KVC-Enrolment-Pack2.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
THE NEW ZEALAND GAZETTE. [No~ 68
2598 THE NEW ZEALAND GAZETTE. [No~ 68 .MILITARY AREA No. 10 (CHRISTCHURCH)-continued. MILITARY AREA No. 11 (DUNEDIN)-oontinued. 453017 White, Alan Rutherford, metal worker, 645 Ferry Rd., 451331 Blanchard, Alfred Herbert, labourer, Duntroon. Christchurch. 451460 Bowie, Robert John, clerk, 82 Duncan St., Dunedin C. 2. .454843 White, Charles Edgar Joseph, foundry worker, 82 Byron St., 450079 Boyd, Jack Thomson, 481 Leith St., Dunedin. Sydenham, Christchurch. · ' 450135 Brinsdon, Allan Stanley, farm labourer, Otakou, via Dunedin. 455169 White, Herbert Alfred James, herd.tester, 14 Windsor Tee., 450530 Brinsdon, Leonard James, farm labourer,· care of Mr.' A. Christchurch. , Chapman, Ika Rd., Oamaru. 454831 Whiteside, Ronald William, painter, 164 Lincoln Rd., 450374 Brown, ]'ergus George Beaumont, student, 118 Bay View Addington, Christchurch. Rd., Dunedin. 452251 Whitta, Neville Bruce, student, 201 Kilmore St., Christ 450588 Brown, John Andrew, carpenter's apprentice, 7 Alexander church. · St., Abbotsford. 456120 Willetts, Douglas, mill· hand, 239 Cashel St.,· Christchurch 455749 Brown, Leslie Hubert, programme-assistant, 151 Albany f1. l. St., Dunedin. 454880 Williams, Defyd Ifor, civil servant, 7 Jutland St., New 452936 Brown, Leslie James, labourer, Kyeburn Diggings, Naseby. Brighton, Christchurch. • 453734 Brown, Malcolm James, clerk, 55 Riselaw Rd., Dunedin. 451918 Williamson, Ernest, farm labourer, Child Welfare Branch, 454836 Bryant, Horace James, apprentice carpenter, Box 114, P.O. Box 105, Timaru. Alexandra. 453499 Wilson, Mervyn Henry, assistant cinematograph-operator, 454818 Buchanan, Thomas Harry, warehouseman,.. 6A Greenock St., 30 Akaroa St., Kaiapoi. Kaikorai, Dunedin. ' ' 453015 Wilson, Raymond Keith, carpenter, 39 Buffon St., Christ 450540 Bull, David Cormack, dental student, care of Mrs. Spence, church. 42 Pinehill Tee., Dunedin. 450919 Wilson, Robert Ferguson, fitter, 66 Bordesley St., Linwood. -

General Distribution and Characteristics of Active Faults and Folds in the Clutha and Dunedin City Districts, Otago
General distribution and characteristics of active faults and folds in the Clutha and Dunedin City districts, Otago DJA Barrell GNS Science Consultancy Report 2020/88 April 2021 DISCLAIMER This report has been prepared by the Institute of Geological and Nuclear Sciences Limited (GNS Science) exclusively for and under contract to Otago Regional Council. Unless otherwise agreed in writing by GNS Science, GNS Science accepts no responsibility for any use of or reliance on any contents of this report by any person other than Otago Regional Council and shall not be liable to any person other than Otago Regional Council, on any ground, for any loss, damage or expense arising from such use or reliance. Use of Data: Date that GNS Science can use associated data: March 2021 BIBLIOGRAPHIC REFERENCE Barrell DJA. 2021. General distribution and characteristics of active faults and folds in the Clutha and Dunedin City districts, Otago. Dunedin (NZ): GNS Science. 71 p. Consultancy Report 2020/88. Project Number 900W4088 CONTENTS EXECUTIVE SUMMARY ...................................................................................................... IV 1.0 INTRODUCTION ........................................................................................................1 1.1 Background .....................................................................................................1 1.2 Scope and Purpose .........................................................................................5 2.0 INFORMATION SOURCES ........................................................................................7 -
Urban Streams
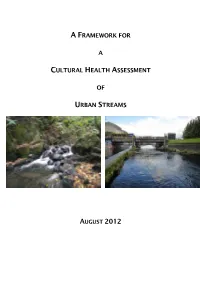
A FRAMEWORK FOR A CULTURAL HEALTH ASSESSMENT OF URBAN STREAMS AUGUST 2012 Cover page photos Left: Ross Creek (in the headwaters of the Leith). Right: the Leith in its Lower Reaches. 2 Table of Contents CHAPTER 1 .........................................................................................................................................................................5 BACKGROUND ......................................................................................................................................................5 RESEARCH OBJECTIVES .....................................................................................................................................6 REPORT STRUCTURE ..........................................................................................................................................6 CHAPTER 2: METHODS ...................................................................................................................................................9 INTRODUCTION ....................................................................................................................................................9 STUDY AREA .........................................................................................................................................................9 METHODOLOGY ....................................................................................................................................................9 QUALITATIVE DATA ANALYSIS ..........................................................................................................................11 -

Surface Water Quality the Water of Leith and Lindsay's Creek Kaikorai
Surface water quality The Water of Leith and Lindsay’s Creek Kaikorai Stream Waitati River and Carey’s Creek © Copyright for this publication is held by the Otago Regional Council. This publication may be reproduced in whole or in part provided the source is fully and clearly acknowledged. ISBN 1-877265-67-5 Published August 2008 Water of Leith, Kaikorai, Waitati and Carey’s Creek i Foreword To help protect water quality, the Otago Regional Council (ORC) carries out long- term water quality monitoring as part of a State of the Environment programme. To supplement this information, targeted and detailed short-term monitoring programmes are also implemented in some catchments. This report provides the results from more detailed investigations carried out in three catchments: Water of Leith Kaikorai Stream Waitati River and Carey’s Creek The Water of Leith and Kaikorai Stream are both located in Dunedin and drain typical residential and industrial areas. Both watercourses have many stormwater outfalls which compromise water quality. The Waitati River and Carey’s Creek have little development in their catchments. The upper catchments are forested while lower in the catchment, pasture dominates. Water quality is generally very good. This report forms a baseline study from which ORC and local community programmes can work together to address various issues in the catchments. It is hoped that these catchment programmes will promote environmentally sound practices which will sustain and improve water quality. Water of Leith, Kaikorai, Waitati and Careys Creek Water of Leith, Kaikorai, Waitati and Carey’s Creek ii Water of Leith, Kaikorai, Waitati and Careys Creek Water of Leith, Kaikorai, Waitati and Carey’s Creek iii Executive summary Between July 2007 and March 2008, the Otago Regional Council (ORC) carried out intensive water quality monitoring programmes in the following catchments: Water of Leith Kaikorai Stream Waitati River and Carey’s Creek The aim of this monitoring was to establish a baseline water quality. -

Report Superseded
Report Superseded The landslide mapping in this report has been superseded by the 2017 report: Revised landslide database for the coastal sector of the Dunedin City district. Please refer to the 2017 document for the most up to date landslide information. Landslide maps and associated information are available online through the ORC’s Natural Hazard Database: https://www.orc.govt.nz/managing-our- environment/natural-hazards/otago-natural- hazards-database Active landslides in the Dunedin area October 2015 Otago Regional Council Private Bag 1954, Dunedin 9054 70 Stafford Street, Dunedin 9016 Phone 03 474 0827 Fax 03 479 0015 Freephone 0800 474 082 www.orc.govt.nz © Copyright for this publication is held by the Otago Regional Council. This publication may be reproduced in whole or in part, provided the source is fully and clearly acknowledged. ISBN 978-0-905324-18-7 Report writer: Ben Mackey, Hazards Analyst (Geologic) Reviewed by: Michael Goldsmith, Manager Natural Hazards Published October 2015 Cover: Abbotsford landslide, 1979. Photo courtesy of Otago Daily Times. Active landslides in the Dunedin area i Overview In this report, existing information relating to the most recently active group of known landslides in Dunedin City has been collated to help inform the review of the Dunedin City District Plan. Three sub-categories within this group of landslides have been determined, with reference made to original source reports. The attributes of approximately 2,100 mapped landslide features in Dunedin City were collated into a database by GNS in 2012 and 2014 (Glassey and Smith Lyttle, 2012; Glassey et al, 2014), hereafter termed the landslide database. -

The New Zealand Gazette. 1795
JUNE 24.] THE NEW ZEALAND GAZETTE. 1795 MILITARY AREA No. 11 (DUNEDIN)-contiwued. MILITARY AREA No. 11 (DUNEDIN)-continued. 517146 Bennett, Albert Sydney Clarence, boxmaker, 176 Helens- 626751 Cairns, William, orchard hand, care of Donaldson, 41 borough Rd., Wakari. College St. 505835 Berry, Ernest Henry, wicker-worker, 82 Forth St. 519188 Caldwell, George, fitter, 22 Eskvale St. 627039 Berry, Gordon Henry, nurseryman, 184 Malvern St., Gardens. 519204 Cameron, Colin Stewart, storeman, 26 Cutten St. 602750 Berry, Harold Francis William, hairdresser, 10 Dee St., 500939 Cameron, Ian Bain, joiner's machinist, 18 Lynu St., Oamaru. Oamaru. 626589 Cameron, Murdoch Martin, farm hand, Hyde. 607083 Berry, Mynot Noel, clerk, 125 Blacks Rd. 519404 Camp, James Thomas, waterside worker, 33 Harrington St., 605557 Berry, Robert James Augustus, police constable, 154 Port Chalmers. Victoria Rd., St. Clair. 500334 Campbell, Arthur Basil, timber machinist, 20 Morrison St. 522418 Berryman, Cyril, coach-painter, 10 Begg St., Roslyn. 506531 Campbell, Arthur John, builder, 41 Kelvin St. 546028 Betts, Clarence Album Sidney, boilermaker, 209A Cargill Rd. 624162 Campbell, Colin Gordon, blue maker, 33A Forth St. 502762 Bingham, Claude Henry, stonemason, 99 Tomahawk Rd., 604843 Campbell, Colin Greek, bus-driver, Dickson St., Macandrew Anderson's Bay. Bay. 498216 Binning, Douglas Sydney, motor mechanic, 115 Lynn St., 500346 Campbell, Gavin Angus, clerk, 3 West Belt, Oamaru. Maori Hill. 579229 Campbell, George Riddell, orchardist, Nga para St., Alexandra. 590196 Bird, Albert John, plumber, 46 Highcliff Rd., Anderson's 559364 Campbell, Gordon, porter (N.Z.R.), Gordon St., Kurow. Bay. 572387 Campbell, Ivan John, manager, 145 Victoria Rd., St. Clair. 484610 Birt, Charles Ernest_, mechanic, 15 Cochrane St. -

October-Informer-2018.Pdf
Greater Green Island Informer October 2018 Greater Green Island Community Recreational Area Development Above left: Playco finish installing the train. Above right: The Carousel is tested by the Community Senior Constable Fred Jansen who is in the GGICN. The Green Island Memorial Gardens was turned into a playground construction zone last month, and the anticipation has Green Island School pupil Lena Walker (6) jumping sky high. “I’m very excited,” Lena said, of the official opening on Friday, October 12th. Greater Green Island Community Network chairman Steve Hayward, along with the Network committee, is thrilled that the development is underway. “It will be a great focal point for families to gather and get together. We are really excited,” he said. The playground would include train-style play equipment for children aged up to 6 years, and had been in the planning for two years. “It’s fenced so it’s safe. It’s going to be using an under utilised area. Everyone has been so positive from the start,” Mr Hayward said. “We are looking forward to the next 12 months, focusing on the family seating and the BBQ area.” The recreational area is being developed in the Green Island Memorial Gardens, Main South Road. Bottom left: Lox Kellas, RSA President and Steve Hayward GGICN Chairperson prepare the first site hole while Lena Walker celebrates. We would like to thank all the businesses and residents who helped make this project happen. The generous community support and enthusiasm has been incredible, and the GGI Community Network would like to extend a warm invitation to the: Official Opening on Friday, October 12th at 12.30pm. -

3.8.13.2 General Comment on Waitati / Doctors Point
3.8.13.2 General comment on Waitati / Doctors Point 1291.The s42A Report noted that Waitati has a primary school, community centre, library, convenience store and a bus service into the city. Large parts of Waitati (but not Doctors Point) are subject to a Hazard 2 Flood overlay, meaning that new development requires resource consent. 1292.The township is not serviced for wastewater, and on-site disposal is required, reflected in a 1,000m2 minimum site size for township and settlement development. The area is serviced by the Northern Pipeline, which is supplied from Mt Grand Water Treatment Plant and provides water to Waitati and sites further north. The scheme does not have capacity for urban expansion, as demonstrated by water shortages in Warrington in 2016. There are currently poor fire flows (WWS Request for Technical Assessment, pp. 5-6). 1293.Submissions were received in relation to 4 sites within the Waitati / Doctors Point area: 135 / 145 Doctors Point Road, 128D Doctors Point Road, 3 Chelivode Street and 974- 1045 Mount Cargill Road. As many of the submitters and issues raised were common for the Doctors Point Road and Chelivode Street sites, the submitters’evidenceontheseis considered together, after the submissions and s42A Report response are summarised. 3.8.13.3 135 and 145 Doctors Point Road, Waitati (Sheet 58) 1294.135 and 145 Doctors Point Road (known as Opeke) are together a 19.51ha block of land, both owned by Willowridge Developments Ltd. The sites are zoned Township and Settlement Zone in the 2GP. The zoning is Rural in the operative Plan. -

Assessment of Liquefaction Hazards in the Dunedin City District D
Assessment of liquefaction hazards in the Dunedin City district D. J. A. Barrell P. J. Glassey S. C. Cox B. Smith Lyttle GNS Science Consultancy Report 2014/068 May 2014 DISCLAIMER This report has been prepared by the Institute of Geological and Nuclear Sciences Limited (GNS Science) exclusively for and under contract to Otago Regional Council. Unless otherwise agreed in writing by GNS Science, GNS Science accepts no responsibility for any use of, or reliance on any contents of this Report by any person other than Otago Regional Council and shall not be liable to any person other than Otago Regional Council, on any ground, for any loss, damage or expense arising from such use or reliance. The data presented in this Report are available to GNS Science for other use from May 2014. BIBLIOGRAPHIC REFERENCE Barrell, D. J. A.; Glassey, P. J.; Cox, S.C.; Smith Lyttle, B. 2014. Assessment of liquefaction hazards in the Dunedin City district, GNS Science Consultancy Report 2014/068. 66 p. Project Number 440W1489-00 CONTENTS EXECUTIVE SUMMARY ......................................................................................................... 1 1.0 INTRODUCTION .......................................................................................................... 3 1.1 BACKGROUND ..................................................................................................... 3 1.2 SCOPE OF WORK UNDERTAKEN ........................................................................... 3 1.3 DATA COLLATION AND REVIEW ........................................................................... -
Recreation in Dunedin Free and Under $5
Recreation in Dunedin Free and under $5 Contents Areas ................................................................................................................. 2 Map .................................................................................................................... 3 Foreword ......................................................................................................... 4 Life's a Beach ................................................................................................... 5 Sport and Exercise ......................................................................................... 7 Stadiums and Sports Centres .................................................................. 8 Volunteering .................................................................................................... 9 Finding out more .......................................................................................... 13 Eat Fresh and Grow Your Own ............................................................... 16 Dunedin Community Gardens .............................................................. 16 Where did you get that dress? ................................................................. 18 The Octagon Club ....................................................................................... 20 Central Dunedin .......................................................................................... 21 North ............................................................................................................. -

Heritage Walks.Pub
Josephine in Otago Settlers Museum Museum Settlers Otago in Josephine was the contractor. contractor. the was strengthening and W H Naylor Naylor H W and strengthening www.ipenz.org.nz/heritage Structural Engineer for the the for Engineer Structural Southland. Southland. in 1990. J R G Hanlon was the the was Hanlon G R J 1990. in in Otago & & Otago in technology and industry engineering, in achievements Recognising replaced with stainless steel rods rods steel stainless with replaced Services. Recreation & Community DCC and Museum Settlers Otago rods in 1964/65 and these were were these and 1964/65 in rods nce from from nce assista with Chapter Otago Heritage Engineering (IPENZ) neers ssional Engi- ssional Profe of Institution The by produced been has brochure This strengthened with galvanised tie tie galvanised with strengthened remainder solid. The tower was was tower The solid. remainder thirds of its height, with the the with height, its of thirds spire being hollow for about two two about for hollow being spire were similarly constructed, the the constructed, similarly were 500mm thick. The tower and spire spire and tower The thick. 500mm stone, making a solid wall about about wall solid a making stone, are of brick, lined with Oamaru Oamaru with lined brick, of are The exterior walls of the church church the of walls exterior The for 1,000 people. people. 1,000 for had to be rebuilt. The church opened in 1873 and has seating seating has and 1873 in opened church The rebuilt. be to had the spire was slightly out of perpendicular and 4.6 m too short so so short too m 4.6 and perpendicular of out slightly was spire the The spire is 53 m high. -

Property ID Address Property Name Area Removed
Property ID Address Property Name Area removed (sq m) 5010100 27 St Leonards Drive St Leonards Property: St Leonards Hall 934 5010243 47 Harrier Road St Leonards Water: St Leonards Water Storage Tank 740 5010259 15 Burkes Drive Ravensbourne Reserve: Burkes Recreation Reserve 5111 5010260 21 Burkes Drive Ravensbourne Waste: Former Burkes-St Leonard Treament Plant 1900 5010544 5 Gerrys Road Ravensbourne Water: Gerrys Road Water Storage Tank 1142 5010700 5 Wanaka Street Ravensbourne Property: Ravensbourne Hall 1015 5010741 14 Ellesmere Street Ravensbourne Water: Ellesmere St Water Storage Tank 1006 5010920 188 Ravensbourne Road Ravensbourne Property: 884 5011751 55 Campbells Road Dunedin Water: Pine Hill Water Storage Tank 754 5012519 PT SEC 6 Cleghorn Street Dunedin Reserve: Stevensons Bush Scenic Reserve 56211 5012539 588 North Road Dunedin Water: Mt Mera Water Storage Tank 753 5012588 210 Blacks Road Dunedin Water: Signal Hill Water Storage Tank 11510 5012719 133 Blacks Road Dunedin Roading: Right of Way 452 5012738 10A Grandview Crescent Dunedin Roading: Drainage Right 154 5013163 LOT 4 Craigleith Street Dunedin Waste: Part Bed of Lindsays Creek 233 5014018 24 Cornhill Street Dunedin Reserve: Chacombe Avenue Reserve 110 5014127 34 Buccleugh Street Dunedin Reserve: Buccleugh Street Reserve 13741 5014128 30 Buccleugh Street Dunedin Housing: Buccleugh Street Community Housing 3390 5014146 LOT 1 North Road Dunedin Waste: Part Bed of Lindsays Creek 489 5014333 2 Leith Valley Road Dunedin Waste: Part Bed Leith Stream 6915 5014390 174 Malvern