Acute Toxicity Following Analytically Confirmed Use of the Novel Psychoactive Substance (NPS) Methiopropamine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

How Pre-Clinical Studies Have Influenced Novel Psychoactive Substance Legislation in the UK and Europe
Article How preclinical studies have influenced novel psychoactive substance legislation in the UK and Europe Santos, Raquel, Guirguis, Amira and Davidson, Colin Available at http://clok.uclan.ac.uk/31793/ Santos, Raquel ORCID: 0000-0003-3129-6732, Guirguis, Amira and Davidson, Colin ORCID: 0000-0002-8180-7943 (2020) How preclinical studies have influenced novel psychoactive substance legislation in the UK and Europe. British Journal Of Clinical Pharmacology, 86 (3). pp. 452-481. ISSN 0306-5251 It is advisable to refer to the publisher’s version if you intend to cite from the work. http://dx.doi.org/10.1111/bcp.14224 For more information about UCLan’s research in this area go to http://www.uclan.ac.uk/researchgroups/ and search for <name of research Group>. For information about Research generally at UCLan please go to http://www.uclan.ac.uk/research/ All outputs in CLoK are protected by Intellectual Property Rights law, including Copyright law. Copyright, IPR and Moral Rights for the works on this site are retained by the individual authors and/or other copyright owners. Terms and conditions for use of this material are defined in the policies page. CLoK Central Lancashire online Knowledge www.clok.uclan.ac.uk How Pre-Clinical Studies Have Influenced Novel Psychoactive Substance Legislation in The UK and Europe Raquel Santos1, Amira Guirguis2 & Colin Davidson1* 1School of Pharmacy & Biomedical Sciences, Faculty of Clinical & Biomedical Sciences, University of Central Lancashire, UK. 2Swansea University Medical School, Institute of Life Sciences 2, Swansea University, Swansea, Wales, UK. *Corresponding author Colin Davidson School of Pharmacy and Biomedical Science Faculty of Clinical & Biomedical Sciences University of Central Lancashire Preston PR1 2HE +44 (0)1772 89 3920 [email protected] Key words: novel psychoactive substance, legal high, legislation, toxicity, abuse Running Head: review of NPS pharmacology The authors have no conflicts of interest to declare Page | 1 Abstract Novel psychoactive substances (NPS) are new drugs of abuse. -
Overview of the Misuse of Drugs Act 1971
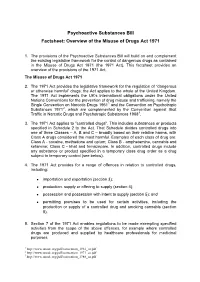
Psychoactive Substances Bill Factsheet: Overview of the Misuse of Drugs Act 1971 1. The provisions of the Psychoactive Substances Bill will build on and complement the existing legislative framework for the control of dangerous drugs as contained in the Misuse of Drugs Act 1971 (the 1971 Act). This factsheet provides an overview of the provisions of the 1971 Act. The Misuse of Drugs Act 1971 2. The 1971 Act provides the legislative framework for the regulation of “dangerous or otherwise harmful” drugs; the Act applies to the whole of the United Kingdom. The 1971 Act implements the UK’s international obligations under the United Nations Conventions for the prevention of drug misuse and trafficking, namely the Single Convention on Narcotic Drugs 19611 and the Convention on Psychotropic Substances 19712, which are complemented by the Convention against Illicit Traffic in Narcotic Drugs and Psychotropic Substances 19883. 3. The 1971 Act applies to "controlled drugs". This includes substances or products specified in Schedule 2 to the Act. That Schedule divides controlled drugs into one of three Classes – A, B and C – broadly based on their relative harms, with Class A drugs considered the most harmful. Examples of each class of drug are: Class A - cocaine, methadone and opium; Class B - amphetamine, cannabis and ketamine; Class C - khat and temazepam. In addition, controlled drugs include any substance or product specified in a temporary class drug order as a drug subject to temporary control (see below). 4. The 1971 Act provides for a range of offences in relation to controlled drugs, including: • importation and exportation (section 3); • production, supply or offering to supply (section 4); • possession and possession with intent to supply (section 5); and • permitting premises to be used for certain activities, including the production or supply of a controlled drug and smoking cannabis (section 8). -

Peakal: Protons I Have Known and Loved — Fifty Shades of Grey-Market Spectra
PeakAL: Protons I Have Known and Loved — Fifty shades of grey-market spectra Stephen J. Chapman* and Arabo A. Avanes * Correspondence to: Isomer Design, 4103-210 Victoria St, Toronto, ON, M5B 2R3, Canada. E-mail: [email protected] 1H NMR spectra of 28 alleged psychedelic phenylethanamines from 15 grey-market internet vendors across North America and Europe were acquired and compared. Members from each of the principal phenylethanamine families were analyzed: eleven para- substituted 2,5-dimethoxyphenylethanamines (the 2C and 2C-T series); four para-substituted 3,5-dimethoxyphenylethanamines (mescaline analogues); two β-substituted phenylethanamines; and ten N-substituted phenylethanamines with a 2-methoxybenzyl (NBOMe), 2-hydroxybenzyl (NBOH), or 2,3-methylenedioxybenzyl (NBMD) amine moiety. 1H NMR spectra for some of these compounds have not been previously reported to our knowledge. Others have reported on the composition of “mystery pills,” single-dose formulations obtained from retail shops and websites. We believe this is the first published survey of bulk “research chemicals” marketed and sold as such. Only one analyte was unequivocally misrepresented. This collection of experimentally uniform spectra may help forensic and harm-reduction organizations identify these compounds, some of which appear only sporadically. The complete spectra are provided as supplementary data.[1] Keywords: 1H NMR, drug checking, grey markets, research chemicals, phenylethanamines, N-benzyl phenylethanamines, PiHKAL DOI: http://dx.doi.org/10.16889/isomerdesign-1 Published: 1 August 2015 Version: 1.03 “Once you get a serious spectrum collection, Nevertheless, an inherent weakness of grey markets is the the tendency is to push it as far as you can.”1 absence of regulatory oversight. -

Temporary Class Drug Order Report: 5-6APB and Nbome Compounds
ACMD Advisory Council on the Misuse of Drugs Chair: Professor Les Iversen Secretary: Rachel Fowler 3rd Floor (SW), Seacole Building 2 Marsham Street London SW1P 4DF Tel: 020 7035 0555 [email protected] Home Secretary Rt Hon. Theresa May MP Home Office 2 Marsham Street London SW1P 4DF 29 May 2013 Dear Home Secretary, I am writing to formally request that you consider laying a temporary class drug order (TCDO) pursuant to section 2A of the Misuse of Drugs Act 1971 on the following two groups of novel psychoactive substances (NPS). We consider the laying of TCDOs is appropriate as a pre-emptive measure in advance of the summer music festival season. Both classes of drugs have been associated with serious harm and drug-related deaths. ‘Benzofury’ compounds 5- and 6-APB and related substances are phenethylamine-type materials, related to ecstasy (MDMA). There have been several deaths and hospitalisations in the UK associated with these NPS, although poly-substance use often complicates the case. Research indicates that there is a potential risk of cardiac toxicity associated with the long-term use of 5- and 6-APB. Anecdotal user reports suggest that the consumption of these substances can cause insomnia, increased heart rate and anxiety, with some users reporting MDMA like symptoms. The related compound 5-IT has been subject to an EMCDDA-Europol joint report and an EMCDDA risk assessment exercise. [www.emcdda.europa.eu/publications/joint-reports/5- IT] 1 The substances recommended for control are: 5- and 6-APB: (1-(benzofuran-5-yl)-propan-2-amine and 1-(benzofuran-6-yl)-propan- 2-amine) and their N-methyl derivatives. -
CREW Booklet
PSYCHOACTIVE DRUGS V2.1 12/16 SERVICE AVAILABILITY Drop-in Monday – Wednesday: 1pm – 5pm Thursday: 3pm – 7pm Friday – Saturday: 1pm – 5pm Sunday: Closed Telephone information Monday – Friday: 10am – 5pm Online information: www.mycrew.org.uk CONTACT Address | 32 Cockburn Street, Edinburgh, EH1 1PB Telephone | 0131 220 3404 Email | [email protected] Main | www.crew2000.org.uk Enterprise | www.mindaltering.co.uk Info and support | www.mycrew.org.uk Facebook | www.facebook.com/Crew2000 Twitter | www.twitter.com/Crew_2000 Instagram | www.instagram.com/Crew_2000 Psychoactive drugs have mind altering properties. They are often consumed to produce a wide range of desirable physical and psychological effects and there are hundreds of substances available. Psychoactive drugs can occur naturally (e.g. cannabis and psilocybin); be extracted from natural sources (e.g. cocaine and heroin) or produced synthetically (man-made) in a laboratory (e.g. MDMA and methamphetamine). People choose to take drugs for many reasons including relaxation, insomnia, pain relief, escapism, peer pressure and social norms, to get high, self-medication, to have fun, to lower inhibitions, to feel different, because they want to, to increase connection with others and music, to increase creativity, increase sexual arousal, curiosity, tradition, religious or spiritual beliefs, to lose/gain weight, to cope with grief, loneliness, trauma etc. People from all strata of society have the potential to consume drugs and we must avoid stereotypes. Most drug use is recreational and not recorded; however, pockets of problematic use exist in a range of settings. The use of drugs is widespread and includes not just illegal substances but alcohol, nicotine, caffeine and medicines - which many people do not consider to be drugs. -

Advisory Council on the Misuse of Drugs Chair: Professor Les Iversen Secretary: Rachel Fowler 3Rd Floor Seacole Building 2
ACMD Advisory Council on the Misuse of Drugs Chair: Professor Les Iversen Secretary: Rachel Fowler 3rd Floor Seacole Building 2. Marsham Street London SW1P 4DF 020 7035 0454 Email: [email protected] Rt Hon. Theresa May MP Home Office 2 Marsham Street London SW1P 4DF 18th October 2012 Dear Home Secretary, In March 2012 the ACMD advised that methoxetamine be subject to a temporary class drug order. Methoxetamine was marketed as a legal alternative to ketamine until a temporary class drug order was implemented in April 2012. As is now required, the ACMD has followed its initial assessment with a consideration of methoxetamine in the context of the Misuse of Drugs Act 1971; I enclose the report with this letter. The chemical structure of methoxetamine bears a close resemblance to that of both ketamine and phencyclidine (PCP, „Angel Dust‟, a class A drug), which both produce well- documented and serious adverse effects following both acute and chronic usage. Users report that the effects of methoxetamine are similar to those of ketamine, however, some users report that the effects are of longer duration.The harmful effects reported include severe dissociation, cardiovascular symptoms, paranoid thoughts and unpleasant hallucinations. The first analytically confirmed series reported by Guy‟s and St Thomas‟ NHS Foundation Trust, London in 2011, was of three individuals who presented having self-reported use of methoxetamine. All three presented with a ketamine-like dissociative state, but also had significant stimulant effects with agitation and cardiovascular effects including tachycardia and hypertension. Toxicological screening of serum samples confirmed methoxetamine use in two of the cases. -

CREW NPS Booklet
NEW Psychoactive DRUGS V1.7 05/15 Service availability Drop-in: Monday – Wednesday: 1pm – 5pm, Thursday: 3pm – 7pm, Friday – Saturday: 1pm – 5pm, Sunday: Closed Telephone information and support: Monday – Friday: 10am – 5pm Online information and chatroom support: www.mycrew.org.uk Address | 32 Cockburn Street | Edinburgh | EH1 1PB Telephone | 0131 220 3404 Email | [email protected] Main | www.crew2000.org.uk Enterprise | www.mindaltering.co.uk Info and support | www.mycrew.org.uk Facebook | www.facebook.com/Crew2000 Twitter | www.twitter.com/Crew_2000 Instagram | www.instagram.com/Crew_2000 This booklet has been designed to expand worker knowledge and confidence in the area of NPS. It is most useful when discussed as part of Crew’s NPS training. Crew was established in 1992, in response to the rapid expansion of recreational drug use. We provide up-to-date information on the drugs that people are taking so they can make informed decisions about their own health. This is achieved using a stepped care approach and through collaboration with volunteers, service users and professionals. Crew neither condemns nor condones drug use, but we believe there are ways to reduce harm to health. As a national agency, Crew is at the forefront of emerging drug trends and we engage at all levels including service development, practice and policy. Our services include: – Support line: non-judgmental drug and sexual health information and support. – Drop-in: drug and sexual health information, condoms (NHS c:card service) and DJ workshops. – Outreach services: we provide welfare at large events, such as clubs and festivals to educate revellers on partying safely. -

A Chemical Analysis Examining the Pharmacology of Novel Psychoactive Substances Freely Available Over the Internet and Their Impact on Public (Ill) Health
Open Access Research A chemical analysis examining the pharmacology of novel psychoactive substances freely available over the internet and their impact on public (ill) health. Legal highs or illegal highs? Tammy C Ayres,1,2 John W Bond3 To cite: Ayres TC, Bond JW. ABSTRACT ARTICLE SUMMARY A chemical analysis Objectives: Public Health England aims to improve the examining the pharmacology nation’s health and acknowledges that unhealthy Article focus of novel psychoactive lifestyles, which include drug use, undermine society’s - substances freely available To analyse the chemical composition of health and well-being. Recreational drug use has over the internet and their substances bought over the internet, including impact on public (ill)health. changed to include a range of substances sold as the legality of the active ingredients and if Legal highs or illegal highs? ‘research chemicals’ but known by users as ‘legal highs’ products differ between retailers. BMJ Open 2012;2:e000977. (legal alternatives to the most popular illicit recreational - To consider the medical implications and adverse doi:10.1136/ drugs), which are of an unknown toxicity to humans and health risks associated with legal highs bought bmjopen-2012-000977 often include prohibited substances controlled under the over the internet. Misuse of Drugs Act (1971). Consequently, the long- term effects on users’ health and inconsistent, often Key messages < Prepublication history for illegal ingredients, mean that this group of drugs - The most recent examination of the composition this paper is available online. presents a serious risk to public health both now and in of ‘legal highs’, conducted 6 months after the To view these files please the future. -
Methiopropamine (MPA) Critical Review Report Agenda Item 4.8
Methiopropamine (MPA) Critical Review Report Agenda Item 4.8 Expert Committee on Drug Dependence Thirty-eighth Meeting Geneva, 14-18 November 2016 38th ECDD (2016) Agenda item 4.8 MPA Page 2 of 21 38th ECDD (2016) Agenda item 4.8 MPA Contents Acknowledgements .......................................................................................................................... 5 Summary .......................................................................................................................................... 6 1. Substance identification .................................................................................................... 7 A. International Nonproprietary Name (INN) ........................................................................ 7 B. Chemical Abstract Service (CAS) Registry Number .......................................................... 7 C. Other Chemical Names ...................................................................................................... 7 D. Trade Names ...................................................................................................................... 7 E. Street Names ...................................................................................................................... 7 F. Physical Appearance .......................................................................................................... 7 G. WHO Review History ......................................................................................................... 7 2. -

Next Generation of Novel Psychoactive Substances on the Horizon – A
Drug and Alcohol Dependence 157 (2015) 1–17 Contents lists available at ScienceDirect Drug and Alcohol Dependence j ournal homepage: www.elsevier.com/locate/drugalcdep Review Next generation of novel psychoactive substances on the horizon – A complex problem to face ∗ Jolanta B. Zawilska , Dariusz Andrzejczak Department of Pharmacodynamics, Medical University of Lodz, Poland a r t i c l e i n f o a b s t r a c t Article history: Background: The last decade has seen a rapid and continuous growth in the availability and use of novel Received 14 May 2015 psychoactive substances (NPS) across the world. Although various products are labeled with warnings Received in revised form “not for human consumption”, they are intended to mimic psychoactive effects of illicit drugs of abuse. 30 September 2015 Once some compounds become regulated, new analogues appear in order to satisfy consumers’ demands Accepted 30 September 2015 and at the same time to avoid criminalization. This review presents updated information on the second Available online 9 October 2015 generation of NPS, introduced as replacements of the already banned substances from this class, focusing on their pharmacological properties and metabolism, routes of administration, and effects in humans. Keywords: Methods: Literature search, covering years 2013–2015, was performed using the following keywords Novel psychoactive substances alone or in combination: “novel psychoactive substances”, “cathinones”, “synthetic cannabinoids”, Synthetic cannabimimetics Cathinones “benzofurans”, “phenethylamines”, “2C-drugs”, “NBOMe”, “methoxetamine”, “opioids”, “toxicity”, and Psychostimulants “metabolism”. NBOMe compounds Results: More than 400 NPS have been reported in Europe, with 255 detected in 2012–2014. The most Methoxetamine popular are synthetic cannabimimetics and psychostimulant cathinones; use of psychedelics and opioids Psychedelics is less common. -

Is the Main Law on Drug Classification in the UK. It Classifies Drugs B
Misuse of Drugs Act (1971) is the main law on drug The Psychoactive Substances Act (2016) has come into classification in the UK. It classifies drugs by the degree of force on 26 May 2016. social harm. The most severe crimes can be punished with a Under the PSA it is an offence to Produce, Supply, Offer to life sentence and unlimited fine. supply, Possess with intent to supply, or Possess on custodial It is amended to add new substances as evidence on their premises and to Import or Export Psychoactive Substances i.e. harm is gathered. Temporary Class Drug Orders (TCDO’s) can any substance intended for human consumption that is capable 24 January 2017 be placed on substances which are suspected to be harmful of producing psychoactive effects. It carries a maximum while evidence is gathered to support classification. sentence of up to 7 years and unlimited fine. Class A Drugs Class B Drugs Class C Drugs Produced on Max. Possession: 7 years & fine Possession: 5 years & fine Possession: 2 years & fine Penalty Supply: life & fine MoDA(1971) Supply: 14 years & fine MoDA(1971) Supply: 14 years & fine MoDA(1971) LSD Cannabis Anabolic steroids LSD related substances Synthetic Cannabinoids GHB and GBL - Tryptamines - Mephedrone (Meow Meow) Khat AMT (Banned Oct 2014) - ‘Spice’/’Black Mamba’ containing MSJ 5-MeO–DALT AM-2201 or UR-144 Tranquilisers and Benzodiazepines (Banned Jan 2015) Amphetamines including - ALD-52, AL-LAD, ETH-LAD, PRO- Barbiturates - Rohypnol, LAD and LSZ Codeine - Diazepam, (Banned Jan 2015) Naphyrone – ‘Rave’, ‘NRG1’, ‘NRG-1’, - Temazepam, Heroin ‘Energy1’, ‘Energy-1’ - Phenazepam Heroin related substances 2-DPMP, D2PM and - AH7921 (opiate derivative) diphenylmethylpyrrolidine (stimulant Banned Oct 2014 found in ‘Ivory Wave’ NPS) Cocaine Methoxetamine (MXE) Magic Mushrooms Ketamine Crack Benzofuran Compounds Ecstasy - Benzo Fury, White Pearl, 6-APDB, PMA 6-APB, 5-APDB, 5-APB (Banned Methadone 10/06/2014) Methylphenidate (Ritalin) (unless prescribed). -

New Psychoactive Substances – Evidence Review
New Psychoactive Substances – Evidence Review Crime and Justice NEW PSYCHOACTIVE SUBSTANCES – EVIDENCE REVIEW Fiona Fraser, Safer Communities Analytical Unit, Scottish Government Scottish Government Social Research 2014 This report is available on the Scottish Government Publications Website (http://www.scotland.gov.uk/Publications/Recent). The views expressed in this report are those of the researcher and do not necessarily represent those of the Scottish Government or Scottish Ministers. © Crown copyright 2014 You may re-use this information (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit http://www.nationalarchives.gov.uk/doc/open-government-licence/ or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU, or e-mail: [email protected] EXECUTIVE SUMMARY Introduction This paper summarises key information on New Psychoactive Substances (NPS) and evidence gaps. Data on Scotland is presented in the context of UK and international evidence. Definition of NPS In the UK, the Advisory Council on the Misuse of Drugs (ACMD) defines ‘new psychoactive substances’ as: “psychoactive drugs which are not prohibited by the United Nations Single Convention on Narcotic Drugs or by the Misuse of Drugs Act 1971, and which people are seeking for intoxicant use”. Although not scheduled under the UN drug control conventions, a number of the NPS mentioned in this paper are now controlled in the UK (e.g. mephedrone, BZP, NBOMe and Benzofury). Main types of NPS available The number of NPS available is constantly changing and growing which makes it difficult to identify levels and risks of use and for health and enforcement agencies to respond.