Determination of Concentration of Nifekalant in Human Plasma By
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinical Study of the Acute Effects of Intravenous Nifekalant on the Defibrillation Threshold in Patients with Persistent and Paroxysmal Atrial Fibrillation
Circ J 2008; 72: 76–80 Clinical Study of the Acute Effects of Intravenous Nifekalant on the Defibrillation Threshold in Patients With Persistent and Paroxysmal Atrial Fibrillation Kaoru Okishige, MD; Hiroki Uehara, MD; Naoto Miyagi, MD; Kentarou Nakamura, MD; Kouji Azegami, MD; Hirofumi Wakimoto, MD; Kageyuki Ohba, MD; Kenzo Hirao, MD*; Mitsuo Shimabukuro, MD**; Mistuaki Isobe, MD* Background Antiarrhythmic agents are considered to have significant effects on the defibrillation energy re- quirement, so this study investigated the effects of nifekalant on defibrillation. Methods and Results Forty-two patients with persistent atrial fibrillation (AF) underwent electrical cardiover- sion via intracardiac electrode catheters prior to and after the intravenous administration of nifekalant. The suc- cess rate of the defibrillation and change in the defibrillation threshold using sequential incremental defibrillation energy deliveries was investigated. In addition, the parameters that could predict the beneficial effects of nifekalant were also assessed. Nifekalant significantly decreased the defibrillation energy requirement in 13 of the 42 cases, and nifekalant also converted AF to sinus rhythm with an identical energy to that of the last unsuccessful defib- rillation in 21 of 42 cases. The success of defibrillation seemed to be dependent on significant prolongation of the intracardiac atrial electrogram intervals during AF by the nifekalant. Conclusions Intravenous nifekalant significantly improved the electrical defibrillation efficacy in patients with persistent -

ILCOR Guidelines 2015 for Web.Pdf
Supplement to Circulation 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations Dallas, Texas February 1–3, 2015 Editors Mary Fran Hazinski (AHA) Jerry P. Nolan (ERC) International Liaison Committee on Resuscitation (ILCOR) Editorial Board Vinay M. Nadkarni (ILCOR Co-Chair, AHA) Eddy Lang (Grade Expert, HSFC) Gavin D. Perkins (ILCOR Co-Chair, ERC) Swee Han Lim (RCA) William H. Montgomery (C2015 Consensus Ian K. Maconochie (ERC) Conference Coordinator, AHA) Peter T. Morley (Evidence Monica E. Kleinman (Conference Evaluation Expert, ANZCOR) Co-Chair, AHA) Nikolaos I. Nikolaou (ERC) Maaret Castren (Conference Co-Chair, ERC) Robert W. Neumar (AHA) Richard Aickin (COI Co-Chair, ERC) Jeffrey M. Perlman (AHA) John E. Billi (COI Co-Chair, AHA) Eunice M. Singletary (AHA) Farhan Bhanji (HSFC) Jasmeet Soar (ERC) Clifton W. Callaway (AHA) Andrew H. Travers (HSFC) Allan R. de Caen (HSFC) Michelle Welsford (HSFC) Judith C. Finn (ANZCOR) Jonathan Wyllie (ERC) Lana M. Gent (AHA) David A. Zideman (ERC) Participating ILCOR Resuscitation Councils 2015 ILCOR Honorees Acknowledgments American Heart Association (AHA) Tom P. Aufderheide Alicia G. Pederson Australian and New Zealand Committee on Karl B. Kern Russell E. Griffin Resuscitation (ANZCOR) Vinay M. Nadkarni Jose Maria E. Ferrer European Resuscitation Council (ERC) Jerry P. Nolan Mandy L. Cootes Heart and Stroke Foundation of Canada (HSFC) Roger D. White Kara Robinson InterAmerican Heart Foundation (IAHF) Jody Hundley Resuscitation Council of Asia (RCA) Sandra Iverson Resuscitation Council of Southern Africa (RCSA) Joe Loftin We acknowledge the considerable contributions made by the late Professor Ian Jacobs, PhD, to this 2015 International Consensus on CPR Science. -
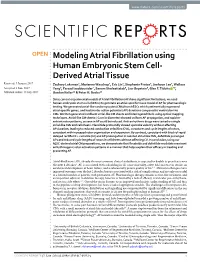
Modeling Atrial Fibrillation Using Human Embryonic Stem Cell
www.nature.com/scientificreports OPEN Modeling Atrial Fibrillation using Human Embryonic Stem Cell- Derived Atrial Tissue Received: 9 January 2017 Zachary Laksman1, Marianne Wauchop2, Eric Lin3, Stephanie Protze4, Jeehoon Lee5, Wallace Accepted: 1 June 2017 Yang6, Farzad Izaddoustdar7, Sanam Shafaattalab8, Lior Gepstein9, Glen F. Tibbits 10, Published: xx xx xxxx Gordon Keller11 & Peter H. Backx12 Since current experimental models of Atrial Fibrillation (AF) have significant limitations, we used human embryonic stem cells (hESCs) to generate an atrial-specific tissue model of AF for pharmacologic testing. We generated atrial-like cardiomyocytes (CMs) from hESCs which preferentially expressed atrial-specific genes, and had shorter action potential (AP) durations compared to ventricular-like CMs. We then generated confluent atrial-like CM sheets and interrogated them using optical mapping techniques. Atrial-like CM sheets (~1 cm in diameter) showed uniform AP propagation, and rapid re- entrant rotor patterns, as seen in AF could be induced. Anti-arrhythmic drugs were tested on single atrial-like CMs and cell sheets. Flecainide profoundly slowed upstroke velocity without affecting AP duration, leading to reduced conduction velocities (CVs), curvatures and cycle lengths of rotors, consistent with increased rotor organization and expansion. By contrast, consistent with block of rapid delayed rectifier +K currents (Ikr) and AP prolongation in isolated atrial-like CMs, dofetilide prolonged APs and reduced cycle lengths of rotors in cell sheets without affecting CV. In conclusion, using our hESC-derived atrial CM preparations, we demonstrate that flecainide and dofetilide modulate reentrant arrhythmogenic rotor activation patterns in a manner that helps explain their efficacy in treating and preventing AF. -

The Use of Stems in the Selection of International Nonproprietary Names (INN) for Pharmaceutical Substances
WHO/PSM/QSM/2006.3 The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances 2006 Programme on International Nonproprietary Names (INN) Quality Assurance and Safety: Medicines Medicines Policy and Standards The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 © World Health Organization 2006 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. -
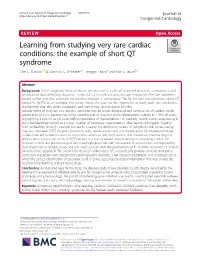
The Example of Short QT Syndrome Jules C
Hancox et al. Journal of Congenital Cardiology (2019) 3:3 Journal of https://doi.org/10.1186/s40949-019-0024-7 Congenital Cardiology REVIEW Open Access Learning from studying very rare cardiac conditions: the example of short QT syndrome Jules C. Hancox1,4* , Dominic G. Whittaker2,3, Henggui Zhang4 and Alan G. Stuart5,6 Abstract Background: Some congenital heart conditions are very rare. In a climate of limited resources, a viewpoint could be advanced that identifying diagnostic criteria for such conditions and, through empiricism, effective treatments should suffice and that extensive mechanistic research is unnecessary. Taking the rare but dangerous short QT syndrome (SQTS) as an example, this article makes the case for the imperative to study such rare conditions, highlighting that this yields substantial and sometimes unanticipated benefits. Genetic forms of SQTS are rare, but the condition may be under-diagnosed and carries a risk of sudden death. Genotyping of SQTS patients has led to identification of clear ion channel/transporter culprits in < 30% of cases, highlighting a role for as yet unidentified modulators of repolarization. For example, recent exome sequencing in SQTS has identified SLC4A3 as a novel modifier of ventricular repolarization. The need to distinguish “healthy” from “unhealthy” short QT intervals has led to a search for additional markers of arrhythmia risk. Some overlap may exist between SQTS, Brugada Syndrome, early repolarization and sinus bradycardia. Genotype-phenotype studies have led to identification of arrhythmia substrates and both realistic and theoretical pharmacological approaches for particular forms of SQTS. In turn this has increased understanding of underlying cardiac ion channels. -
Note to Users
NOTE TO USERS Page(s) not included in the original manuscript and are unavailable from the author or university. The manuscript was microfilmed as received. This reproduction is the best copy available. EFFECT OF COMBINATION POT.-i\SSIL'bI CHANNEL BLOCKERS ON CARDIAC REFEb$.CTORINESS IN ISOLXÎED RABBIT HEARTS AND NTACT GUI'IE.4 PIG HE.4RTS A thssis submitted in conformit>.with the requiremrnts for the degres of hlastrr of Science Graduate Depanment of Medical Science Universit). of Toronto O Copyright by Nikolaos Marnalias 200 1 National Libraiy Bibliothèque nationale du Canada Acquisitions and Acquisitions et Bibliogrâphic Senrices services bibliographiques The author has granted a non- L'auteur a accordé une licence non exclusive licence allowing the exclusive permettant à la National Library of Canada to Bibliothèque nationale du Canada de reproduce, loan, distntbute or sell reproduire, prêter, distribuer ou copies of this thesis in microform, vendre des copies de cette thèse sous paper or electronic formats. la forme de microfiche/film, de reproduction sur papier ou sur format électronique. The author retains ownership of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial extracts from it Ni la thèse ni des extraits substantiels may be printed or otherwise de ceiieîi ne doivent être imprimés reproduced without the author's ou autrement reproduits sans son permission. autorisation. EFFECT OF COMBINATION POTASSIUM CHANNEL BLOCKERS ON CARDIAC REFRACTORiNESS IN ISOLATED RABBIT HEARTS AND iNTACT GUiNEA PIG HEARTS NIKOLAOS MAM.4LIAS MASTER OF SCIENCE 200 1 GRADUATE DEPARTMENT OF MEDICAL SCIENCE LJNIVERSITY OF TORONTO ABSTRACT Dofetilide and sotaiol prolong ventricular refractorinrss by blocking the rapidly açtivating delayrd rectitier potassium channel (Ikr). -

(12) Patent Application Publication (10) Pub. No.: US 2015/0202317 A1 Rau Et Al
US 20150202317A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0202317 A1 Rau et al. (43) Pub. Date: Jul. 23, 2015 (54) DIPEPTDE-BASED PRODRUG LINKERS Publication Classification FOR ALPHATIC AMNE-CONTAINING DRUGS (51) Int. Cl. A647/48 (2006.01) (71) Applicant: Ascendis Pharma A/S, Hellerup (DK) A638/26 (2006.01) A6M5/9 (2006.01) (72) Inventors: Harald Rau, Heidelberg (DE); Torben A 6LX3/553 (2006.01) Le?mann, Neustadt an der Weinstrasse (52) U.S. Cl. (DE) CPC ......... A61K 47/48338 (2013.01); A61 K3I/553 (2013.01); A61 K38/26 (2013.01); A61 K (21) Appl. No.: 14/674,928 47/48215 (2013.01); A61M 5/19 (2013.01) (22) Filed: Mar. 31, 2015 (57) ABSTRACT The present invention relates to a prodrug or a pharmaceuti Related U.S. Application Data cally acceptable salt thereof, comprising a drug linker conju (63) Continuation of application No. 13/574,092, filed on gate D-L, wherein D being a biologically active moiety con Oct. 15, 2012, filed as application No. PCT/EP2011/ taining an aliphatic amine group is conjugated to one or more 050821 on Jan. 21, 2011. polymeric carriers via dipeptide-containing linkers L. Such carrier-linked prodrugs achieve drug releases with therapeu (30) Foreign Application Priority Data tically useful half-lives. The invention also relates to pharma ceutical compositions comprising said prodrugs and their use Jan. 22, 2010 (EP) ................................ 10 151564.1 as medicaments. US 2015/0202317 A1 Jul. 23, 2015 DIPEPTDE-BASED PRODRUG LINKERS 0007 Alternatively, the drugs may be conjugated to a car FOR ALPHATIC AMNE-CONTAINING rier through permanent covalent bonds. -

Frequency-Dependent Electrophysiological Effects of Flecainide, Nifekalant and D,L-Sotalol on the Human Atrium
CLINICAL INVESTIGATIONS Jpn Circ J 2001; 65: 1–6 Frequency-Dependent Electrophysiological Effects of Flecainide, Nifekalant and d,l-Sotalol on the Human Atrium Hiromi Watanabe, MD; Ichiro Watanabe, MD; Toshiko Nakai, MD; Naohiro Oshikawa, MD; Satoshi Kunimoto, MD; Riko Masaki, MD; Toshiaki Kojima, MD; Satoshi Saito, MD; Yukio Ozawa, MD; Katsuo Kanmatuse, MD To compare the effects of class Ic and III antiarrhythmic agents on the termination and prevention of atrial fibril- lation, the present study investigated the use-dependent electrophysiological effects of flecainide, nifekalant and d,l-sotalol on the human atrium. Flecainide significantly prolonged effective refractory period (ERP), intra-atrial conduction time (IACT) and monophasic action potential duration (MAPD), and its effects on ERP and IACT were use-dependent. Nifekalalant significantly prolonged ERP and MAPD, and these effects were reverse use- dependent; however, there was no significant change in IACT. d,l-Sotalol significantly prolonged MAPD and the effect was reverse use-dependent. It significantly prolonged ERP, but the effect was not reverse use-dependent. d,l-Sotalol increased IACT in a use-dependent manner. Thus, for atrial fibrillation, class Ic antiarrhythmic agents might be more effective in termination and class III antiarrhythmic agents might be more effective in prevention. (Jpn Circ J 2001; 65: 1–6) Key Words: Antiarrhythmic drugs; Atrial muscle; Monophasic action potential; Reverse use-dependency; Use-dependency lass I antiarrhythmic drugs have use-dependent diac dysfunction -

Antiarrhythmic Drugs for Out-Of-Hospital Cardiac Arrest with Refractory Ventricular Fibrillation Takashi Tagami1,2*, Hideo Yasunaga2 and Hiroyuki Yokota3
Tagami et al. Critical Care (2017) 21:59 DOI 10.1186/s13054-017-1639-8 REVIEW Open Access Antiarrhythmic drugs for out-of-hospital cardiac arrest with refractory ventricular fibrillation Takashi Tagami1,2*, Hideo Yasunaga2 and Hiroyuki Yokota3 in OHCA patients and that antiarrhythmic drugs can be Abstract used as advanced life support during cardiac arrest in This article is one of ten reviews selected from the patients with refractory ventricular dysrhythmias [5, 6]. Annual Update in Intensive Care and Emergency Refractory VF/pVT is generally defined as failure to ter- medicine 2017. Other selected articles can be found minate VF/pVT with one to three stacked shocks [5]. online at http://ccforum.com/series/ Antiarrhythmic drugs that may be used include amio- annualupdate2017. Further information about the darone, lidocaine, and nifekalant ([5, 6]; Table 1). The Annual Update in Intensive Care and Emergency ILCOR guidelines recommend the use of amiodarone as Medicine is available from http://www.springer.com/ first‐choice treatment for adult patients with refractory series/8901. VF/pVT to improve the rate of return of spontaneous circulation (ROSC) [5, 6]. Lidocaine and nifekalant are recommended as alternatives to amiodarone in the treat- Background ment of refractory VF/pVT in adult patients. However, ‐ ‐ Out of hospital cardiac arrest (OHCA) affects approxi- as mentioned in the knowledge gap section of the latest mately 300,000 people in the United States, 280,000 resuscitation guidelines [5], existing evidence is not people in Europe and 110,000 people in Japan each year enough to suggest that amiodarone is superior to lidocaine – [1 3]. -
Cross-Tumoral Phase 2 Clinical Trial Exploring Crizotinib (PF-02341066) in Patients with Advanced Tumors Induced by Causal Alterations of ALK And/Or MET ("CREATE")
EORTC Avenue E. Mounierlaan 83/11 Brussel 1200 Bruxelles België – Belgique Tel: +32 2 774 16 11 e-mail: [email protected] www.eortc.org EORTC Network of Core Institutions (NOCI) Cross-tumoral phase 2 clinical trial exploring crizotinib (PF-02341066) in patients with advanced tumors induced by causal alterations of ALK and/or MET ("CREATE") EORTC protocol 90101 (EudraCT number 2011-001988-52) (NCT01524926) Study Coordinator: Patrick Schöffski Protocol Date of PRC Amendment reference version approval/notification N° Classification Outline December 03, 2010 ---- ---- 1.0 July 27, 2011 ---- ---- 2.0 February 08, 2012 1 Scientific 3.0 May 15, 2012 2 Scientific 4.0 March 28, 2014 3 Scientific 5.0 June 04, 2014 4 Scientific 6.0 March 26, 2015 5 Scientific 7.0 April 21, 2015 6 Scientific 8.0 August 17, 2015 7 Scientific 9.0 February 25, 2016 8 Scientific 9.1 April 13, 2016 9 Administrative 10.0 February 06, 2017 10 Scientific Version 10.0 / February 06, 2017 Copyright EORTC 2017 EORTC-90101 CREATE Contact addresses Writing Committee: P. Schöffski, University Hospitals Leuven, Leuven, Belgium EORTC Headquarters team, Brussels, Belgium Study Coordinator: Patrick Schöffski Phone: +32 16 346900 E-mail: [email protected] Clinical Research Sandrine Marreaud Physician: Phone: +32 2 774 16 85 E-mail: [email protected] Clinical Scientist: Angélique Deleersnijder Phone: +32 2 774 10 35 E-mail: [email protected] Project Manager: Dominiek Staelens Phone: +32 2 774 15 34 E-mail: [email protected] Data Manager: Tiana -

Stembook 2018.Pdf
The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 WHO/EMP/RHT/TSN/2018.1 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances. Geneva: World Health Organization; 2018 (WHO/EMP/RHT/TSN/2018.1). Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. -

A Abacavir Abacavirum Abakaviiri Abagovomab Abagovomabum
A abacavir abacavirum abakaviiri abagovomab abagovomabum abagovomabi abamectin abamectinum abamektiini abametapir abametapirum abametapiiri abanoquil abanoquilum abanokiili abaperidone abaperidonum abaperidoni abarelix abarelixum abareliksi abatacept abataceptum abatasepti abciximab abciximabum absiksimabi abecarnil abecarnilum abekarniili abediterol abediterolum abediteroli abetimus abetimusum abetimuusi abexinostat abexinostatum abeksinostaatti abicipar pegol abiciparum pegolum abisipaaripegoli abiraterone abirateronum abirateroni abitesartan abitesartanum abitesartaani ablukast ablukastum ablukasti abrilumab abrilumabum abrilumabi abrineurin abrineurinum abrineuriini abunidazol abunidazolum abunidatsoli acadesine acadesinum akadesiini acamprosate acamprosatum akamprosaatti acarbose acarbosum akarboosi acebrochol acebrocholum asebrokoli aceburic acid acidum aceburicum asebuurihappo acebutolol acebutololum asebutololi acecainide acecainidum asekainidi acecarbromal acecarbromalum asekarbromaali aceclidine aceclidinum aseklidiini aceclofenac aceclofenacum aseklofenaakki acedapsone acedapsonum asedapsoni acediasulfone sodium acediasulfonum natricum asediasulfoninatrium acefluranol acefluranolum asefluranoli acefurtiamine acefurtiaminum asefurtiamiini acefylline clofibrol acefyllinum clofibrolum asefylliiniklofibroli acefylline piperazine acefyllinum piperazinum asefylliinipiperatsiini aceglatone aceglatonum aseglatoni aceglutamide aceglutamidum aseglutamidi acemannan acemannanum asemannaani acemetacin acemetacinum asemetasiini aceneuramic