogenetics of the humans. However, some of them, including COA7, are factor containing five Sel1-like repeat domains Fondazione Istituto found in humans but not in yeast. COA7 is a 231aa- (Interpro IPR006597), is conserved in animals, but Neurologico “Carlo Besta”, Milan, Italy long mitochondrial protein present in animals, containing neither in plants nor in fungi, and has been five Sel1-like tetratricopeptide repeat sequences, which reported to localise in the mitochondrial IMS.6 Correspondence to are likely to interact with partner proteins. Here, we describe the first -

WO 2019/079361 Al 25 April 2019 (25.04.2019) W 1P O PCT
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization I International Bureau (10) International Publication Number (43) International Publication Date WO 2019/079361 Al 25 April 2019 (25.04.2019) W 1P O PCT (51) International Patent Classification: CA, CH, CL, CN, CO, CR, CU, CZ, DE, DJ, DK, DM, DO, C12Q 1/68 (2018.01) A61P 31/18 (2006.01) DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, C12Q 1/70 (2006.01) HR, HU, ID, IL, IN, IR, IS, JO, JP, KE, KG, KH, KN, KP, KR, KW, KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, (21) International Application Number: MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, PCT/US2018/056167 OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (22) International Filing Date: SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, 16 October 2018 (16. 10.2018) TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (25) Filing Language: English (84) Designated States (unless otherwise indicated, for every kind of regional protection available): ARIPO (BW, GH, (26) Publication Language: English GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, TZ, (30) Priority Data: UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, 62/573,025 16 October 2017 (16. 10.2017) US TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, ΓΕ , IS, IT, LT, LU, LV, (71) Applicant: MASSACHUSETTS INSTITUTE OF MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, SM, TECHNOLOGY [US/US]; 77 Massachusetts Avenue, TR), OAPI (BF, BJ, CF, CG, CI, CM, GA, GN, GQ, GW, Cambridge, Massachusetts 02139 (US). -

Supplementary Table S4. FGA Co-Expressed Gene List in LUAD
Supplementary Table S4. FGA co-expressed gene list in LUAD tumors Symbol R Locus Description FGG 0.919 4q28 fibrinogen gamma chain FGL1 0.635 8p22 fibrinogen-like 1 SLC7A2 0.536 8p22 solute carrier family 7 (cationic amino acid transporter, y+ system), member 2 DUSP4 0.521 8p12-p11 dual specificity phosphatase 4 HAL 0.51 12q22-q24.1histidine ammonia-lyase PDE4D 0.499 5q12 phosphodiesterase 4D, cAMP-specific FURIN 0.497 15q26.1 furin (paired basic amino acid cleaving enzyme) CPS1 0.49 2q35 carbamoyl-phosphate synthase 1, mitochondrial TESC 0.478 12q24.22 tescalcin INHA 0.465 2q35 inhibin, alpha S100P 0.461 4p16 S100 calcium binding protein P VPS37A 0.447 8p22 vacuolar protein sorting 37 homolog A (S. cerevisiae) SLC16A14 0.447 2q36.3 solute carrier family 16, member 14 PPARGC1A 0.443 4p15.1 peroxisome proliferator-activated receptor gamma, coactivator 1 alpha SIK1 0.435 21q22.3 salt-inducible kinase 1 IRS2 0.434 13q34 insulin receptor substrate 2 RND1 0.433 12q12 Rho family GTPase 1 HGD 0.433 3q13.33 homogentisate 1,2-dioxygenase PTP4A1 0.432 6q12 protein tyrosine phosphatase type IVA, member 1 C8orf4 0.428 8p11.2 chromosome 8 open reading frame 4 DDC 0.427 7p12.2 dopa decarboxylase (aromatic L-amino acid decarboxylase) TACC2 0.427 10q26 transforming, acidic coiled-coil containing protein 2 MUC13 0.422 3q21.2 mucin 13, cell surface associated C5 0.412 9q33-q34 complement component 5 NR4A2 0.412 2q22-q23 nuclear receptor subfamily 4, group A, member 2 EYS 0.411 6q12 eyes shut homolog (Drosophila) GPX2 0.406 14q24.1 glutathione peroxidase -
New Perspective in Diagnostics of Mitochondrial Disorders
Pronicka et al. J Transl Med (2016) 14:174 DOI 10.1186/s12967-016-0930-9 Journal of Translational Medicine RESEARCH Open Access New perspective in diagnostics of mitochondrial disorders: two years’ experience with whole‑exome sequencing at a national paediatric centre Ewa Pronicka1,2*, Dorota Piekutowska‑Abramczuk1†, Elżbieta Ciara1†, Joanna Trubicka1†, Dariusz Rokicki2, Agnieszka Karkucińska‑Więckowska3, Magdalena Pajdowska4, Elżbieta Jurkiewicz5, Paulina Halat1, Joanna Kosińska6, Agnieszka Pollak7, Małgorzata Rydzanicz6, Piotr Stawinski7, Maciej Pronicki3, Małgorzata Krajewska‑Walasek1 and Rafał Płoski6* Abstract Background: Whole-exome sequencing (WES) has led to an exponential increase in identification of causative vari‑ ants in mitochondrial disorders (MD). Methods: We performed WES in 113 MD suspected patients from Polish paediatric reference centre, in whom routine testing failed to identify a molecular defect. WES was performed using TruSeqExome enrichment, followed by variant prioritization, validation by Sanger sequencing, and segregation with the disease phenotype in the family. Results: Likely causative mutations were identified in 67 (59.3 %) patients; these included variants in mtDNA (6 patients) and nDNA: X-linked (9 patients), autosomal dominant (5 patients), and autosomal recessive (47 patients, 11 homozygotes). Novel variants accounted for 50.5 % (50/99) of all detected changes. In 47 patients, changes in 31 MD-related genes (ACAD9, ADCK3, AIFM1, CLPB, COX10, DLD, EARS2, FBXL4, MTATP6, MTFMT, MTND1, MTND3, MTND5, NAXE, NDUFS6, NDUFS7, NDUFV1, OPA1, PARS2, PC, PDHA1, POLG, RARS2, RRM2B, SCO2, SERAC1, SLC19A3, SLC25A12, TAZ, TMEM126B, VARS2) were identified. The ACAD9, CLPB, FBXL4, PDHA1 genes recurred more than twice suggesting higher general/ethnic prevalence. In 19 cases, variants in 18 non-MD related genes (ADAR, CACNA1A, CDKL5, CLN3, CPS1, DMD, DYSF, GBE1, GFAP, HSD17B4, MECP2, MYBPC3, PEX5, PGAP2, PIGN, PRF1, SBDS, SCN2A) were found. -

Mackenzie's Mission Gene & Condition List
Mackenzie’s Mission Gene & Condition List What conditions are being screened for in Mackenzie’s Mission? Genetic carrier screening offered through this research study has been carefully developed. It is focused on providing people with information about their chance of having children with a severe genetic condition occurring in childhood. The screening is designed to provide genetic information that is relevant and useful, and to minimise uncertain and unclear information. How the conditions and genes are selected The Mackenzie’s Mission reproductive genetic carrier screen currently includes approximately 1300 genes which are associated with about 750 conditions. The reason there are fewer conditions than genes is that some genetic conditions can be caused by changes in more than one gene. The gene list is reviewed regularly. To select the conditions and genes to be screened, a committee comprised of experts in genetics and screening was established including: clinical geneticists, genetic scientists, a genetic pathologist, genetic counsellors, an ethicist and a parent of a child with a genetic condition. The following criteria were developed and are used to select the genes to be included: • Screening the gene is technically possible using currently available technology • The gene is known to cause a genetic condition • The condition affects people in childhood • The condition has a serious impact on a person’s quality of life and/or is life-limiting o For many of the conditions there is no treatment or the treatment is very burdensome for the child and their family. For some conditions very early diagnosis and treatment can make a difference for the child. -

Loss of COX4I1 Leads to Combined Respiratory Chain Deficiency And
cells Article Loss of COX4I1 Leads to Combined Respiratory Chain Deficiency and Impaired Mitochondrial Protein Synthesis Kristýna Cunˇ átová 1,2, David Pajuelo Reguera 1 , Marek Vrbacký 1, Erika Fernández-Vizarra 3 , Shujing Ding 3, Ian M. Fearnley 3, Massimo Zeviani 3 , Josef Houštˇek 1 , Tomáš Mráˇcek 1,* and Petr Pecina 1,* 1 Laboratory of Bioenergetics, Institute of Physiology, Czech Academy of Sciences, 142 00 Prague, Czech Republic; [email protected] (K.C.);ˇ [email protected] (D.P.R.); [email protected] (M.V.); [email protected] (J.H.) 2 Department of Cell Biology, Faculty of Science, Charles University, 128 00 Prague, Czech Republic 3 MRC Mitochondrial Biology Unit, University of Cambridge, Cambridge CB2 0XY, UK; [email protected] (E.F.-V.); [email protected] (S.D.); [email protected] (I.M.F.); [email protected] (M.Z.) * Correspondence: [email protected] (T.M.); [email protected] (P.P.) Abstract: The oxidative phosphorylation (OXPHOS) system localized in the inner mitochondrial membrane secures production of the majority of ATP in mammalian organisms. Individual OXPHOS complexes form supramolecular assemblies termed supercomplexes. The complexes are linked not only by their function but also by interdependency of individual complex biogenesis or maintenance. For instance, cytochrome c oxidase (cIV) or cytochrome bc1 complex (cIII) deficiencies affect the level of fully assembled NADH dehydrogenase (cI) in monomeric as well as supercomplex forms. It was hypothesized that cI is affected at the level of enzyme assembly as well as at the level of cI stability and maintenance.