Kentucky's Largest Health Plan Adopts
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

November/December 2013
AMERICAN BICYCLIST ADVENTURES 2014 VENUS DE MILES: IN BICYCLING RIDE GUIDE RISING ABOVE Four tales of freedom From charity rides to Riders in Colorado from the road, rail multi-day tours, get help victims of recent and trail p. 12 rolling in 2014 p. 20 floods p. 18 November - December 2013 WWW.BIKELEAGUE.ORG AMERICAN BICYCLIST CONTENT November — December 2013 LEAGUE BOARD ELECTION 8 CAST YOUR VOTE! Help determine who will represent you on the League board. FROM THE SADDLE 12 ADVENTURES IN BICYCLING Four tales of freedom from the road, rail and trail. WOMEN BIKE 18 VENUS DE MILES 2013: RISING ABOVE Colorado ride evolves into a community service event that helps victims of devastating floods. Tour de Cure 2014 RIDE GUIDE 20 100+ RIDES FOR RIDERS OF ALL IN EVERY ISSUE SKILL LEVELS From charity rides to multi-day tours, get rolling 02 VIEWPOINT in 2014! 03 INBOX 04 COGS&GEARS 28 QUICKSTOP AMERICAN BICYCLIST IS PRINTED WITH SOY INK ON 30% POST-CONSUMER RECYCLED PAPER CERTIFIED BY RAINFOREST ALLIANCE TO THE FOREST STEWARDSHIP COUNCIL™ STANDARDS. ON THE COVER Erica Lighthiser with children Eva, Clara and Emmett (and dog, Hayduke) on their 2013 bike adventure. VIEWPOINT RIDE GUIDE: YOUR WAY TO A BRIGHTER FUTURE A two-week bicycle tour in the Brittany Re- 300 advocacy organizations, together with gion of France changed my life. the members of the Bicycle Tour Network, I was 19 years old and was re-taking a offer an extraordinary community service rather unspectacular first year at the Uni- in organizing rides to suit every possible versity of Birmingham when the idea was taste and level of riding. -

Economic Impact Study of Bicycling in Arizona Out-Of-State Bicycle Tourists & Exports
An Economic Impact Study of Bicycling in Arizona Out-of-State Bicycle Tourists & Exports FINAL REPORT APPENDIX PREPARED FOR: MPD 64-12 CONTRACT NO. ADOT11-013181 PREPARED BY: McClure Consulting LLC 2944 N. 44th Street, Suite 101 Phoenix, AZ 85018 Economic & Policy Resources, Inc. 400 Cornerstone Drive, Suite 310 Williston, VT 05495 Kimley-Horn and Associates, Inc. 333 East Wetmore Road, Suite 280 Tucson, AZ 85705 June 2013 ACKNOWLEDGEMENTS PREPARED FOR ARIZONA DEPARTMENT OF TRANSPORTATION CONTRACT NO: ADOT11-013181 TECHNICAL ADVISORY COMMITTEE (TAC) TAC members included representatives from the diverse set of stakeholders below: ADOT, Communications ADOT, Multimodal Planning Division (MPD), Bicycle and Pedestrian Program ADOT, MPD, Transportation Analysis ADOT, MPD, Research Center ADOT, MPD, Tribal Transportation Arizona Office of Tourism Arizona State Parks Federal Highway Administration – Arizona Division MPOs and COGs KEY INFORMANTS The authors appreciate the input of Key Informants who were contacted for this study and agreed to be interviewed in order to provide additional insight into the study approach and processes. In addition to the persons listed below, other individuals offered informal opinions, and these contributions were also appreciated. Tom Armstrong, Cochise Bicycle Advocates Bob Beane, Coalition of Arizona Bicyclists Wayne Cullop, Greater Arizona Bicycling Association Richard DeBernardis, President, Perimeter Bicycling Association of America Karen Lamberton, Cochise County Transportation Planner Mike -
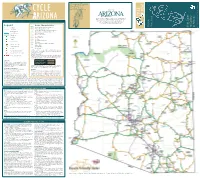
2009 Cycle Arizona Bicycle User
Arizona Department of Transportation 206 S. 17th Ave., Mail Drop 310B Phoenix, AZ 85007 ransportation T email: [email protected] of website: http://www.azbikeped.org Supported by CYCLE Department Arizona RIZONA the by CYCLE Arizona in Subscribe to Arizona Highways magazine for a monthly guide to RIZONA Arizona’s best places to visit, hike, drive, sightsee and dine. Plus bicycling you’ll find the extraordinary scenic photography that has made of Map Arizona Highways magazine a world-wide favorite. Guide To subscribe visit www.arizonahighways.com interest Cycling the Arizona Legend Route Characteristics in Bicycle User Your to in Effective Shoulder Width = 4 ft or greater Stateline Published Effective Shoulder Width < 4 ft County Line Rumble Strip with Effective Shoulder Width < 4 ft Rivers & Streams Bridge with Effective Shoulder Width < 4 ft Lakes & Reservoirs Low Traffic Volumes National Park Medium Traffic Volumes High Traffic Volumes State Park Bicycles Prohibited Campsite Dirt Roads Interstate Frontage Roads Point of Interest Other Roads Regionally Significant Routes (Non-ADOT) National Monument Extreme Grade Tourist Information Moderate Grade Rest Area Varied Grade Facilities conditions as shown on this map often vary from one side Population less than 1,000 of the road to the other. Bicyclists should use extreme caution while riding on Arizona highways. Population greater than 1,000 TRAFFIC VOLUMES Distance Between Points All traffic volumes on this map are Annual Average Daily Traffic (AADT). AADT is the total number of vehicles passing a given point, in both directions, during a year, divided by 365 days, given in vehicles per day (vpd). -

View Sanofi Sponsorships and Charitable Donations
2015 SANOFI US Legal Name Project Title Payment Amount A R M S Inc Homecoming & Project Little Soldier $5,000.00 Academy of Managed Care Pharmacy Improving patient outcomes and management of hyperlipidem $45,000.00 ACS Organic Chemistry Division Graduate Research Symposium $1,000.00 AHIP Foundation Executive Leadership Program $55,000.00 Alabama Kidney Foundation 2015 Huntsville Kidney Walk $1,000.00 Alabama Kidney Foundation 2015 Birmingham Kidney Walk $1,000.00 Alabama Kidney Foundation Dothan Kidney Walk $1,000.00 Albany American Diabetes Association Saratoga Springs Tour de Cure $5,000.00 ALL IN TOGETHER CAMPAIGN INC All in Together Campaign: Advancing and Empowering Women $37,500.00 Allergy & Asthma Network Mothers of Asthmatics US Anaphylaxis Summit $30,000.00 Allergy & Asthma Network Mothers of Asthmatics AAP Anaphylaxis Champions Program $100,000.00 Allergy & Asthma Network Mothers of Asthmatics Allergy & Asthma Day Capitol Hill 2015 $50,000.00 Alliance For A Healthier Generation Inc Alliance for a Healthier Generation $25,000.00 Alliance for Aging Research 2015 Aging in Motion Coalition $15,000.00 Amerian Diabetes Association AMerican Diabetes Association Diabetes Health and Wellness Ex $2,500.00 American Academy of Pediatrics-Key Cards American Academy of Pediatrics Key Card Sponsorship $35,000.00 AMERICAN ASSOCIATION FOR CANCER RESEARCH 2015 AACR Annual Meeting MICR Networking and Resource Cen $10,000.00 AMERICAN ASSOCIATION FOR CANCER RESEARCH 2015 AACR Network Hubs Sponsorship $ 25,000.00 American Cancer Society ACS CAN Seattle -

Editors' Comments Table of Contents
April/May 2016 Volume 9 Issue 2 Editors ’ Comments Table of Contents Sharon Boyd & Dale Campbell: To go directly to an article, click on the Article Title Editors Prez Says Colorado Springs Rallies around Bicycling With the Appointment of a Bike Coordinator Comes Goals and Challenges CSCC – 30 Years and Still Riding! CSCC – What Does It Mean to You? Calculating the Experience of Riding a Bike Colorado Commuters Bike More Than Almost Any Other State Get ready to Start the 2016 National Bike Challenge Have Any Travel Plans for 2016? Here ’ s an Idea! This is definitely the time of the year that can be a challenge to A Coalition of Cyclists Brings More Than Just our desire to be out and on a Coordination! bicycle. In just this past week, Here ’ s another Source for Ride Planning across the U S for example, there have been of A clear warm days with little wind Special Activities & Rides of Interest! and temps in the 60s/70s. And Colorado Springs Cycles Forward to Stop Diabetes then – WAM! – there comes that day (or days) with multiple Mountain Bikers Taking Notice of New Cycling Hot Spot inches of snow, wind chills in the in Southern Colorado teens and winds of over 30 Ever Wonder Why Something ’ s Not Quite Right with mph. So what do we do on the New Bike those days? Get on the Editors ’ Comments trainer? Look at cycling web Come See the Covered Velodrome at the April Club pages? Watch a cycling movie? Meeting! Try to wait out Mother Nature, Have You Checked Your Miles for 2016? while she decides to present a real Spring, -

LOCAL EVENT GUIDE Greater Philadelphia Tour De Cure Saturday, June 4, 2016 Ambler, PA
LOCAL EVENT GUIDE Greater Philadelphia Tour de Cure Saturday, June 4, 2016 Ambler, PA Local ADA Office, Route Descriptions…. American Diabetes Associati on 150 Monument Road, Suite 100, Bala Cynwyd, PA 19004 Tour de Cure Local Staff: Meredith Charney Alison Carey Tel: 610-864-2599 Tel: (732) 469-7979 x3519 [email protected] [email protected] Location, Directions, Fundraising Tips, Mobile Red Riders, Champions , What to Bring, Safety Parking, Schedule .... 2 App, Social Media………. 3 Team Red….................. 4-5 Information, FAQ …. 6-8 Thank you for registering for the June 4th Greater Philadelphia Tour de Cure! We’re celebrating the 25th Anniversary of the Tour de Cure and we want you to be a part of this incredible day. Since 1991, Tour de Cure riders have raised over $250 million to help advance our mission and move us closer towards the ultimate goal to Stop Diabetes! The Tour de Cure is more than just a cycling event. It’s a day packed with excitement and energy where riders of all levels join forces in the fight to Stop Diabetes® and raise critical funds for diabetes research, education and advocacy in support of the American Diabetes Association. We promise to go the extra mile to make sure your experience is memorable, and we’re gearing up for another exciting event by offering all the extras you can expect from a Tour de Cure event including breakfast & lunch, scenic route choices for all types of riders, medical and on-course support, well-stocked rest stops, and a finish line festival full of fun and activities. -

Tour De Cure 2012 Events by State Draft As of 1‐13‐2012
Tour de Cure 2012 Events by State Draft as of 1‐13‐2012 State Event Date City State State Event Date City State Alabama 5/12/12 Hoover (Birmingham) AL Missouri 6/23/12 Republic MO Alaska 6/3/2012 Eagle River (Anchorage) AK Montana 9/15/12 Three Forks MT 6/9/2012 Fairbanks AK Nebraska 6/3/12 Springfield NE 3/4/12 Tucson AZ 4/14/12 Henderson (Las Vegas) NV Arizona Nevada 3/24/12 Phoenix AZ New Jersey 6/3/12 Basking Ridge NJ Arkansas 4/14/12 Little Rock AR 6/24/12 Princeton NJ 10/6/12 Springdale AR 9/15/12 Brielle (Jersey Shore) NJ 4/21/12 Cardiff (San Diego) CA 6/2/12 Bernalillo (Albuquerque) NM California New Mexico 4/29/12 Long Beach (Los Angeles) CA 9/17/12 Farmington NM 5/5/12 Roseville (Sacramento) CA New York 6/2/12 Sanborn (Buffalo) NY 5/6/12 Yountville CA 6/3/12 Verona Beach NY (Utica/Syracuse) 6/10/12 Palo Alto (Silicon Valley) CA 6/3/12 Saratoga Springs NY (Albany) 9/29/12 Costa Mesa (Orange CA 6/3/12 New York NY County) 11/10/12 Santa Barbara CA 6/9/12 Riverhead NY Woodland Park (Colorado 6/10/12 Rochester NY Colorado 6/16/2012 Springs) CO 8/18/12 Longmont (Denver) CO 8/18/12 Watkins Glen NY (Montour Falls) Connecticut 6/10/12 North Haven CT North Carolina 6/2-3/2012 Cary (Raleigh) NC Delaware 5/12/12 Newark DE North Dakota 6/16/12 Fargo (Moorhead) ND 6/3/12 DC Area (Reston) VA 6/9/12 Westerville (Columbus) OH Dist. -

Baltimore Bicycling Club Newsletter
Baltimore Bicycling Club Newsletter INDEX Volume 40 Number 1 January | February 2007 Committees . .2 BBC 2006 Event Calender . .3 Out of Bounds . .4-5 End of Season Celebration . .6 BBC Club Awards . .7 BBC Executive Board . .8 Ride Leaders . .9 2006 Sponsors Thanks . .10 Event Leaders . .11 Pedel in Style . .12 Tour de Montes . .13 Kent County Spring Fling . .14 Gourmet Meals & Lodging . .15 Spring Fling Registration . .16 Event Waiver . .17 Winter Weight Gain . .18-19 One Less Car . .20 Ride Start locations . .21-23 Jan & Feb Ride Schedule . .24-29 Ride Descriptions & BBC Talk .30-31 Upcoming Events January 20 Crabs Potluck To make sure you continue to get your Newsletter and membership renewal notices, please let us know if any of your membership information changes. You can do this by sending an e-mail to [email protected], or go on the Web site to the Member Update page (http://www.baltobikeclub.org/index.pl/update), complete the form, and submit it. Baltimore Bicycling Club, Inc P.O. Box 5894 Baltimore, MD 21282-5894. www.baltimorebicyclingclub.org 2007 Officers & Members-at-Large of the Board The BBC is governed by an Executive Board (consisting of a President, Vice President, Treasurer, Secretary, four mem- bers-at-large, and the Past President) which meets monthly to discuss club business. If you would like more information, please 2007 Committees call the current BBC President. For a syn- opsis of the minutes, call the Secretary. Insurance . .Howard Rosenbaum . .410-653-2363 Government Relations . .Bob Moore . .410-435-6623 Officers Bob Carson, President Instructional Programs . -

The Pittsburgh Tour De Cure – Ride.Run.Walk
Welcome to the Pittsburgh Tour de Cure – Ride.Run.Walk. Saturday, September 14, 2019 INSIDE: What to Expect .............. 1 Check In & Start Times . 1 Route Info ...................... 2 Start/Finish Line Fun ..... 2 Day of Event Info .......... 3 Rider Markings & Safety 4 What to Bring ................ 4 FAQs .............................. 5 Tour de Cure Sponsors . 6 The Pittsburgh Tour de Cure: Ride. Run. Walk. is taking place on September 14, 2019 allowing participants to "choose their move" through a 12/30/63 mile bike ride, 5k walk, or 5k run. You’re training and fundraising to support the ADA’s mission - now you’re CHECK IN & START TIMES ready to have some fun! Tour de Cure is an exciting day and the more prepared you are, the better time you’ll have. 63 Miles Ride Check in starts at 6:00 a.m. START / FINISH LINE Route starts at 7:00 a.m. Route markings will be RED South Shore Riverfront Park, 2701 S Water St, Pittsburgh, PA 15203 *12-15 mph average pace (next to the Hofbräuhaus ) 30 Miles Packet Pick Up Check-in starts at 7:00 a.m. Route starts at 8:00 a.m. • Thursday, Sept 12th 3-7pm at South Side Works Cinema 425 Cinema Dr, Pittsburgh Route markings will be GREEN *9 mph average pace Fundraising Minimums: Participants must raise the fundraising minimum to participate. 12 Miles • Check-in starts at 8:30 a.m. Cyclists: Registration Fee & $200 fundraising minimum; Children riding 12 and Route starts at 9:30 a.m. under $50 Route markings will be BLUE • Walkers/Runners: No registration fee & $100 fundraising minimum; Children 12 *5 mph average pace and under free 5K FUN Run Check-in starts at 9:00 a.m. -

0 Sponsorship Opportunities
Sponsorship Opportunities 10 JUNE 20, 20 National Capital Tour de Cure Reston Town Center Reston, Virginia What is Tour de Cure? American Diabetes Association Tour de Cure is a signature fundraising event of the The American Diabetes Association is the nation’s leading 501(c)(3) American Diabetes Association- a premier cycling event non-profit health organization providing diabetes research, held in 80 locations in 33 states. Last year, more than information, and advocacy. Founded in 1940, the American 33,000 participants raised over $13 million to support the Diabetes Association funds research, publishes scientific findings, and mission of the ADA. Tour de Cure is a ride- not a race!- provides information and other services to people with diabetes, with routes designed for everyone from the recreational their families, health professionals and the public. The Association is rider to the experienced cyclist. The 2010 Tour de Cure also actively involved in advocating for scientific research and for will take place on on June 20, 2010 at the Reston Town the rights of people with diabetes. Center in Reston, Virginia. Tour de Cure is a unique opportunity for companies, organizations, and families to come together to fight diabetes, raise awareness, OUR MISSION and build a sense of community. Particpants will choose from 6 scenic routes (1-12, 17, 20 33, 63, and 100 The mission of the American Diabetes Association is to miles), supported from start to finish with rest stops, food prevent and cure diabetes to and improve the lives of to fuel the journey, and inspiring stories of those who all people affected by diabetes. -

Helping People See the World Through Different Eyes
Helping people see the world through different eyes... 6C Newsletter - December 2017 DG Steve Kinsky Chronology of a Lions Event Here’s a mini-chronicle of the Community Strides Walk for Diabetes held on Saturday, November 18. In reviewing what we did at each step along the way, I’m able to uncover some valuable information pertaining to the Walk that might make future ones more productive. August 14: I receive the Diabetes Awareness article for the MD6 Newsletter from Cyber’s Janice Smith and Chatfield’s Carol Louks. The article notes the American Diabetes Association (ADA) Tour de Cure event in early September and its Camp for Type 1 diabetes-afflicted youth, a JDRF fundraiser, some LCI tips on how to conduct a diabetes screening program and a blurb about women and diabetes. September 9: I attend Tour de Cure in Parker. Janice and I do the 3 mile walk. I notice numerous other diabetes advocacy organizations with booths. The event also features a bike ride with varying lengths - one as much as 100 kilometers. While we walk, Janice tells me of her annual Strides Walk for Diabetes. September 14: Several of us meet at the ADA offices in the Highlands to discuss how to organize a District-wide Community Strides Walk that would combine the best of ADA and LCI resources to raise money for diabetes. We conclude that the best way to do so would be to feature the young campers at the Type 1 Camp in Wood- land Park. September 15: The Mane Lioner mentions a planned presentation on diabetes treatment to be conducted at the Trinity United Methodist Church in downtown Denver. -

Thank You for Registering for the May 18, 2013 Alabama Tour De Cure!
Location, Directions, Tour de Cure Coordinator: American Diabetes Association: Parking, Schedule .......... 2 Aimee Johnson 3918 Montclair Road, Suite 218 Tel: 205.870.5172X3070 Birmingham, AL 35213 Fundraising Tips, Mobile Email: [email protected] Fax: 205.879.2903 App, Social Media .......... 3 Red Riders, Champions of Diabetes, Team Red ....... 4 What to Bring, Safety Information, FAQ ........... 5-7 Thank you for registering for the May 18, 2013 Alabama Tour de Cure! Thank you for doing your part to Stop Diabetes by registering for the Tour de Cure. We’re looking forward to the biggest and best Tour de Cure yet and it’s promising to be a fantastic event! We have improved routes, increased safety & medical support and have an extraordinary post-ride party planned for the finish line! This guide contains information to help you prepare for the Tour de Cure and tips to ensure you have a great experience on the day of the ride. It’s fun, it’s fabulous and most importantly it’s for a great cause – raising funds in support of the nearly 26 million Americans living with diabetes and their families. Route Descriptions The Alabama Tour de Cure begins at St. Vincent’s 119, located at 7191 Cahaba Valley Road, Hoover, AL 35242. Our 5 routes are designed to appeal to all skill levels. Routes include: 20 Mile Ride Our 20 Mile Ride offers a moderate challenge while being safe and scenic. There is a rest stop at the half-way mark and plenty of SAG patrols, which make this ride a great choice for the beginner cyclist! 37 Mile Ride (50K) Our 37 Mile Ride offers a moderate challenge while being safe and scenic.