Prioritization of Variants Detected by Next Generation Sequencing According to the Mutation Tolerance and Mutational Architecture of the Corresponding Genes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -
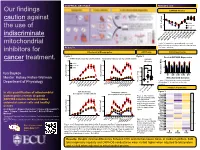
Boykov Our Findings Caution Against the Use of Indiscriminate
GRAPHICAL ABSTRACT RESULTS cont Our findings OXPHOS Kinetics 150 caution against 100 Colon 50 CT26.WT the use of of max JO2 % Heart 0 indiscriminate OligomycinFCCP FCCP[1µM] FCCP[2µM] FCCP[3µM] [4µM] GATPGATP (-54.16)GATP (-58.93)GATP (-60.64) (-61.49)FCCP [0.5µM] Δ Δ Δ Δ mitochondrial Figure 3 Respiration in permeabilized colon and heart strips and in permeabilized cells, depicted as a RESULTS % of max respiration. inhibitors for Mitochondrial Bioenergetics ATP/O ratio OXPHOS proteome Figure 1 Figure 2 Pooled OXPHOS Expression cancer treatment. OXPHOS Kinetics (per mg cellular protein) Respiratory Capacity (per mg cellular protein) OXPHOS 8000 8000 * Efficiency 100 * Colon * * * ns * * * 6000 CT26.WT 6000 * * ns 50 Heart * * 2.0 * * * ns 4000 * * 4000 * * * 1.5 (pmol/s/mg) 0 * Max of Percent (pmol/s/mg) 2 Ilya Boykov 2 2000 * * 2000 CI CII CIII CIV CV JO * JO * * * * * 1.0 * * Mentor: Kelsey Fisher-Wellman * (pmol/s/mg) Mitochondrial Complex * 2 0 0 0.5 Figure 4: Mitochondrial complex enrichment Department of Physiology JO depicted as % of max content for each P/M P/M CytC CytC PCRPCRPCR Basal BasalClamp Oligo complex Oct/Suc Rot/Anti Oct/Suc Rot/Anti 0.0 1uM FCCP2uM FCCP3uM FCCP4uM FCCP 1uM 2uMFCCP 3uMFCCP 4uMFCCP FCCP 0.5uM FCCP 0.5uM FCCP Complex IV proteome P/O Colon P/O Heart Figure 5 In situ quantification of mitochondrial OXPHOS Kinetics Respiratory Capacity P/O CT26.WT (per mg mitochondrial protein) (per mg mitochondrial protein) Cox7c 20000 Figure 2: Mitochondrial bioenergetics reveals disparate 20000 COX2 * * * * * P/O ratio in mitochondria Cox6b1 * * with 100uM ADP Cox6c OXPHOS kinetics between mouse 15000 * * 15000 * energized with Succinate Cox7a1 * * COX1 1 colorectal cancer cells and healthy * and Octanoyl-L-carnitine. -

Biogenesis of Cytochrome C Oxidase — in Vitro Approaches to Study Cofactor Insertion Into a Bacterial Subunit I
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Biochimica et Biophysica Acta 1777 (2008) 904–911 Contents lists available at ScienceDirect Biochimica et Biophysica Acta journal homepage: www.elsevier.com/locate/bbabio Review Biogenesis of cytochrome c oxidase — in vitro approaches to study cofactor insertion into a bacterial subunit I Peter Greiner ⁎, Achim Hannappel, Carolin Werner, Bernd Ludwig Institute for Biochemistry, Molecular Genetics, Johann-Wolfgang-Goethe University, Max-von-Laue Straβe 9, 60438 Frankfurt am Main, Germany ARTICLE INFO ABSTRACT Article history: Biogenesis of cytochrome c oxidase is a complex process involving more than 30 known accessory proteins in Received 30 November 2007 yeast for the regulation of transcription and translation, membrane insertion and protein processing, cofactor Received in revised form 25 March 2008 insertion, and subunit assembly. Here, we focus on the process of cofactor insertion into subunit I of Accepted 2 April 2008 cytochrome c oxidase using the soil bacterium Paracoccus denitrificans as a model organism. The use of Available online 10 April 2008 bacterial systems facilitates biogenesis studies, as the number of required assembly factors is reduced to a Keywords: minimum. Both, co- and posttranslational cofactor insertion scenarios are discussed, and several approaches Assembly to shed light on this aspect of biogenesis are presented. CtaG, the Paracoccus homolog of yeast Cox11 which is fi Cox11 involved in copper delivery to the CuB center, has been puri ed and characterized spectroscopically. A Copper chaperone previously unreported signal at 358 nm allows monitoring copper transfer from copper-loaded CtaG to an Heme a acceptor. -

Lamin A/C Cardiomyopathy: Implications for Treatment
Current Cardiology Reports (2019) 21:160 https://doi.org/10.1007/s11886-019-1224-7 MYOCARDIAL DISEASE (A ABBATE AND G SINAGRA, SECTION EDITORS) Lamin A/C Cardiomyopathy: Implications for Treatment Suet Nee Chen1 & Orfeo Sbaizero1,2 & Matthew R. G. Taylor1 & Luisa Mestroni1 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of Review The purpose of this review is to provide an update on lamin A/C (LMNA)-related cardiomyopathy and discuss the current recommendations and progress in the management of this disease. LMNA-related cardiomyopathy, an inherited autosomal dominant disease, is one of the most common causes of dilated cardiomyopathy and is characterized by steady progression toward heart failure and high risks of arrhythmias and sudden cardiac death. Recent Findings We discuss recent advances in the understanding of the molecular mechanisms of the disease including altered cell biomechanics, which may represent novel therapeutic targets to advance the current management approach, which relies on standard heart failure recommendations. Future therapeutic approaches include repurposed molecularly directed drugs, siRNA- based gene silencing, and genome editing. Summary LMNA-related cardiomyopathy is the focus of active in vitro and in vivo research, which is expected to generate novel biomarkers and identify new therapeutic targets. LMNA-related cardiomyopathy trials are currently underway. Keywords Lamin A/C gene . Laminopathy . Heart failure . Arrhythmias . Mechanotransduction . P53 . CRISPR–Cas9 therapy Introduction functions, including maintaining nuclear structural integrity, regulating gene expression, mechanosensing, and Mutations in the lamin A/C gene (LMNA)causelaminopathies, mechanotransduction through the lamina-associated proteins a heterogeneous group of inherited disorders including muscu- [6–11]. -

WES Gene Package Multiple Congenital Anomalie.Xlsx
Whole Exome Sequencing Gene package Multiple congenital anomalie, version 5, 1‐2‐2018 Technical information DNA was enriched using Agilent SureSelect Clinical Research Exome V2 capture and paired‐end sequenced on the Illumina platform (outsourced). The aim is to obtain 8.1 Giga base pairs per exome with a mapped fraction of 0.99. The average coverage of the exome is ~50x. Duplicate reads are excluded. Data are demultiplexed with bcl2fastq Conversion Software from Illumina. Reads are mapped to the genome using the BWA‐MEM algorithm (reference: http://bio‐bwa.sourceforge.net/). Variant detection is performed by the Genome Analysis Toolkit HaplotypeCaller (reference: http://www.broadinstitute.org/gatk/). The detected variants are filtered and annotated with Cartagenia software and classified with Alamut Visual. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM median depth % covered % covered % covered gene symbol gene ID >10x >20x >30x A4GALT [Blood group, P1Pk system, P(2) phenotype], 111400 607922 101 100 100 99 [Blood group, P1Pk system, p phenotype], 111400 NOR polyagglutination syndrome, 111400 AAAS Achalasia‐addisonianism‐alacrimia syndrome, 231550 605378 73 100 100 100 AAGAB Keratoderma, palmoplantar, -

Supplementary Table S4. FGA Co-Expressed Gene List in LUAD
Supplementary Table S4. FGA co-expressed gene list in LUAD tumors Symbol R Locus Description FGG 0.919 4q28 fibrinogen gamma chain FGL1 0.635 8p22 fibrinogen-like 1 SLC7A2 0.536 8p22 solute carrier family 7 (cationic amino acid transporter, y+ system), member 2 DUSP4 0.521 8p12-p11 dual specificity phosphatase 4 HAL 0.51 12q22-q24.1histidine ammonia-lyase PDE4D 0.499 5q12 phosphodiesterase 4D, cAMP-specific FURIN 0.497 15q26.1 furin (paired basic amino acid cleaving enzyme) CPS1 0.49 2q35 carbamoyl-phosphate synthase 1, mitochondrial TESC 0.478 12q24.22 tescalcin INHA 0.465 2q35 inhibin, alpha S100P 0.461 4p16 S100 calcium binding protein P VPS37A 0.447 8p22 vacuolar protein sorting 37 homolog A (S. cerevisiae) SLC16A14 0.447 2q36.3 solute carrier family 16, member 14 PPARGC1A 0.443 4p15.1 peroxisome proliferator-activated receptor gamma, coactivator 1 alpha SIK1 0.435 21q22.3 salt-inducible kinase 1 IRS2 0.434 13q34 insulin receptor substrate 2 RND1 0.433 12q12 Rho family GTPase 1 HGD 0.433 3q13.33 homogentisate 1,2-dioxygenase PTP4A1 0.432 6q12 protein tyrosine phosphatase type IVA, member 1 C8orf4 0.428 8p11.2 chromosome 8 open reading frame 4 DDC 0.427 7p12.2 dopa decarboxylase (aromatic L-amino acid decarboxylase) TACC2 0.427 10q26 transforming, acidic coiled-coil containing protein 2 MUC13 0.422 3q21.2 mucin 13, cell surface associated C5 0.412 9q33-q34 complement component 5 NR4A2 0.412 2q22-q23 nuclear receptor subfamily 4, group A, member 2 EYS 0.411 6q12 eyes shut homolog (Drosophila) GPX2 0.406 14q24.1 glutathione peroxidase -

The Genetic Mechanism That Links Hutchinson-Gilford Progeria Syndrome to Physiological Aging
Department of Biosciences and Nutrition The genetic mechanism that links Hutchinson-Gilford progeria syndrome to physiological aging AKADEMISK AVHANDLING som för avläggande av medicine doktorsexamen vid Karolinska Institutet offentligen försvaras i Hörsalen, plan 4, Novum, Huddinge. Fredagen den 14 februari, 2014, kl 09.15 av Sofía Rodríguez Vásquez B.Sc. Licentiate in Biological Sciences Huvudhandledare: Fakultetsopponent: Docent Maria Eriksson Professor Karima Djabali Karolinska Institutet Technical University Munich Institutionen för Biovetenskaper och Department of Dermatology and Näringslära Institute for Medical Engineering Bihandledare: Betygsnämnd: Professor Karin Dahlman-Wright Docent Rickard Sandberg Karolinska Institutet Karolinska Institutet Institutionen för Biovetenskaper och Institutionen för Cell- och Molekylär Näringslära Biologi Professor Caroline Graff Professor Brun Ulfhake Karolinska Institutet Karolinska Institutet Institutionen för Neurobiologi, Institutionen för Neurovetenskap Vårdvetenskap och Samhälle Professor Jan Dumanski Uppsala Universitet Institutionen för Immunologi, Genetik och Patologi. Enheten för Medicinsk Genetik Stockholm 2014 DEPARTMENT OF BIOSCIENCES AND NUTRITION Karolinska Institutet, Stockholm, Sweden THE GENETIC MECHANISM THAT LINKS HUTCHINSON-GILFORD PROGERIA SYNDROME TO PHYSIOLOGICAL AGING Sofía Rodríguez Vásquez Stockholm 2014 All previously published papers were reproduced with permission from the publisher. Published by Karolinska Institutet. © Sofia Rodríguez Vásquez, 2014 ISBN 978-91-7549-372-5 Printed by Printed by 2014 Gårdsvägen 4, 169 70 Solna Dedicated to my beloved parents and life heroes: Benito Rodríguez Rodríguez & Doris Vásquez Silva ABSTRACT Aging is a complex process that is not completely understood. The study of segmental progeroid syndromes such as Hutchinson-Gilford progeria syndrome (HGPS) has allowed us to connect the common genetic mechanisms that occur in normal physiological aging, with the cellular alterations presented by this severe premature aging syndrome. -

Coa3 and Cox14 Are Essential for Negative Feedback Regulation of COX1 Translation in Mitochondria
JCB: Article Coa3 and Cox14 are essential for negative feedback regulation of COX1 translation in mitochondria David U. Mick,1,2,3 Milena Vukotic,3 Heike Piechura,4 Helmut E. Meyer,4 Bettina Warscheid,4,5 Markus Deckers,3 and Peter Rehling3 1Institut für Biochemie und Molekularbiologie, Zentrum für Biochemie und Molekulare Zellforschung and 2Fakultät für Biologie, Universität Freiburg, D-79104 Freiburg, Germany 3Abteilung für Biochemie II, Universität Göttingen, D-37073 Göttingen, Germany 4Medizinisches Proteom-Center, Ruhr-Universität Bochum, D-44801 Bochum, Germany 5Clinical and Cellular Proteomics, Duisburg-Essen Universität, D-45117 Essen, Germany egulation of eukaryotic cytochrome oxidase assem- newly synthesized Cox1 and are required for Mss51 as- bly occurs at the level of Cox1 translation, its central sociation with these complexes. Mss51 exists in equilibrium Rmitochondria-encoded subunit. Translation of COX1 between a latent, translational resting, and a committed, messenger RNA is coupled to complex assembly in a neg- translation-effective, state that are represented as distinct ative feedback loop: the translational activator Mss51 is complexes. Coa3 and Cox14 promote formation of the thought to be sequestered to assembly intermediates, ren- latent state and thus down-regulate COX1 expression. dering it incompetent to promote translation. In this study, Consequently, lack of Coa3 or Cox14 function traps Mss51 we identify Coa3 (cytochrome oxidase assembly factor 3; in the committed state and promotes Cox1 synthesis. Our Yjl062w-A), a novel regulator of mitochondrial COX1 data indicate that Coa1 binding to sequestered Mss51 in translation and cytochrome oxidase assembly. We show complex with Cox14, Coa3, and Cox1 is essential for that Coa3 and Cox14 form assembly intermediates with full inactivation. -

Human Induced Pluripotent Stem Cell–Derived Podocytes Mature Into Vascularized Glomeruli Upon Experimental Transplantation
BASIC RESEARCH www.jasn.org Human Induced Pluripotent Stem Cell–Derived Podocytes Mature into Vascularized Glomeruli upon Experimental Transplantation † Sazia Sharmin,* Atsuhiro Taguchi,* Yusuke Kaku,* Yasuhiro Yoshimura,* Tomoko Ohmori,* ‡ † ‡ Tetsushi Sakuma, Masashi Mukoyama, Takashi Yamamoto, Hidetake Kurihara,§ and | Ryuichi Nishinakamura* *Department of Kidney Development, Institute of Molecular Embryology and Genetics, and †Department of Nephrology, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan; ‡Department of Mathematical and Life Sciences, Graduate School of Science, Hiroshima University, Hiroshima, Japan; §Division of Anatomy, Juntendo University School of Medicine, Tokyo, Japan; and |Japan Science and Technology Agency, CREST, Kumamoto, Japan ABSTRACT Glomerular podocytes express proteins, such as nephrin, that constitute the slit diaphragm, thereby contributing to the filtration process in the kidney. Glomerular development has been analyzed mainly in mice, whereas analysis of human kidney development has been minimal because of limited access to embryonic kidneys. We previously reported the induction of three-dimensional primordial glomeruli from human induced pluripotent stem (iPS) cells. Here, using transcription activator–like effector nuclease-mediated homologous recombination, we generated human iPS cell lines that express green fluorescent protein (GFP) in the NPHS1 locus, which encodes nephrin, and we show that GFP expression facilitated accurate visualization of nephrin-positive podocyte formation in -

Arthrogryposis and Congenital Myasthenic Syndrome Precision Panel
Arthrogryposis and Congenital Myasthenic Syndrome Precision Panel Overview Arthrogryposis or arthrogryposis multiplex congenita (AMC) is a group of nonprogressive conditions characterized by multiple joint contractures found throughout the body at birth. It usually appears as a feature of other neuromuscular conditions or part of systemic diseases. Primary cases may present prenatally with decreased fetal movements associated with joint contractures as well as brain abnormalities, decreased muscle bulk and polyhydramnios whereas secondary causes may present with isolated contractures. Congenital Myasthenic Syndromes (CMS) are a clinically and genetically heterogeneous group of disorders characterized by impaired neuromuscular transmission. Clinically they usually present with abnormal fatigability upon exertion, transient weakness of extra-ocular, facial, bulbar, truncal or limb muscles. Severity ranges from mild, phasic weakness, to disabling permanent weakness with respiratory difficulties and ultimately death. The mode of inheritance of these diseases typically follows and autosomal recessive pattern, although dominant forms can be seen. The Igenomix Arthrogryposis and Congenital Myasthenic Syndrome Precision Panel can be as a tool for an accurate diagnosis ultimately leading to a better management and prognosis of the disease. It provides a comprehensive analysis of the genes involved in this disease using next-generation sequencing (NGS) to fully understand the spectrum of relevant genes involved, and their high or intermediate penetrance. -
Long Non‑Coding RNA AK055347 Is Upregulated in Patients with Atrial Fibrillation and Regulates Mitochondrial Energy Production in Myocardiocytes
MOLECULAR MEDICINE REPORTS 14: 5311-5317, 2016 Long non‑coding RNA AK055347 is upregulated in patients with atrial fibrillation and regulates mitochondrial energy production in myocardiocytes GUIYING CHEN*, HONG GUO*, YING SONG, HUIYING CHANG, SHAOJUN WANG, MIAOMIAO ZHANG and CHANG LIU Department of Cardiology, The First Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang 150001, P.R. China Received September 10, 2015; Accepted September 22, 2016 DOI: 10.3892/mmr.2016.5893 Abstract. The role of long non-coding RNAs (lncRNAs) in and mortality. However, the etiology of AF is complex and atrial fibrillation remains to be fully elucidated. The current unclear, and inherited and environmental factors have been study performed microarray analysis to investigate differen- reported to be involved (5,6). tial lncRNA expression profiling in atrial samples from the The progression of AF is commonly accompanied with pulmonary vein and the surrounding left atrial area (LA‑PV) alterations in gene expression, thus resulting in abnormal protein and from the left atrial appendage (LAA) in 16 patients expression expression (7,8). A previous study identified that long with atrial fibrillation (AF). Microarray analysis identified non‑coding RNAs (lncRNAs), endogenous RNAs >200 nucleo- 94 lncRNAs that were differentially expressed between the tides in length that do not code for functional proteins, regulate LA‑PV and LAA in patients with AF. AK055347 was one the gene expression of numerous proteins (9). Several studies of lncRNAs with the most significant alterations observed. have demonstrated that lncRNAs are associated with diseases Knockdown of AK055347 inhibited cell viability of H9C2 including cancer (10), endocrine diseases (11), liver diseases (12) cardiomyocytes, accompanied by downregulation of Cyp450 and heart diseases (13,14). -

Case Report of Malouf Syndrome Not Associated with LMNA Gene Mutation
MOJ Clinical & Medical Case Reports Case Report Open Access Case report of malouf syndrome not associated with LMNA gene mutation Abstract Volume 4 Issue 6 - 2016 Malouf syndrome, currently known as dilated cardiomyopathy associated with Tatiyana G Vaikhanskaya,1 Larysa N hypergonadotropic hypogonadism (DCM-НН), is a rare congenital disorder with Sivitskaya,2 Nina G Danilenko,2 Tatsiyana V clinical signs including DCM phenotype, ovary dysgenesis in females or primary 1 2 testicular failure in males, mental retardation, facial dysmorphism, skin lesions, bone Kurushka, Oleg G Davydenko abnormalities and occasionally marfanoid habitus. The disorder can be caused by 1Health Information Technology Department, Republican mutation in the LMNA gene, encoding lamins A and C. In the present manuscript, Scientific and Practical Centre of Cardiology, Belarus we report the sporadic case of a young female with dilated cardiomyopathy, 2Cytoplasmic Inheritance Department, Institute of Genetics hypergonadotropic hypogonadism and primary amenorrhea, cognitive deficiency, and Cytology of the National Academy of Sciences of Belarus, body mass deficit, facial dysmorphism and subclinical hypothyroidism. Radiation Belarus exposure, mumps, diabetes mellitus, autoimmune diseases, and Turner’s syndrome have been ruled out. Specific features of mandibuloacral dysplasia, like bone dysplasia, Correspondence: Tatiyana G Vaikhanskaya, Health Information are absent. The first-degree relatives are healthy. The clinical data suggested a Technology Department, Republican Scientific and Practical laminopathy. Targeted next-generation sequencing was used to search for mutations in Centre of Cardiology, 220036, R Lyuksembourg str 110, Minsk, genes, associated with cardiomyopathy, including LMNA. However, genetic analysis Belarus, Tel +375291307140, Email [email protected] did not confirm the assumption: mutation was not found.