Kirklandside Hospital Update
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Contract Between Scottish Ministers
CONTRACT BETWEEN SCOTTISH MINISTERS AND GEOAMEY PECS LTD FOR THE SCOTTISH COURT CUSTODY AND PRISONER ESCORT SERVICE (SCCPES) REFERENCE: 01500 MARCH 2018 Official No part of this document may be disclosed orally or in writing, including by reproduction, to any third party without the prior written consent of SPS. This document, its associated appendices and any attachments remain the property of SPS and will be returned upon request. 1 | P a g e 01500 Scottish Court Custody and Prisoner Escort Service (SCCPES) FORM OF CONTRACT CONTRACT No. 01500 This Contract is entered in to between: The Scottish Ministers, referred to in the Scotland Act 1998, represented by the Scottish Prison Service at the: Scottish Prison Service Calton House 5 Redheughs Rigg Edinburgh EH12 9HW (hereinafter called the “Purchaser”) OF THE FIRST PART And GEOAmey PECS Ltd (07556404) The Sherard Building, Edmund Halley Road Oxford OX4 4DQ (hereinafter called the “Service Provider”) OF THE SECOND PART The Purchaser hereby appoints the Service Provider and the Service Provider hereby agrees to provide for the Purchaser, the Services (as hereinafter defined) on the Conditions of Contract set out in this Contract. The Purchaser agrees to pay to the Service Provider the relevant sums specified in Schedule C and due in terms of the Contract, in consideration of the due and proper performance by the Service Provider of its obligations under the Contract. The Service Provider agrees to look only to the Purchaser for the due performance of the Contract and the Purchaser will be entitled to enforce this Contract on behalf of the Scottish Ministers. -
HSCP-Annual Performance Report
East Ayrshire Health and Social Care Partnership Annual Performance Report 2017/18 September 2018 1 Table of Contents 1. Executive Summary ...................................................................................................................................................... 3 2. Introduction ................................................................................................................................................................. 8 3A. Measuring Performance Under Integration ............................................................................................................. 12 3. Our Performance 2015/16-2017/18 ........................................................................................................................... 13 4. Integration Joint Board- Governance and Decision Making ....................................................................................... 38 5. Financial Performance ............................................................................................................................................... 46 6. Best Value................................................................................................................................................................... 54 7. Inspection Findings..................................................................................................................................................... 55 8. Audit and Performance Committee .......................................................................................................................... -

W-Ward 5, Woodland View
Woodland View Ward 5 Woodland View Information for you Recovery that benefits individuals, families, carers and communities Ward 5 is a residential unit, which provides a specialist service for residents of Ayrshire and Arran over the age of 16, who have an alcohol and/or drug problem and mental health issues. The ward has 10 beds for residential care; 5 for rehabilitation and 5 for detoxification with 8 day care places available. It is situated within the grounds of Woodland View, Ayrshire Central Hospital. Ward 5 provides a flexible service based on the needs of each individual person. The main treatment is through 1 to 1 support and group work, with each workshop designed to support each person on their road to recovery. Treatments available consist of: • A detoxification programme (usually up to 1 week) • A residential 4 week programme • Assessment of mental health and wellbeing • A structured day attendance programme Who does Ward 5 work with? We work with a wide range of partner organisations (including third and voluntary sector organisations) to support an individual’s recovery. We will also link clients in with peer support groups and activities. 2 Committed to the protection of children and vulnerable adults Recovery that benefits individuals, families, carers and communities How can Ward 5 help you? Alcohol and drug misuse can affect your physical and mental health, your relationships, your employment as well as your ability to cope with everyday life. Factors such as age, family support, lifestyle, personality and personal belief may also determine how drugs or alcohol affect you. Recovery means different things to different people and no two people will have the same recovery journey. -

Report Contents
East Ayrshire Advocacy Services Ltd Annual Report April 2017– March 2018 REPORT CONTENTS 1. Report Contents 2. Chairperson’s Report 3. Manager’s Report 4. Who’s Who! 5. What do we mean by advocacy? Why do we need it? 6. Why Should Advocacy be Independent? 7. Types of Advocacy provided 8-9. Who is our Service for? How to refer 10-16. Referral Information – Adult Service 17-19. Referral information – Older people’s Service and Specialist Service 20-21. Independent Advocacy – HMP Kilmarnock (Bowhouse) 22. Advocacy Matters 23-24. Awareness Raising/Networking 25. Inputs to Consultation Exercises/Strategy Groups etc. 26. Training 27. Resource Information 28. Thanks 29-30. Board of Directors Report for year ended 31st March 2018 1 Board of Directors 2017-2018 Independent Examination of Accounts 2 East Ayrshire Advocacy Services Ltd Annual Report April 2017 – March 2018 CHAIRPERSON’S REPORT This past year has been a year of uncertainty for the Board of Directors and staff as our service was reviewed (see Manager’s Report). However, despite this, our dedicated staff continued to cope with the ever increasing demand for independent advocacy in East Ayrshire. Workloads continue to increase and staff constantly juggle their time to ensure that those most vulnerable in our community are enabled to make their views known. We are very grateful to our funders East Ayrshire Council and NHS Ayrshire and Arran for their continued commitment to independent advocacy, particularly in these times of budget constraints and efficiencies. Also, many thanks to each and every member of staff and my fellow Board members for all their hard work and commitment. -

NHS Ayrshire and Arran Annual Audit 2015/16
NHS Ayrshire and Arran 2015/16 Annual Audit Report for the Board of NHS Ayrshire and Arran and the Auditor General for Scotland June 2016 Key contacts Contents Fiona Mitchell-Knight, Assistant Director Key messages .................................................................................................. 3 [email protected] Introduction ...................................................................................................... 5 Audit of the 2015/16 financial statements....................................................... 6 David Jamieson, Senior Audit Manager [email protected] Financial management and sustainability .................................................... 13 Governance and transparency ...................................................................... 21 Mark Laird, Senior Auditor Best Value ....................................................................................................... 29 [email protected] Appendix I: Significant audit risks ............................................................... 34 4th Floor (South Suite) Appendix II: Summary of NHS Ayrshire and Arran local audit reports 2015/16 ......................................................................................................................... 40 The Athenaeum Building 8 Nelson Mandela Place Appendix III: Summary of Audit Scotland national reports 2015/16 .......... 41 Glasgow Appendix IV: Action plan ............................................................................. -
Audit and Scrutiny Committee 14 November 2017
Audit and Scrutiny Committee A Meeting of the Audit and Scrutiny Committee of North Ayrshire Council will be held in the Council Chambers , Ground Floor, Cunninghame House, Irvine, KA12 8EE on Tuesday, 30 January 2018 at 10:00 to consider the undernoted business. 1 Declarations of Interest Members are requested to give notice of any declarations of interest in respect of items of business on the Agenda. 2 Minutes The accuracy of the Minutes of the meetings of the Audit and Scrutiny Committee held on 14 November 2017 and 9 January 2018 will be confirmed and the Minutes signed in accordance with Paragraph 7 (1) of Schedule 7 of the Local Government (Scotland) Act 1973 (copy enclosed). 3 Quarter Two 2017/18 Progress Report - Directorate Plan Performance Submit report by the Chief Executive on the progress of the Directorate Plans 2015/18 as at 30 September 2017 (copy enclosed). 4 Local Government Benchmarking Framework (LGBF) 2015/16 Submit report by the Chief Executive on the Directorates' priorities identified following the publication of the latest LGBF report (copy enclosed). 5 Internal Audit Repor ts Issued Submit report by the Executive Director (Finance and Corporate Support) on the findings of Internal Audit work completed between 1 November and 31 December 2017 (copy enclosed). 6 Internal Audit Charter Submit report by Executive Director (Finance and Corporate Support) on the updated Internal Audit Charter (copy enclosed). North Ayrshire Council, Cunninghame House, Irvine KA12 8EE 1 7 Q2 2017 YTD Complaint Report Submit report by the Executive Director (Finance and Corporate Support) on the Council's complaint performance and the volumes and trends of complaints received in the first 6 months of Financial Year 2017/18. -

Integration Joint Board Meeting Thursday, 11 February 2021 at 10
Integration Joint Board Meeting Thursday, 11 February 2021 at 10:00 Arrangements in Terms of COVID-19 In light of the current COVID-19 pandemic, this meeting will be held remotely in accordance with the provisions of the Local Government (Scotland) Act 2003. Where possible, the meeting will be live-streamed and available to view at https://north-ayrshire.public-i.tv/core/portal/home. In the event that live-streaming is not possible, a recording of the meeting will instead be available to view at this location. 1 Apologies 2 Declarations of Interest Members are requested to give notice of any declarations of interest in respect of items of business on the Agenda. 3 Minutes/Action Note The accuracy of the Minutes of the meeting held on 17 December 2020 will be confirmed and the Minutes signed in accordance with Paragraph 7 (1) of Schedule 7 of the Local Government (Scotland) Act 1973. 3.1 Matters Arising Consider any matters arising from the minutes of the previous meeting. 4 Appointments and Recruitment Submit report by Andrew Fraser, Head of Service (Democratic Services) on the appointment of the Director of North Ayrshire Health and Social Care Partnership and the Head of Service (Health and Community Care) and arrangements for the appointment of the Chief Finance and Transformation Officer and Section 95 Officer (copy enclosed). 1 5 Director’s Report Submit report by Caroline Cameron, Director NAHSCP on developments within the North Ayrshire Health and Social Care Partnership (copy enclosed). 6 Financial Performance Submit report by Eleanor Currie, Interim Chief Finance and Transformation Officer on the financial position of the North Ayrshire Health and Social Care Partnership (copy enclosed). -
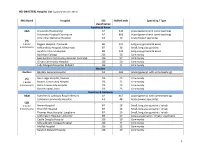
MASTER) Hospital List (Updated October 2015
HEI (MASTER) Hospital List (updated October 2015) NHS Board Hospital ISD Staffed beds Speciality / Type classification Ayrshire & Arran A&A University Hospital Ayr A2 343 Acute (general with some teaching) University Hospital Crosshouse A2 666 Acute (general with some teaching) Arran War Memorial Hospital A3 19 Acute (mixed speciality) (9) 3 acute Biggart Hospital, Prestwick B6 121 Long stay geriatric & acute 6 community Kirklandside Hospital, Kilmarnock B7 36 Small, long stay geriatric Ayrshire Central Hospital B8 142 Long stay geriatric & acute Davidson Cottage J26 26 Community East Ayrshire Community Hospital, Cumnock J26 57 Community Girvan Community Hospital J26 20 Community Lady Margaret Hospital, Millport J26 9 Community Borders Borders Borders General Hospital A2 265 Acute (general, with some teaching) (5) Hay Lodge Hospital, Peebles J26 23 Community 1 acute Hawick Community Hospital J26 22 Community 4 community Kelso Community Hospital J26 23 Community Knoll Hospital, Duns J26 23 Community Dumfries & Galloway D&G Dumfries & Galloway Royal Infirmary A2 367 Acute (general, with some teaching) Galloway Community Hospital A3 48 Acute (mixed speciality) (10) 2 acute Annan Hospital B7 18 Small, long stay geriatric / rehab 8 community Thornhill Hospital B7 13 Small, long stay geriatric / rehab Thomas Hope Hospital, Langholm B7 10 Small, long stay geriatric / rehab Lochmaben Hospital, Lockerbie B9 17 Long stay geriatric / rehab / psychiatry Castle Douglas Hospital J26 19 Community Kirkcudbright Cottage Hospital J26 9 Community Moffat Hospital J26 12 Community Newton Stewart Hospital J26 19 Community 1 HEI (MASTER) Hospital List (updated October 2015) Fife Fife Victoria Hospital, Kirkcaldy A2 621 Acute (general with some teaching) (7) Queen Margaret Hospital, Dunfermline A3 196 Acute (mixed speciality) 2 acute 5 community Cameron Hospital, Leven B7 95 Small, long stay geriatric Adamson Hospital, Cupar J26 19 Community Glenrothes Hospital J26 74 Community Randolph Wemyss Memorial Hospital J26 16 Community St. -

Site Code Site Name Address Address2 Town Post Code Tenure
Site Code Site Name Address Address2 Town Post Code Tenure Organisation A210H Ayr Hospital Dalmellington Road Ayr KA7 3UB Owned NHS Ayrshire & Arran A103H Ayrshire Central Hospital Ayrshire Central Hospital Kilwinning Road Irvine KA12 8TJ Owned NHS Ayrshire & Arran A111H Crosshouse Hospital 59A Kilmarnock Road Crosshouse Kilmarnock KA2 0BD Owned NHS Ayrshire & Arran A211B Drongan Resource Centre 21A Mill Of Shield Road Drongan KA6 7BA Owned NHS Ayrshire & Arran A204B Girvan Health Centre 109A Henrietta Street Girvan KA26 9AN Owned NHS Ayrshire & Arran A206H Holmhead Hospital Holmhead Cumnock KA18 1RR Owned NHS Ayrshire & Arran A110H Lady Margaret Hospital College Street Millport KA28 0HF Owned NHS Ayrshire & Arran A218C Muirkirk Clinic Glasgow Road Muirkirk KA18 3RQ Owned NHS Ayrshire & Arran A278B Patna Health Centre Doonside Avenue Patna KA6 7LX Owned NHS Ayrshire & Arran A201H Ailsa Hospital Dalmellington Road Ayr KA6 6AB Owned NHS Ayrshire & Arran A024B Dailly Surgery Owned NHS Ayrshire & Arran A026B Lochranza Newton Road Lochranza KA27 8HQ Owned NHS Ayrshire & Arran A101H Arran War Memorial Margnaheglish Road Lamlash KA27 8LF Owned NHS Ayrshire & Arran A104B Stewarton Health Centre 46 High Street Stewarton KA3 5BP Owned NHS Ayrshire & Arran A105B Townhead Surgery, Irvine Owned NHS Ayrshire & Arran A105H Kirklandside Hospital Kirklandside Kilmarnock KA1 5LH Owned NHS Ayrshire & Arran A106B Stevenston Health Centre Main Street Stevenston KA20 3AB Owned NHS Ayrshire & Arran A107B Saltcoats Health Centre 19 Raise Street Saltcoats KA21 -

Property and Asset Management Strategy (PAMS)
2015/16 Property and Asset Management Strategy (PAMS) Image 1 - Artist Impression of NACH Scheme (Source: Balfour Beatty) Working together to NHS Ayrshire & Arran achieve the healthiest life possible for everyone in DRAFT 9 Ayrshire and Arran 17/06/2015 Property and Asset Management Strategy (PAMS) Contents Contents .............................................................................................................................. 2 1. Executive Summary ....................................................................................... 5 2. Introduction .................................................................................................... 7 3. Where are we now? ...................................................................................... 10 3.1. NHS Ayrshire and Arran ................................................................................................. 10 3.1.1. Health and Social Care Partnerships .............................................................................. 11 3.2. Current Developments................................................................................................... 13 3.2.1. Building for Better Care ................................................................................................. 13 3.2.2. Woodland View (Formerly Adult Acute Mental Health Community Hospital, NACH) .. 15 3.2.3. Focus for Investment – Property ................................................................................... 18 3.2.4. Disinvestment and Sales ............................................................................................... -

Mental Health Services and Woodland View
EAST AYRSHIRE HEALTH AND SOCIAL CARE PARTNERSHIP INTEGRATED JOINT BOARD 4 FEBRUARY 2016 WOODLAND VIEW PROGRESS REPORT Report by the Director of Health and Social Care INTRODUCTION 1. Due for completion on 18 March 2016, Woodland View is the new mental health and community hospital facility at Ayrshire Central Hospital, Irvine. The new development will have 206 single occupancy bedrooms each with ensuite shower rooms and a full range of therapeutic support accommodation within 11 single storey wards each with private courtyard gardens and a range of community and treatment services including outpatients over 2 floors. 2. The design of the new development provides the best possible healing environment for patients and a safe and inspiring working environment for staff. It is based on a holistic view of wellbeing and addresses the psychological, emotional, physical and physiological needs of both patients and staff creating a therapeutic environment. 3. The flexible accommodation is designed to easily adapt to new models of care which focus on the recovery, rehabilitation and enablement of individuals from North, East and South Ayrshire and to provide a hub of community resource to be flexibly used by other agencies, partners and the public. In – patient Services are: Speciality Bed Numbers Area Served Adult Acute Mental Health 3 wards each with North, East , South 20 beds = 60 Adult Mental Health 2x10 beds = 20 North, East, South Rehabilitation bedded unit Adult Mental Health 1x10 beds =10 North, East , South Forensic rehabilitation Adult Addiction 1x10 beds = 10 North, East, South Rehabilitation Adult Low Secure Service 1x 8 beds = 8 North, East, South Intensive Psychiatric Care 1x8 beds = 8 North, East, South Unit Elderly Mental Health Acute 1x15 beds = 15 North, East Organic Elderly Mental Health Acute 1x15 beds = 15 North, East -Functional Older People Rehabilitation 1x30 beds = 30 North and Enablement Older People Complex Care 1x30 beds = 30 North Total 206 beds WOODLAND VIEW PROGRAMME PLAN 4. -

Scotland) 15 June 2021
Version 1.6 (Scotland) 15 June 2021 ISARIC/WHO Clinical Characterisation Protocol UK (Scotland) Recruitment Procedures for FRONTLINE CLINICAL RESEARCH STAFF The most up to date versions of the protocol and case report form are available at isaric4c.net/protocols/ A virtual site visit is available at isaric4c.net/virtual_site_visit/ AIM: Please recruit the following patients only: • Vaccine failure (positive COVID test - rather than displaying symptoms – >28d after having received a vaccine) • Reinfection (proven after proven) • Co-infection (flu/RSV) • COVID associated hyper inflammation (MIS-A/MIS-C/PINS-TS) at any age • Samples from patients with pathogens of public health interest including people identified as infected with SARS-CoV “variants of concern” • All children CONSENT: once the form is signed by a participant it is hazardous. To record consent, we suggest an independent witness observes the completed form then signs a fresh copy outside of the isolation area. Consent can also be obtained by telephone from participants or from relatives for proxy consent. RECRUITMENT PACKS: Sample collection kits will be supplied to sites. Sample collections kits can be requested from: [email protected] Each kit will have a specific kit ID number, with each component within showing this kit ID and its own respective component ID for audit purposes. Pods and bio-bags for shipping will also be supplied to sites. These can be requested from [email protected] OBTAIN SAMPLES according to the schedule. You can find out which tier you are operating at in the front page of the site file. If you have capacity to recruit at TIER 2: Day 1 2 3 4 5 6 7 8 9 28 days after discharge Samples R S S C Sample priority 1 2 3 4 R: recruitment sample; S: serial sample; C: convalescent sample.