Review Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The National Drugs List
^ ^ ^ ^ ^[ ^ The National Drugs List Of Syrian Arab Republic Sexth Edition 2006 ! " # "$ % &'() " # * +$, -. / & 0 /+12 3 4" 5 "$ . "$ 67"5,) 0 " /! !2 4? @ % 88 9 3: " # "$ ;+<=2 – G# H H2 I) – 6( – 65 : A B C "5 : , D )* . J!* HK"3 H"$ T ) 4 B K<) +$ LMA N O 3 4P<B &Q / RS ) H< C4VH /430 / 1988 V W* < C A GQ ") 4V / 1000 / C4VH /820 / 2001 V XX K<# C ,V /500 / 1992 V "!X V /946 / 2004 V Z < C V /914 / 2003 V ) < ] +$, [2 / ,) @# @ S%Q2 J"= [ &<\ @ +$ LMA 1 O \ . S X '( ^ & M_ `AB @ &' 3 4" + @ V= 4 )\ " : N " # "$ 6 ) G" 3Q + a C G /<"B d3: C K7 e , fM 4 Q b"$ " < $\ c"7: 5) G . HHH3Q J # Hg ' V"h 6< G* H5 !" # $%" & $' ,* ( )* + 2 ا اوا ادو +% 5 j 2 i1 6 B J' 6<X " 6"[ i2 "$ "< * i3 10 6 i4 11 6! ^ i5 13 6<X "!# * i6 15 7 G!, 6 - k 24"$d dl ?K V *4V h 63[46 ' i8 19 Adl 20 "( 2 i9 20 G Q) 6 i10 20 a 6 m[, 6 i11 21 ?K V $n i12 21 "% * i13 23 b+ 6 i14 23 oe C * i15 24 !, 2 6\ i16 25 C V pq * i17 26 ( S 6) 1, ++ &"r i19 3 +% 27 G 6 ""% i19 28 ^ Ks 2 i20 31 % Ks 2 i21 32 s * i22 35 " " * i23 37 "$ * i24 38 6" i25 39 V t h Gu* v!* 2 i26 39 ( 2 i27 40 B w< Ks 2 i28 40 d C &"r i29 42 "' 6 i30 42 " * i31 42 ":< * i32 5 ./ 0" -33 4 : ANAESTHETICS $ 1 2 -1 :GENERAL ANAESTHETICS AND OXYGEN 4 $1 2 2- ATRACURIUM BESYLATE DROPERIDOL ETHER FENTANYL HALOTHANE ISOFLURANE KETAMINE HCL NITROUS OXIDE OXYGEN PROPOFOL REMIFENTANIL SEVOFLURANE SUFENTANIL THIOPENTAL :LOCAL ANAESTHETICS !67$1 2 -5 AMYLEINE HCL=AMYLOCAINE ARTICAINE BENZOCAINE BUPIVACAINE CINCHOCAINE LIDOCAINE MEPIVACAINE OXETHAZAINE PRAMOXINE PRILOCAINE PREOPERATIVE MEDICATION & SEDATION FOR 9*: ;< " 2 -8 : : SHORT -TERM PROCEDURES ATROPINE DIAZEPAM INJ. -

Drotrecogin Alfa (Activated)
PRODUCT MONOGRAPH PrXIGRIS® drotrecogin alfa (activated) Sterile Powder for Intravenous Injection 5 mg or 20 mg drotrecogin alfa (activated) per vial Antithrombotic Profibrinolytic Anti-Inflammatory Enzyme © ELI LILLY CANADA INC. Date of Approval: 3650 Danforth Avenue August 20, 2009 Toronto, Ontario M1N 2E8 1-888-545-5972 www.lilly.ca Submission Control No: 128989 XIGRIS [drotrecogin alfa (activated)] Page 1 of 36 Product Monograph Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION......................................................... 3 SUMMARY PRODUCT INFORMATION ....................................................................... 3 INDICATIONS AND CLINICAL USE............................................................................. 3 CONTRAINDICATIONS .................................................................................................. 4 WARNINGS AND PRECAUTIONS................................................................................. 4 ADVERSE REACTIONS................................................................................................... 8 DRUG INTERACTIONS ................................................................................................. 12 DOSAGE AND ADMINISTRATION ............................................................................. 13 OVERDOSAGE ............................................................................................................... 16 ACTION AND CLINICAL PHARMACOLOGY ........................................................... 16 STORAGE -

Kengrexal, INN-Cangrelor Tetrasodium
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Kengrexal 50 mg powder for concentrate for solution for injection/infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each vial contains cangrelor tetrasodium corresponding to 50 mg cangrelor. After reconstitution 1 mL of concentrate contains 10 mg cangrelor. After dilution 1 mL of solution contains 200 micrograms cangrelor. Excipient with known effect Each vial contains 52.2 mg sorbitol. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Powder for concentrate for solution for injection/infusion. White to off-white lyophilised powder. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Kengrexal, co-administered with acetylsalicylic acid (ASA), is indicated for the reduction of thrombotic cardiovascular events in adult patients with coronary artery disease undergoing percutaneous coronary intervention (PCI) who have not received an oral P2Y12 inhibitor prior to the PCI procedure and in whom oral therapy with P2Y12 inhibitors is not feasible or desirable. 4.2 Posology and method of administration Kengrexal should be administered by a physician experienced in either acute coronary care or in coronary intervention procedures and is intended for specialised use in an acute and hospital setting. Posology The recommended dose of Kengrexal for patients undergoing PCI is a 30 micrograms/kg intravenous bolus followed immediately by 4 micrograms/kg/min intravenous infusion. The bolus and infusion should be initiated prior to the procedure and continued for at least two hours or for the duration of the procedure, whichever is longer. At the discretion of the physician, the infusion may be continued for a total duration of four hours, see section 5.1. -
Efficacy Claims and Subset Analyses in Phase III: Some Thoughts and Examples
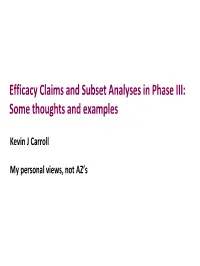
Efficacy Claims and Subset Analyses in Phase III: Some thoughts and examples Kevin J Carroll My personal views, not AZ’s Why do we do them? • Fundamentally, because we can, and we feel compelled to do so. • Yet, we have no agreed framework for the conduct and interpretation of such analyses, nor for their potential implications on product labelling and drug approval. • Of interest to consider the use and utility of subgroup analyses in confirmatory Phase III trials where such analyses are intended: 1. To provide an assessment of internal ‘consistency’ in an trial with an overall positive outcome. 2. By design to formally assess a hypothesis of efficacy in a predefined subset. 3. To salvage a negative trial. 2 The persuasiveness of subset analyses in confirmatory trials PIII trial Not designed to formally Designed to formally assess efficacy in subset assess efficacy in subset Overall result Overall result Co-primary Subset as part positive negative popln, divided of hierarchical alpha formal confirmatory Multiple Post-hoc • Subset exploratory subsets not testing analyses •Subset +ve procedure subsets identified in weakest of identified in advance • label claim even evidence if overall –ve advance • Extremely •Subset +ve difficult to use • label claim • Subset as basis for •Susbet -ve • Looking for defined in approval. • Overall ‘consistency’ response to positive • Grps that data • May be some • Label claim ‘benefit the most • possibly after very limited possible for / least’ regulatory circumstances overall? • Not a matter of rejection where proving efficacy, • How to conditional but obvious respond to approval can potential to such data? be considered impact on with post- labelling approval commitment 3 1. -

Heparin Induced Thrombocytopenia – Adult – Inpatient– Clinical Practice Guideline
Heparin Induced Thrombocytopenia – Adult – Inpatient– Clinical Practice Guideline Table of Contents EXECUTIVE SUMMARY ........................................................................................................... 2 SCOPE ...................................................................................................................................... 6 METHODOLOGY ...................................................................................................................... 6 DEFINITIONS (OPTIONAL): ..................................................................................................... 7 INTRODUCTION ....................................................................................................................... 7 RECOMMENDATIONS .............................................................................................................. 7 BENEFITS/HARMS OF IMPLEMENTATION ...........................................................................17 IMPLEMENTATION PLAN AND TOOLS ........................ERROR! BOOKMARK NOT DEFINED. REFERENCES .........................................................................................................................17 APPENDIX A ............................................................................................................................17 Note: Active Table of Contents Click to follow link CPG Contact for Changes: CPG Contact for Content: Name: Philip J Trapskin, PharmD,BCPS Name: Anne E. Rose, PharmD Phone Number: 263-1328 Phone Number: -

Modifications to the Harmonized Tariff Schedule of the United States To
U.S. International Trade Commission COMMISSIONERS Shara L. Aranoff, Chairman Daniel R. Pearson, Vice Chairman Deanna Tanner Okun Charlotte R. Lane Irving A. Williamson Dean A. Pinkert Address all communications to Secretary to the Commission United States International Trade Commission Washington, DC 20436 U.S. International Trade Commission Washington, DC 20436 www.usitc.gov Modifications to the Harmonized Tariff Schedule of the United States to Implement the Dominican Republic- Central America-United States Free Trade Agreement With Respect to Costa Rica Publication 4038 December 2008 (This page is intentionally blank) Pursuant to the letter of request from the United States Trade Representative of December 18, 2008, set forth in the Appendix hereto, and pursuant to section 1207(a) of the Omnibus Trade and Competitiveness Act, the Commission is publishing the following modifications to the Harmonized Tariff Schedule of the United States (HTS) to implement the Dominican Republic- Central America-United States Free Trade Agreement, as approved in the Dominican Republic-Central America- United States Free Trade Agreement Implementation Act, with respect to Costa Rica. (This page is intentionally blank) Annex I Effective with respect to goods that are entered, or withdrawn from warehouse for consumption, on or after January 1, 2009, the Harmonized Tariff Schedule of the United States (HTS) is modified as provided herein, with bracketed matter included to assist in the understanding of proclaimed modifications. The following supersedes matter now in the HTS. (1). General note 4 is modified as follows: (a). by deleting from subdivision (a) the following country from the enumeration of independent beneficiary developing countries: Costa Rica (b). -

Statistical Analysis Plan – Part 1
NCT03251482 Janssen Research & Development Statistical Analysis Plan – Part 1 A Randomized, Double-blind, Double-dummy, Multicenter, Adaptive Design, Dose Escalation (Part 1) and Dose-Response (Part 2) Study to Evaluate the Safety and Efficacy of Intravenous JNJ-64179375 Versus Oral Apixaban in Subjects Undergoing Elective Total Knee Replacement Surgery Protocol 64179375THR2001; Phase 2 JNJ-64179375 Status: Approved Date: 18 October 2017 Prepared by: Janssen Research & Development, LLC Document No.: EDMS-ERI-148215770 Compliance: The study described in this report was performed according to the principles of Good Clinical Practice (GCP). Confidentiality Statement The information in this document contains trade secrets and commercial information that are privileged or confidential and may not be disclosed unless such disclosure is required by applicable law or regulations. In any event, persons to whom the information is disclosed must be informed that the information is privileged or confidential and may not be further disclosed by them. These restrictions on disclosure will apply equally to all future information supplied to you that is indicated as privileged or confidential. 1 Approved, Date: 18 October 2017 JNJ-64179375 NCT03251482 Statistical Analysis Plan - Part 1 64179375THR2001 TABLE OF CONTENTS TABLE OF CONTENTS ............................................................................................................................... 2 LIST OF IN-TEXT TABLES AND FIGURES ............................................................................................... -

Anticoagulation Dosing Guideline for Adult COVID-19 Patients
Anticoagulation Dosing Guideline for Adult COVID-19 Patients Enoxaparin is the preferred first line anticoagulant for patients diagnosed with COVID-19. The incidence of HIT with enoxaparin is less than 1%. VTE Prophylaxis: VTE prophylaxis will be considered for COVID-19 patients who are low risk. Low risk COVID-19 patient 1. Not receiving mechanical ventilation 2. D-Dimer < 6 mg/L 3. ESRD on iHD without clotting Kidney Function BMI (kg/m2) Dosing of Enoxaparin Concern for HIT or LMWH Failure CrCL ≥ 30 mL/min 18.5-39.9 30mg SUBQ Q12H Consult Hematology 40-49.9 40mg SUBQ Q12H ≥ 50 60mg SUBQ Q12H CrCL < 30 mL/min 18.5-39.9 30mg SUBQ Q24H Consult Hematology OR ≥ 40 40mg SUBQ Q24H ESRD/AKI on RRT Special Population: < 18.5 (or weight < 50kg) Heparin 2500 SUBQ Q8H Consult Hematology *Contraindications: Platelets < 25 K/uL or Fibrinogen < 50 mg/dL or active bleeding Therapeutic anticoagulation Therapeutic anticoagulation will be considered for COVID-19 patients who are considered high risk or diagnosed with an acute VTE. High risk COVID-19 patient (for all hospitalized patients): Receiving mechanical ventilation AND D-dimer > 6 mg/L OR Acute kidney injury (Scr increase 0.3 mg/dL above baseline) +/- CVVHD/AVVHD/SLED or IHD with clotting Anti-Xa level goals for enoxaparin therapy (when indicated): 1. Therapeutic peak LMWH level (Drawn 4 hours after 3rd dose): 0.6-1 anti-Xa units/mL 2. Therapeutic trough LMWH level (Drawn 1 hour prior to 3rd dose): < 0.5 anti-Xa units/mL Kidney Function BMI Dosing of Enoxaparin Concern for HIT or (kg/m2) LMWH -

Transition of Anticoagulants 2019
Transition of Anticoagulants 2019 Van Hellerslia, PharmD, BCPS, CACP, Brand Generic Clinical Assistant Professor of Pharmacy Practice, Angiomax bivalirudin Temple University School of Pharmacy, Philadelphia, PA Arixtra fondaparinux Bevyxxa betrixaban Pallav Mehta, MD, Assistant Professor of Medicine, Coumadin warfarin Division of Hematology/Oncology, Eliquis apixaban MD Anderson Cancer Center at Cooper, Camden, NJ Fragmin dalteparin Lovenox enoxaparin Reviewer: Kelly Rudd, PharmD, BCPS, CACP, Pradaxa dabigatran Clinical Specialist, Anticoagulation, Bassett Medical Center, Savaysa edoxaban Cooperstown, NY Xarelto rivaroxaban From To Action Apixaban Argatroban/ Wait 12 hours after last dose of apixaban to initiate parenteral anticoagulant. In cases of Bivalirudin/ high bleeding risk, consider omitting initial bolus when transitioning to heparin infusion. Enoxaparin/ Dalteparin/ Fondaparinux/ Heparin Apixaban Warfarin When going from apixaban to warfarin, consider the use of parenteral anticoagulation as a bridge (eg, start heparin infusion or therapeutic enoxaparin AND warfarin 12 hours after last dose of apixaban and discontinue parenteral anticoagulant when INR is therapeutic). Apixaban affects INR so that initial INR measurements during the transition may not be useful for determining the appropriate dose of warfarin. Apixaban Betrixaban, Wait 12 hours from last dose of apixaban to initiate betrixaban, dabigatran, edoxaban, or Dabigatran, rivaroxaban. Edoxaban, or Rivaroxaban Argatroban Apixaban, Start apixaban, betrixaban, dabigatran, -

Legemiddelforbruket I Norge 2012–2016 Drug Consumption in Norway 2012–2016
2017:1 LEGEMIDDELSTATISTIKK EVT STIKKTITTEL INN HER Legemiddelforbruket i Norge 2012–2016 Drug Consumption in Norway 2012–2016 ISSN 1890-9647 Legemiddelforbruket i Norge 2012–2016 Drug Consumption in Norway 2012–2016 Solveig Sakshaug Hanne Strøm Christian Berg Hege Salvesen Blix Irene Litleskare Tove Granum Utgitt av Folkehelseinstituttet / Published by Norwegian Institute of Public Health Området for Psykisk og fysisk helse Avdeling for Legemiddelepidemiologi Mars 2017 Tittel/Title: Legemiddelstatistikk 2017:1 Legemiddelforbruket i Norge 2012-2016/Drug Consumption in Norway 2012-2016 Forfattere/Authors: Solveig Sakshaug (redaktør) Hanne Strøm Christian Berg Hege Salvesen Blix Irene Litleskare Tove Granum Bestilling/Order: Rapporten kan lastes ned som pdf på Folkehelseinstituttets nettsider: www.fhi.no/ The report is available as pdf format only and can be downloaded from the www.fhi.no Layout omslag: www.fetetyper.no Kontaktinformasjon/Contact information Folkehelseinstituttet/Norwegian Institute of Public Health P.O.Box 4404 Nydalen N-0403 Oslo Tel: +47 21 07 70 00 ISSN: 1890-9647 ISBN 978-82-8082-826-2 elektronisk utgave Sitering/Citation: Sakshaug, S (red), Legemiddelforbruket i Norge 2012-2016 [Drug Consumption in Norway 2012-2016], Legemiddelstatistikk 2017:1, Oslo: Folkehelseinstituttet, 2017. Tidligere utgaver/Previous editions: 1977: Legemiddelforbruket i Norge 1974 - 1976 1978: Legemiddelforbruket i Norge 1975 - 1977 1980: Legemiddelforbruket i Norge 1975 - 1979 1981: Legemiddelforbruket i Norge 1980 1982: Legemiddelforbruket -

Handbook of Drugs in Intensive Care: an A
This page intentionally left blank This page intentionally left blank Handbook of Drugs in Intensive Care Fourth edition This book is dedicated to Georgina Paw Handbook of Drugs in Intensive Care An A-Z Guide Fourth edition Henry G W Paw BPharm MRPharmS MBBS FRCA Consultant in Anaesthesia and Intensive Care York Hospital York Rob Shulman BSc (Pharm) MRPharmS Dip Clin Pham, DHC (Pharm) Lead Pharmacist in Critical Care University College London Hospitals London CAMBRIDGE UNIVERSITY PRESS Cambridge, New York, Melbourne, Madrid, Cape Town, Singapore, São Paulo, Delhi, Dubai, Tokyo Cambridge University Press The Edinburgh Building, Cambridge CB2 8RU, UK Published in the United States of America by Cambridge University Press, New York www.cambridge.org Information on this title: www.cambridge.org/9780521757157 © H. Paw and R. Shulman 2010 This publication is in copyright. Subject to statutory exception and to the provision of relevant collective licensing agreements, no reproduction of any part may take place without the written permission of Cambridge University Press. First published in print format 2010 ISBN-13 978-0-521-75715-7 Paperback Cambridge University Press has no responsibility for the persistence or accuracy of urls for external or third-party internet websites referred to in this publication, and does not guarantee that any content on such websites is, or will remain, accurate or appropriate. CONTENTS Introduction vii How to use this book viii Abbreviations x Acknowledgements xiii DRUGS: An A–Z Guide 1 SHORT NOTES 229 Routes of -
Antithrombotic Agents in the Management of Sepsis
Antithrombotic Agents in the Management of Sepsis !"#$ Loyola University Medical Center, Maywood, Illinois-60153, USA ABSTRACT Sepsis, a systemic inflammatory syndrome, is a response to infection and when associated with mul- tiple organ dysfunction is termed, severe sepsis. It remains a leading cause of mortality in the critically ill. The response to the invading bacteria may be considered as a balance between proinflammatory and antiinflammatory reaction. While an inadequate proinflammatory reaction and a strong antiinflammatory response could lead to overwhelming infection and death of the patient, a strong and uncontrolled pro- inflammatory response, manifested by the release of proinflammatory mediators may lead to microvas- cular thrombosis and multiple organ failure. Endotoxin triggers sepsis by releasing various mediators inc- luding tumor necrosis factor-alpha and interleukin-1(IL-1). These cytokines activate the complement and coagulation systems, release adhesion molecules, prostaglandins, leukotrienes, reactive oxygen speci- es and nitric oxide (NO). Other mediators involved in the sepsis syndrome include IL-1, IL-6 and IL-8; arachidonic acid metabolites; platelet activating factor (PAF); histamine; bradykinin; angiotensin; comp- lement components and vasoactive intestinal peptide. These proinflammatory responses are counterac- ted by IL-10. Most of the trials targeting the different mediators of proinflammatory response have failed due a lack of correct definition of sepsis. Understanding the exact pathophysiology of the disease will enable better treatment options. Targeting the coagulation system with various anticoagulant agents inc- luding antithrombin, activated protein C (APC), tissue factor pathway inhibitor (TFPI) is a rational appro- ach. Many clinical trials have been conducted to evaluate these agents in severe sepsis.