Public-Trust-Board-27-September
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Notice of Uncontested Elections
NOTICE OF UNCONTESTED ELECTION West Northamptonshire Council Election of Parish Councillors for Arthingworth on Thursday 6 May 2021 I, Anna Earnshaw, being the Returning Officer at the above election, report that the persons whose names appear below were duly elected Parish Councillors for Arthingworth. Name of Candidate Home Address Description (if any) HANDY 5 Sunnybank, Kelmarsh Road, Susan Jill Arthingworth, LE16 8JX HARRIS 8 Kelmarsh Road, Arthingworth, John Market Harborough, Leics, LE16 8JZ KENNEDY Middle Cottage, Oxendon Road, Bernadette Arthingworth, LE16 8LA KENNEDY (address in West Michael Peter Northamptonshire) MORSE Lodge Farm, Desborough Rd, Kate Louise Braybrooke, Market Harborough, Leicestershire, LE16 8LF SANDERSON 2 Hall Close, Arthingworth, Market Lesley Ann Harborough, Leics, LE16 8JS Dated Thursday 8 April 2021 Anna Earnshaw Returning Officer Printed and published by the Returning Officer, Civic Offices, Lodge Road, Daventry, Northants, NN11 4FP NOTICE OF UNCONTESTED ELECTION West Northamptonshire Council Election of Parish Councillors for Badby on Thursday 6 May 2021 I, Anna Earnshaw, being the Returning Officer at the above election, report that the persons whose names appear below were duly elected Parish Councillors for Badby. Name of Candidate Home Address Description (if any) BERRY (address in West Sue Northamptonshire) CHANDLER (address in West Steve Northamptonshire) COLLINS (address in West Peter Frederick Northamptonshire) GRIFFITHS (address in West Katie Jane Northamptonshire) HIND Rosewood Cottage, Church -

Market Harborough | Welford | Guilsborough | Northampton Mondays, Wednesdays & Thursdays Tuesdays & Fridays Except Public Holidays Except Public Holidays
59 60 Market Harborough | Welford | Guilsborough | Northampton Mondays, Wednesdays & Thursdays Tuesdays & Fridays except public holidays except public holidays 60 60 60 60 60 60 60 59 60 Welford bus shelter 0945 1155 1528 Market Harborough Market Hall 1250 Naseby post box 0955 1205 u Lubenham The Green 1300 Cold Ashby bus shelter 0959 1209 1538 Marston Trussell 1304 Thornby bus shelter 1004 1214 1543 Sibbertoft Berkeley Street 1310 Guilsborough Academy u u 1545 Clipston The Green 1317 Guilsborough bus shelter 0706 0820 1010 1220 1549 Naseby post box 1322 Hollowell bus stop 0709 0823 1013 1223 1552 Welford bus shelter arrive 1332 Creaton main road 0712 0826 1016 1226 1555 same bus, no need to change u Creaton The Jetty u u 1018 u u Welford bus shelter arrive 1332 1528 Spratton main road 0716 0830 u 1230 1559 Cold Ashby bus shelter 1342 1538 Spratton Brixworth Road u u 1022 u u Thornby bus shelter 1347 1543 Chapel Brampton Cedar Hythe 0720 0834 1028 1234 1603 Guilsborough Academy u 1545 Kingsthorpe opp Waitrose 0726 0840 1034 1240 1609 Guilsborough bus shelter 0706 0820 1353 1549 Northampton North Gate bus station 0735 0851 1042 1249 1617 Hollowell bus stop 0709 0823 1356 1552 Creaton main road 0712 0826 1359 1555 Spratton main road 0716 0830 1403 1559 Chapel Brampton Cedar Hythe 0720 0834 1407 1603 Kingsthorpe opp Waitrose 0726 0840 1413 1609 this bus goes to Guilsborough Northampton North Gate bus station 0735 0851 1422 1617 Academy on school days only this bus shows route 60 between Welford and Northampton this bus goes to Guilsborough -

Obedience Robins of Accomack: 17Th-Century
OBEDIENCE ROBINS OF ACCOMACK: 17TH-CENTURY STRATEGIES FOR SUCCESS A Thesis MARY CA~ WILHEIT Submitted to the Once of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF ARTS December 1997 Major Subject: History OBEDIENCE ROBINS OF ACCOMACK: 17TH-CENTURY STRATEGIES FOR SUCCESS A Thesis MARY CA~ WILHEIT Submitted to Texas AyrM University in partial tulfillment of thc requirements for the degree of MASTER OF ARTS Approved as to style and content by. John L. Canup Walter L. Buenger ( hair of Committee) (Member) Dennis A. Berthold Julia Kirk ckvvelder (Member) (Head ol Dcpa nt) December 1997 Major Subject: History ABSTRACT Obedience Robins of Accomack: 17th-Century Strategies for Success. (December 1997) Mary Catherine Wilheit, A. B., Wilson College Chair of Advisory Committee: Dr. John L. Canup Obedience Robins emigrated to Virginia in the 1620s in search of the land and status his elder brother gained by inheritance. This thesis establishes motivations for immigration and methods by which one English emigr6 achieved success in Virginia. The 1582 will of Richard Robins established a pattern of primogeniture for successive generations of his Northamptonshire family. Muster lists, wills, parish registers and a 1591 manor survey record increasing prosperity and associated expectations. Robinses were among those "better sorts" who paid taxes, provided armour, held local office, educated their children, and protcstcd against perceived government injustice. In Virginia. Richard Robins*s great grandson parlayed his assets into land, office and status. The extent of his education and financial resources was probably limited, but good health, timing. -

CREATON PARISH COUNCIL Chairman: Mr Stan Perrins Clerk: Mrs L Compton 12 Olde Forde Close Brixworth Northants NN6 9XF
CREATON PARISH COUNCIL Chairman: Mr Stan Perrins Clerk: Mrs L Compton 12 Olde Forde Close Brixworth Northants NN6 9XF Tel/Fax 01604-880727 Email: creatonpc@tiscali co.uk Minutes of the meeting of Creaton Parish Council held on Tuesday 7th September 2010 in the Village Hall, Teeton Lane at 8.00 pm Present: Councillors Stanley Perrins (Chair), Richard Hollingum, Reg Thomas, Maureen Titman and Sylvia Winter In attendance: District Cllr Barry Frenchman, Lynne Compton, Clerk and 2 members of the public Notes from Open Forum : Royal British Legion Poppy Appeal A resident requested that the amount donated from the Parish Council for the purchase of the poppy wreath should increase from £20 to £25 due to rising costs. The current cost of a poppy wreath being £17 Power(s) Action 56. RESOLUTION TO APPROVE APOLOGIES FOR ABSENCE Cllr Perrins proposed acceptance of apologies from Cllr Jack, Cllr Pugh, Cllr Watt and County Councillor Millar, these were seconded by Cllr Hollingum and resolved to be approved by Parish Council 57. RESOLUTION TO SIGN AND APPROVE MINUTES OF MEETING AND AGENDA dated 6th July 2010. These were proposed by Cllr Hollingum, seconded by Cllr Thomas and resolved to be approved by Parish Council 58. MATTERS ARISING FROM PREVIOUS MINUTES (for information only) a) Rural Affordable Housing – It was reported that Joanne Martin (formally Richardson) from Midlands Rural Housing, would provide an update at the October meeting. b) Creaton Appraisal Group – Linda Toombs reported that they were now in a position Clerk to close the account, and as previously agreed, the funds would be transferred to Creaton Parish Council and held in reserve for the future. -

From Long Buckby, Creaton, Crick and Kilsby
Dates for your Diary December 2019 From Long Buckby, Creaton, 7.12.19 Crick 10.30-12.00 noon Charity Coffee Morning Crick and Kilsby 7.12.19 Long Buckby 10.30-11.30 Charity Coffee Morning 5.12.19 Creaton 12.00 noon Nosh & Natter (men’s lunch) (North West Northants. Pastorate) 13.12.19 Long Buckby 12.30 pm for 1.00 pm Lunch Club 19.12.19 Crick 7.00 pm Carols By Candlelight 22.12.19 Long Buckby 6.00 pm Carols with Daventry Brass Band 29.12.19 Long Buckby 2.00 pm Joint Service with tea & cake Long Buckby Secretary January 2020 Lucy Faulkner 07738 156722 2.1.20 Creaton 12.00 noon Nosh & Natter (men’s lunch) Junior Church 10.1.20 Long Buckby 12.30 pm for 1.00 pm Lunch Club Norman Chandler 01327 843813 20.1.20 Crick 2.00 pm Joint Elders Meeting Peggy Bond 01327 842234 February 2020 Creaton 1.2.20 Long Buckby 10.30-11.30 am Charity Coffee Morning Secretary 1.2.20 Crick 10.30-12 noon Charity Coffee Morning Carolyn Wilson 01604 505650 5.2.20 Long Buckby 2.15 pm Ladies Circle 6.2.20 Creaton 12.00 noon Nosh & Natter (men’s lunch) 14.2.20 Long Buckby 12.30 pm for 1.00 pm Lunch Club Crick Kilsby 18.2.20 Long Buckby 7.00 pm Elders Meeting Secretary Secretary & Treasurer Brenda Morgan 01788 822564 Val Janes 01788 822751 Newsletter Editor See page 14 for details of New Editor Happy Christmas and best wishes for the New Year Deadline for March—May newsletter 16th February 2020 and thank you for all your kind words. -
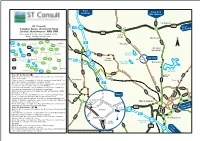
Southern Testing Location Map (Northampton)
From Leicester From A14 Mkt Harboro Harrington ST Consult A5199 A508 A14 M6 J19 J1 From Twigden Barns, Brixworth Road Kettering Creaton, Northampton NN6 8NN A5 A14 Tel: 01604 500020 - Fax: 01604 500021 Cold Email: [email protected] Ashby www.stconsult.co.uk A5199 Maidwell N A43 A508 A14 M6 Kettering Thrapston M1 J19 A14 Thornby A14 W e Rugby l A5199 fo Creaton rd Hanging J18 A43 A6 A45 R o a M45 A428 d Houghton J17 A508 Wellingborough J18 Hollowell A45 A428 Rushden M1 A428 Reservoir Daventry A45 See Inset Northampton A509 West A425 A6 M45 Haddon CreatonCreaton J16 Ravensthorpe A428 Brixworth J15a J17 Reservoir A5 J15 A43 A361 A428 Bedford A508 A361 Pitsford Towcester Ha M1 A509 rle Reservoir st on B5385 e R From M1 Northbound o Harborough a W d Road A43 Exit the M1 at junction 15a, Rothersthorpe Services and follow Long e l f signs to the A43. A5 Buckby o r Braunston d Once at the A43 roundabout, turn left and pass under the M1 to R Thorpeville o A508 arrive at a further roundabout, continue ahead. M1 a d Remain on the A43 over the next three roundabouts, at the next A45 roundabout take the third exit onto the A4500. Continue over the next two roundabouts and after a further 1/2 A5199 A5076 mile turn left onto the A428 Spencer Bridge Road. A428 Pass over the rail and river bridges and turn left onto the A5095 St Andrews Road. Inset At the junction with the A508 turn left onto Kingsthorpe Road. -

Creaton Village Design Statement
Creaton Design Statement Adopted by Daventry District Council as Supplementary Planning Guidance September 2004 CREATON DESIGN STATEMENT CONTENTS 1. Village Context 2. Landscape Character 3. Settlement 4. Important Public and Private Spaces 5. Buildings 6. Highway and Street Furniture 7. Conservation 8. Appendices A1 Important Spaces and Views - Map A2 Important Spaces and Views - Photographs a) Views in to Creaton b) Views out from Creaton c) Views within Creaton B Development Zones C Walls and Verges D Trees and Listed buildings E Buildings INTRODUCTION The Village Design Statement, prepared during 2003 and 2004, describes Creaton as it is today and highlights the qualities valued by its residents. The Design Statement was initiated, funded and supported by Creaton Parish Council but was prepared by an independent team of volunteers in consultation with all households in the village and the Local Planning Authority. A workshop and consultation/exhibition day were held to ensure that local knowledge, views and ideas were included in this document and represent those of the village. The Design Statement aims to make sure that the local distinctiveness and character of Creaton is taken into consideration when local planning decisions are being taken. Change is brought about not only by large developments, but also by the smaller day-to-day adjustments to homes and gardens, open spaces, paths and hedges, which alter the look and feel of the whole village. The Design Statement sets out the principles, design features and quality standards that should be taken into account by those wishing to build, modify or extend property in the parish of Creaton. -

Vol 3 Contents
NORTHAMPTONSHIRE PAST ·& PRESENT VOLUME Ill NORTHAMPTONSHIRE PAST & PRESENT THE JOURNAL OF THE NORTHAMPTONSHIRE RECORD SOCIETY VOLUME Ill IN SIX PARTS 1960-1965 Edited by GYLES ISHAM Published by THE NORTHAMPTONSHIRE RECORD SOCIETY DELAPRE ABBEY NORTHAMPTON 1967 PRINTED IN GREAT BRITAIN V CONTENTS. List of Contents will be found at the beginning of each Number A. INDEX TO CONTRIBUTORS Page BAILEY, BRUCE A. Monuments by the Cox Family .. 115- 116 BoND, SHELAGH M. The Plague at Northampton .. 276-277 BROOKE, CHRISTOPHER. The Penury of Christ's Maidservants 10 CLARK, D AVID M. The Northamptonshire Crop Returns for 1801 213- 214 CLARK, SIR GEORGE. The Legend of St. Rumbold ... 131 - 135 ~ENEKE, HELENA. Mary Helen Simpson· 108- 114 GooDMAN, ANTHONY. The Last Basset ofWeldon ... 291-296 HALL, DEREK. Evidence of Fraud at Mediaeval Drayton? 163- 167 HA TLEY, VICTOR A. The Inhuman Taskmasters (Weedon Bee) 30-34 Some Aspects of Northampton's History, 1815-1831 243-253 HooKER, I. M. F. and N. DmilloTT HUNT John Clare: Some Unpublished Documents of the AsylRm Period 190- 198 !SHAM, GYLES A Royalist Squire's Letter on the Eve of the Restoration 11- 14 Andrew Pictures at Delapre 67-70 Two Local Biographies: Owen Ragsdale; Sir John Robinson 81- 91 The Northamptonshire Origins of Alfred Edward Taylor 106- 107 John Clare: The Northampton Years ... 185- 189 Pepys' American Dinner Party, Part I. 263- 269 JACK, R. IAN. A quincentenary: The Battle of Northampton, July 1Oth, 1460 21-25 KING, PATRICK. The 17th Century Census of Cogenhoe 271-273 F.A.L. Drayton House 63-65 MARLOW, NoRMAN. -
Office Address Details.Pdf
Area Name Identifier Office Name Enquiry office no. Office Type Address Line 2 Address Line 3 Address Line 4 Postcode Midlands 2244 ABBERLEY SPDO 01299 896000 SPDO Abberley Delivery Office The Common Worcester WR6 6AY London 1116 ABBEY WOOD SDO 08456 112439 PDO Abbey Wood & Thamesmead Delivery Office Nathan Way London SE28 0AW Wales 871 ABERCARN DO 01495 245025 PDO Abercarn Delivery Office Prince Of Wales Industrial Estate Newport NP11 4AA Wales 236 ABERDARE DO 01685 872007 PDO Aberdare Delivery Office Aberaman Industrial Estate Aberdare CF446ZZ Scotland 985 ABERFELDY SPDO 01887 822835 SPDO Aberfeldy Delivery Office Dunkeld Street Aberfeldy PH152AA Scotland 1785 ABERFOYLE SPDO 01877 382231 SPDO Aberfoyle Delivery Office Main Street Stirling FK8 3UG Wales 880 ABERGAVENNY DO 01873 303500 PDO Abergavenny Delivery Office 1 St. Johns Square Abergavenny NP7 5AZ Scotland 12 ABERLOUR SPDO Wayside Aberlour Delivery Office Elchies Road Aberlour AB38 9AA Wales 874 ABERTILLERY DO 01495 212546 PDO Abertillery Delivery Office Unit 5 Cwmtillery Industrial Estate Abertillery NP131XE Wales 1257 ABERYSTWYTH DO 01970 632600 PDO Glanyrafon Industrial Estate Llanbadarn Fawr Aberystwyth SY23 3GX Thames Valley 934 ABINGDON DO 08456-113-218 PDO Abingdon Delivery Office Ock Street Abingdon OX14 5AD Scotland 8 ABOYNE SPDO 08457740740 SPDO Aboyne Delivery Office Charlestown Road Aboyne AB345EJ North West England 71 ACCRINGTON DO 08456-113-070 PDO Accrington Delivery Office Infant Street Accrington BB5 1ED Scotland 995 ACHARACLE SPDO 01967 431220 SPDO Acharacle -

Hollowell Lodge Farm, Welford Road, Creaton Offers in Excess Of
Freehold Development Opportunity Rural Location, Spectacular Views Derelict Farmhouse & Buildings Approx 2.68 Acres in Total Ideal Site for Executive Homes Subject to Planning Permission Buyer to Apply for Planning Option Agreement Purchase Viewings by Appointment Only Hollowell Lodge Farm, Welford Road, Creaton Offers in Excess of £3,100,000 Freehold Hollowell Lodge Farm, Welford Road, Creaton, Northants. NN6 8NX A rare opportunity to acquire a potential LOCAL AMENITIES: Food shopping facilities can be found approximately 3 miles away in the village of Guilsborough, where there is also a post office, hairdressers development site in open countryside comprising and general stores. Primary schooling is available in Guilsborough where there is a derelict farmhouse and numerous outbuildings, also an academy school and the village of Creaton which also provides a post office and stores. http://www.guilsborough.northants.sch.uk/ There are C of E in a stunning rural location with exceptional churches in Hollowell, Creaton and Guilsborough, sailing at Hollowell reservoir, views across the valley to Hollowell, golf at nearby Cold Ashby and various sports clubs in Creaton and Guilsborough. Guilsborough and the reservoir. Hollowell Lodge HEALTH & SAFETY: The farmhouse and a number of the buildings are in Farm provides approximately 2.68 acres dilapidated condition therefore access to any building is STRICTLY (1.086ha) of 'Brownfield' area which would lend PROHIBITED. There are tripping and other hazards throughout the site itself to the development of substantial individual and neither the Vendors nor their agents will accept responsibility for any injuries howsoever caused. Children are NOT allowed on site. homes, creating an exclusive sustainable development, with excellent access to road and rail networks. -

Flood Investigation Report Creaton Road, Hollowell
DSA DAVID SMITH ASSOCIATESConsulting Structural & Civil Engineers 8 DUNCAN CLOSE MOULTON PARK NORTHAMPTON NN3 6WL TEL: (01604) 782620 FAX: (01604) 782629 email: [email protected] Web: www.dsagroup.co.uk FLOOD INVESTIGATION REPORT CREATON ROAD, HOLLOWELL 27th JULY 2013 Client: Flood & Water Management Team Planning Services Northamptonshire County Council County Hall, Room 271, Northampton NN1 1DN Prepared by: Richard Jones Date: 31st January 2014 Reference: 13/16767 Revision: 04 VAT Registration No.: 670 8636 12 Eur Ing David Smith B.Sc.(Hons), C. Eng., MICE., M I Struct E., R.MaPS, MFPWS Associates: Hitesh B. Jethwa B.Sc.Eng (Civil) Hons, Alison Smith DSA DAVID SMITH ASSOCIATESConsulting Structural & Civil Engineers 8 DUNCAN CLOSE MOULTON PARK NORTHAMPTON NN3 6WL TEL: (01604) 782620 FAX: (01604) 782629 email: [email protected] Web: www.dsagroup.co.uk REVISION SCHEDULE Northamptonshire County Council Flood Investigation Report Creaton Road, Hollowell David Smith Associates Reference : 13/16767 Rev Date Details Author Checked Approved 01 18/10/13 Draft Report Richard Jones Josie Bateman Josie Bateman (David Smith (Senior Project (Senior Project Associates) Manager Manager F&WM) F&WM) 02 21/10/13 Draft Report for Richard Jones Josie Bateman Josie Bateman Stakeholder Consultation (David Smith (Senior Project (Senior Project Associates) Manager Manager F&WM) F&WM) 03 25/11/13 Revision following Richard Jones Josie Bateman Josie Bateman additional (David Smith (Senior Project (Senior Project information/consultation Associates) Manager Manager F&WM) F&WM) 04 31/01/14 Additional contact Richard Jones Josie Bateman Josie Bateman information added. (David Smith (Senior Project (Senior Project Associates) Manager Manager F&WM) F&WM) VAT Registration No.: 670 8636 12 Eur Ing David Smith B.Sc.(Hons), C. -

Northamptonshire Militia Lists 1777: Fawsley Hundred
FAWSLEY HUNDRED Ashby St. Ledgers 24 Hellidon 47 Badby 56 Kilsby 99 Barby 54 Litchborough 32 Braunston 93 Newnham 41 Catesby 19 Norton 50 Charwelton 15 Preston Capes 32 Daventry 379 Staverton 41 Drayton 29 Stowe Nine Churches 30 Dodford 17 Weedon Bec 65 Everdon 44 Welton 60 Farthingstone 26 Fawsley 16 1,269 Apprentice * 19 Grocer 5 Attorney 5 Groom 1 Baker 15 Groom's man 1 Barber 4 Hog dealer 1 Basket-maker 3 Horse-keeper 6 Besom-maker 1 Husbandman 5 Blacksmith 22 Innholder 1 Bookbinder 1 Joiner 12 Brazier 2 Labourer 214 Breeches-maker 3 Labourer (idle) 3 Brickmaker 1 Labourer's son 1 Butcher 18 Land surveyor 2 Cabinet-maker 1 Maltster 5 Carpenter 24 Mason 13 Carpenter's son 1 Miller 8 Carrier 1 Miller's son 4 Carver 3 No trade given 214 Chandler 2 Ostler 3 Clergyman 4 Outrider 1 Clothier 1 Plasterer 1 Cloth-joiner 1 Plumber & glazier 1 Collar-maker 1 Post-chaise driver 7 Cooper 3 Pump-maker 1 Currier 4 Saddler 2 Cutler 2 Schoolmaster 3 Draper 9 Servant 209 Engrossing clerk 1 Shepherd 7 Esquire 2 Shoemaker 32 Farmer 66 Shopkeeper 1 Farmer's son 29 Stationer 1 Fellmonger 8 Stay-maker 1 Flax-dresser 2 Student 17 Framework-knitter 8 Surgeon 2 Gardener 6 Tailor 26 Glazier 3 Tanner 2 Grazier 9 Tinker 1 Grazier's son 10 Turner 1 FAWSLEY HUNDRED 33 Upholsterer 3 Whitesmith 2 Victualler 14 Woodman 1 Waiter 2 Wool-comber 25 Watchmaker 1 , Yeoman 27 Weaver 67 Yeoman's son 2 Weaver's son 1 Wheelwright 6 1,269 Whip-maker 8 • Includes 18 "clerks & apprentices" at Daventry.