Hydrogels for Wound Dressings a Thesis Su
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MAKIMOUSSE COMPOSITION INCI Name SODIUM POLYACRYLATE STARCH
MAKIMOUSSE COMPOSITION INCI Name SODIUM POLYACRYLATE STARCH TEXTURING AGENT TEXTURING AGENT TEXTURING AGENT SELF-REGULATING SELF-REGULATING SELF-REGULATING RHEOLOGICAL RHEOLOGICAL RHEOLOGICAL AGENT AGENT AGENT SMOOTH SILKY BULKY SILKY SILKY MOUSSE = NON MOUSSE = NON NON MAKIMOUSSE CHOCOLATE MAKIMOUSSE CHANTILLY MAKIMOUSSE FASTER STICKY 25 STICKY STICKY 12 MOUSSE 7 SWELLING AFTERFEEL MOUSSE AFTERFEEL AFTERFEEL TYPE TYPE MATTE SMOOTH SMOOTH FROSTED FROSTED GLOSSY GEL GEL WAVE TYPE GEL swelled hand mixer swelled hand mixer swelled hand mixer 1% gels were prepared by different methods (swelling, by hand, with a mixer): Low shear achieves frosted aspect, high shear reduces frosted aspect with immediate ultimate volume Influence of shear on the gel formation: aspect and spreadability 0,5% gels were poured into a mould. The aspect was observed 5 minutes after demoulding: swelled hand mixer swelled hand mixer swelled hand mixer Particle size 100µm 100µm 100µm Mean particle size = 25 µm Mean particle size = 12 µm Mean particle size = 7 µm Formulation Gel formation MAKIMOUSSE CONVENTIONAL • Swells in water witout agitation or by manual or THICKENER mechanical stirring • pH: stable over a pH range of 4 to 10 • Alcohols: compatible up to 40% with ethanol • Salts: swelling capacity decreases in presence of salts. A higher polymer concentration is required to reach the same Water viscosity compared to a salt-free medium. Water • Urea: compatible • Surfactants: compatible with anionics and nonionics but only up to 1% with cationic, (higher polymer concentration -

Biocompatible Non-Covalent Complexes of Chitosan and Different Polymers: Characteristics and Application in Drug Delivery
Arh. farm. 2020; 70: 173 – 197 Review article/Pregledni rad Biocompatible non-covalent complexes of chitosan and different polymers: characteristics and application in drug delivery Ana Ćirić1*, Danina Krajišnik1, Bojan Čalija1, Ljiljana Đekić1 1 University of Belgrade - Faculty of Pharmacy, Department of Pharmaceutical Technology and Cosmetology, Vojvode Stepe 450, 11221 Belgrade, Serbia *Corresponding author: Ana Ćirić, E-mail: [email protected] Abstract The formulation of biocompatible drug carriers based on cationic biopolymer chitosan and natural or synthetic polymers represents an important research interest. Therefore, this review aims to perceive their potential in drug delivery. The most investigated chitosan-based polymer blends are polyelectrolyte complexes (PECs) obtained by establishing ionic interactions with biocompatible polyanions as alginates, pectin, xanthan gum, carrageenan, carboxymethylcellulose, and collagen. Depending on the preparation conditions, PECs could be prepared in versatile forms including membranes/films, hydrogel beads, nanoparticles, and microparticles, to achieve controlled (e.g., extended, delayed, colon-specific and pH-dependent) drug delivery. PECs can encapsulate hydrophilic and lipophilic drug substances with different molecular weights. Drug encapsulation allows the preservation of their structure, activity, improvement in absorption efficiency, reduction in adverse effects and long-term stability in vitro and in vivo. The biocompatible structures as non-covalent chitosan-based complexes could be formed also by establishing hydrogen bonds, for example with poly(vinyl alcohol). The swelling of these complexes is not pH-dependent and encapsulated drug substances are often released by already known types of diffusion. Moreover, grafted chitosan derivatives (e.g., carboxymethyl chitosan, trimethyl chitosan, acrylated chitosan) are synthesized to improve water solubility at a wide pH range and enhance the encapsulation capacity of promising PEC-based drug carriers. -

Effects of Sodium Polyacrylate and Potassium Polymer on Growth and Physiological Characteristics of Different Flue-Cured Tobaccos W.X
Bulgarian Chemical Communications, Volume 50, Issue 2, (pp. 315 –323) 2018 Effects of sodium polyacrylate and potassium polymer on growth and physiological characteristics of different flue-cured tobaccos W.X. Huang*, Z.Z. Wei, G.Y. Niu, Y.J Zhang, H.F. Shao* College of Tobacco Science, Henan Agricultural University, Zhengzhou, Henan, 450002, China Received January 14, 2018; Accepted February 7, 2018 To investigate water retention effects and physiological regulation mechanism of water-retaining agents on the growth and development of different flue-cured tobacco varieties, a pot experiment was conducted using ‘Yuyan 6’ and ‘Yuyan 10’ to study the effects of sodium polyacrylate and potassium polymer on the agronomic characteristics, the root activity, the activity of antioxidant enzymes, the content of malondialdehyde (MDA) and proline in the leaves of flue-cured tobaccos. The results were as follows. (1) The application of water-retaining agents increased the plant height, the stem diameter, the number of effective leaves, the maximum leaf area and the root activity of flue-cured tobaccos and the effects were more significant for Yuyan 10 of relatively poor drought resistance. (2) The activity of SOD, POD and CAT of flue-cured tobaccos treated with water-retaining agents was reduced to different extents. (3) The application of water-retaining agents lowered the MDA content of flue-cured tobaccos but the effects were more significant for Yuyan 10 of relatively poor drought resistance. (4) The application of water-retaining agents decreased the proline content of flue-cured tobaccos under drought conditions, but the decrease of proline content in Yuyan 6 was larger than that in Yuyan 10. -
Superabsorbent Polymers
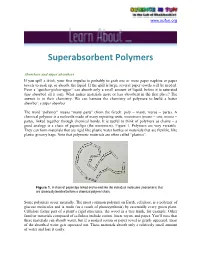
www.scifun.org Superabsorbent Polymers Absorbers and super absorbers If you spill a drink, your first impulse is probably to grab one or more paper napkins or paper towels to soak up, or absorb, the liquid. If the spill is large, several paper towels will be needed. Even a “quicker-picker-upper” can absorb only a small amount of liquid, before it is saturated (has absorbed all it can). What makes materials more or less absorbent in the first place? The answer is in their chemistry. We can harness the chemistry of polymers to build a better absorber: a super absorber. The word “polymer” means “many parts” (from the Greek: poly = many, meros = parts). A chemical polymer is a molecule made of many repeating units, monomers (mono = one, meros = parts), linked together through chemical bonds. It is useful to think of polymers as chains – a good analogy is a chain of paperclips (the monomers), Figure 1. Polymers are very versatile. They can form materials that are rigid like plastic water bottles or materials that are flexible, like plastic grocery bags. Note that polymeric materials are often called “plastics”. Figure 1. A chain of paperclips linked end-to-end like the individual molecules (monomers) that are chemically bonded to form a chemical polymer chain. Some polymers occur naturally. The most common polymer on Earth, cellulose, is a polymer of glucose molecules and is made (as a result of photosynthesis) by essentially every green plant. Cellulose forms part of a plant’s rigid structures, the wood in a tree trunk, for example. -

Life Cycle Assessment of Bio-Based Sodium Polyacrylate Production from Pulp Mill Side Streams: Case Study of Thermo-Mechanical and Sulfite Pulp Mills
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Chalmers Publication Library Life cycle assessment of bio-based sodium polyacrylate production from pulp mill side streams: Case study of thermo-mechanical and sulfite pulp mills Paul Gontiaa, Matty Janssena,∗ aEnvironmental Systems Analysis, Department of Energy and Environment, Chalmers University of Technology, SE-412 96 Goteborg,¨ Sweden Abstract Sodium polyacrylate (Na-PA) is a super absorbent polymer, which is commonly used in diverse hygiene products. The polymer is currently produced from fossil feedstock and its production consequently leads to adverse environmental impacts. Na-PA production from sugars present in pulp mill side streams can potentially be a successful way to achieve a more sustainable production of this polymer. In order to guide the development of a novel biochemical process for producing Na-PA, a life cycle assessment was done in which Na-PA produced from side streams of thermo-mechanical pulp (TMP) and sulfite pulp mills were compared. Furthermore, a comparison was made with Na-PA produced from fossil resources. The results show that the main determinant of the environmental impact of the bio-based Na-PA production is the free sugar content in the side streams. The lowest environmental impact is achieved by the least diluted side streams. More diluted side streams require larger amounts of energy for concentration, and, if the diluted streams are not concentrated, processes such as hydrolysis and detoxification, and fermentation are the environmental hotspots. Furthermore, the higher the yield of the fermentation process, the lower the environmental impact will be. -

Sodium Polyacrylate Superabsorbent Polymers SCIENTIFIC
Sodium Polyacrylate Superabsorbent Polymers SCIENTIFIC Introduction Water from one cup is poured into an “empty” cup (actually containing sodium polyacrylate) and the water “disappears!” Concepts • Polymers • Osmosis • Superabsorbents • Industrial chemistry Materials Sodium polyacrylate, 0.5 g Styrofoam® cups or other opaque containers, 2 Distilled or deionized water, 100 mL Safety Precautions Sodium polyacrylate is nontoxic. However, it is irritating to the eyes and also to nasal membranes if inhaled. Wear chemical splash goggles whenever working with chemicals, heat or glassware. Sodium polyacrylate is an obvious choice for student pranks. Be careful students do not have access to sodium polyacrylate outside of chemistry class. Please review current Material Safety Data Sheets for additional safety, handling, and disposal information. Pre-Lab Preparation Before the students come into the room, place 0.5 g of sodium polyacrylate in one of the Styrofoam cups. Procedure 1. Add approximately 100 mL of distilled or deionized water to the second Styrofoam cup. 2. Tell the students that the water will “disappear” when poured into the other cup. (You can tip the cup forward some- what to show that it is “empty”; it will be difficult to see the 0.5 g of sodium polyacrylate against the white Styrofoam cup.) 3. Slowly pour the water into the cup containing sodium polyacrylate. Swirl the cup a bit (give the sodium polyacrylate time to absorb the water). 4. Tip the cup downward slightly to show the students that the water has “disappeared”! (Don’t turn the cup upside down, or you may dump the jelly-like mass on the floor!) Disposal Please consult your current Flinn Scientific Catalog/Reference Manual for general guidelines and specific procedures, and review all federal, state and local regulations that may apply, before proceeding. -

Safety Data Sheet the Dow Chemical Company
SAFETY DATA SHEET THE DOW CHEMICAL COMPANY Product name: ACULYN™ 2051 Rheology Modifier Issue Date: 03/11/2021 Print Date: 03/25/2021 THE DOW CHEMICAL COMPANY encourages and expects you to read and understand the entire (M)SDS, as there is important information throughout the document. We expect you to follow the precautions identified in this document unless your use conditions would necessitate other appropriate methods or actions. 1. IDENTIFICATION Product name: ACULYN™ 2051 Rheology Modifier Recommended use of the chemical and restrictions on use Identified uses: Rheology modifier COMPANY IDENTIFICATION THE DOW CHEMICAL COMPANY 2211 H.H. DOW WAY MIDLAND MI 48674 UNITED STATES Customer Information Number: 800-258-2436 [email protected] EMERGENCY TELEPHONE NUMBER 24-Hour Emergency Contact: CHEMTREC +1 800-424-9300 Local Emergency Contact: 800-424-9300 2. HAZARDS IDENTIFICATION Hazard classification GHS classification in accordance with the OSHA Hazard Communication Standard (29 CFR 1910.1200) Not a hazardous substance or mixture. Other hazards No data available 3. COMPOSITION/INFORMATION ON INGREDIENTS Chemical nature: Organic compound emulsion This product is a mixture. Component CASRN Concentration ® ™ Trademark of The Dow Chemical Company ("Dow") or an affiliated Page 1 of 15 company of Dow Product name: ACULYN™ 2051 Rheology Modifier Issue Date: 03/11/2021 Sodium polyacrylate 9003-04-7 >= 20.0 - <= 29.0 % Decamethylcyclopentasiloxane 541-02-6 >= 7.0 - <= 10.0 % Ethoxylated branched C11-14, C13-rich 78330-21-9 >= 3.0 - <= 4.0 % alcohols 4. FIRST AID MEASURES Description of first aid measures General advice: If potential for exposure exists refer to Section 8 for specific personal protective equipment. -

ACUMER™ 1051 Scale Inhibitor for Sugar Process
Technical Data Sheet ACUMER™ 1051 Scale Inhibitor for Sugar Process Description ACUMER™ 1051 is a low molecular weight (LMW) polyacrylic acid polymer that can be used as a scale inhibitor during sugar processing. The product has U.S. Food and Drug Administration (FDA) clearance for food contact use. Features and • High performance scale inhibition that can be used in sugar evaporators. Benefits • Wide range of activity on calcium oxalate, calcium sulfate and calcium carbonate scales. • FDA cleared under regulation 21 CFR 173.73 (sodium polyacrylate). • Intrinsically Kosher (manufactured with no raw materials of animal origin). • Shows a higher degree of solubility in presence of calcium ions than other higher molecular weight polymers. Typical Physical (These properties are typical but do not constitute specifications). Properties Property Typical Values Molecular Weight (average) 2000-2300 pH (fully neutralized) 7 Solids, % 43 Density @ 25°C, lb/gal (g/cc) 10.3 (1.22) Brookfield Viscosity, 200 mPa.s/cps @ 25°C (#2 @ 30 rpm) Color, APHA 100 Appearance colorless to straw colored, clear to slightly hazy homogeneous solution, FFVFM* *free from visible foreign matter Anti-Precipitation ACUMER™ 1051 polymer is a general purpose scale inhibitor, as it is effective to inhibit Performance precipitation of calcium carbonate, calcium oxalate, calcium sulphate, barium sulphate, and other low solubility salts. Sugar Processing Heavy scaling occurs all along the evaporation line where the thin juice must be Application concentrated before crystallization. Without any treatment, scaling is responsible for progressively dropping the production capacity and increasing the manufacturing costs and the demand of energy. At the final stage the sugar mill must be shut down for cleaning. -

Red List Microplastic Ingredients
Products on this list have been found to contain ingredients which are commonly considered to be microplastic ingredients. These include but are not limited to Polyethylene (PE), Polypropylene (PP), Polymethyl methacrylate (PMMA), Nylon (PA), Polyurethane, and Acrylates Copolymer. No. Polymer Source 1 Acetophenone/Oxymethylene Copolymer ECHA 2 Acetylenediurea/Formaldehyde/Tosylamide Crosspolymer ECHA 3 Acrolein/Acrylic Acid Copolymer ECHA 4 Acrylamide/Ammonium Acrylate Copolymer ECHA 5 Acrylamide/Ethalkonium Chloride Acrylate Copolymer ECHA 6 Acrylamide/Ethyltrimonium Chloride Acrylate/Ethalkonium Chloride ECHA Acrylate Copolymer 7 Acrylamide/Sodium Acrylate Copolymer ECHA 8 Acrylamide/Sodium Acryloyldimethyltaurate Copolymer ECHA 9 Acrylamide/Sodium Acryloyldimethyltaurate/Acrylic Acid Copolymer ECHA 10 Acrylamides/DMAPA Acrylates/Methoxy PEG Methacrylate Copolymer ECHA 11 Acrylamidopropyltrimonium Chloride/Acrylates Copolymer ECHA 12 Acrylates Copolymer ECHA; UNEP; 13 Acrylates Crosspolymer ECHA 14 Acrylates Crosspolymer-3 ECHA 15 Acrylates Crosspolymer-4 ECHA 16 Acrylates/Acetoacetoxyethyl Methacrylate Copolymer ECHA 17 Acrylates/Acrylamide Copolymer ECHA 18 Acrylates/Aminoacrylates/C10-30 Alkyl PEG-20 Itaconate Copolymer ECHA 19 Acrylates/Ammonium Methacrylate Copolymer ECHA 20 Acrylates/Beheneth-25 Methacrylate Copolymer ECHA 21 Acrylates/Beheneth-25 Methacrylate/Steareth-30 Methacrylate ECHA Copolymer 22 Acrylates/Behenyl Acrylate/Dimethicone Methacrylate Copolymer ECHA 23 Acrylates/Behenyl Methacrylate/Dimethicone Methacrylate -

Carbosperse K-7058N Sodium Polyacrylate Is Also Available in a Powder Form Known As Carbosperse K-7058D
TECHNICAL DATA SHEET Carbosperse™ K-7058N Sodium Polyacrylate Carbosperse K-7058N polyacrylate is a sodium salt of a low molecular weight water soluble acrylic acid polymer (i.e., Carbosperse K-7058) supplied as a water white to amber, slightly hazy, 45% total solids solution in water. Carbosperse K-7058N polyacrylate is a high performance polyelectrolyte with multi-functional properties including sequestration, dispersion, scale inhibition, crystal growth distortion, binding, and plasticizing. The typical properties for Carbosperse K-7058N polyacrylate are as follows: Form Water solution Appearance Water white to amber, slightly hazy Total solids (%) 45 (44 to 46)* Active solids (%) 35.7 Molecular weight** (GPC MW) 7,300 pH 7.0 (6.5 to 7.5)* Viscosity (cP at 25°C) 675 (500 to 750)* Specific gravity 1.2 (1.1 to 1.3) * Specification. ** Expressed as polyacrylic acid as determined an aqueous GPC method. Carbosperse K-7058N sodium polyacrylate is also available in a powder form known as Carbosperse K-7058D. CBSK7058N-TDS (Jun-07) ™ Trademark of The Lubrizol Corporation Lubrizol Advanced Materials, Inc. The information contained herein is believed to be reliable, but no representations, guarantees or warranties of any kind are made as to its accuracy, suitability for particular applications or the results to be obtained. The information is based on laboratory work with small-scale equipment and does not necessarily indicate end 9911 Brecksville Road product performance. Because of the variations in methods, conditions and equipment used commercially in processing these materials, no warranties or guarantees Cleveland, OH 44141-3247 are made as to the suitability of the products for the applications disclosed. -

Lab 2: How Do Diapers Work?
Chemistry 108, Spring 2017 Lab 2: How Do Diapers Work? Goal: In this lab you will compare a generic disposable diaper with a name brand disposable diaper. You will experiment with the chemical responsible for absorbing the water (sodium polyacrylate) and you will decide which type of diaper is the better deal. Report: You have been hired as a free-lance author to write an article for Parent’s magazine. Write an article comparing the generic diaper with the name brand diaper. Discuss the tests you ran, what you found out, and give your opinion on the better of the two diapers (and how you arrive at this conclusion). Also include a discussion of sodium polyacrylate and how it works. Explain how salt affects the performance of sodium polyacrylate and how this relates to urine. Think about and describe at least two other uses for sodium polyacrylate besides its use in disposable diapers. The article should be informative, written for the layperson, scientifically accurate, and incorporate all of your observations, data, and calculations in an organized manner. Procedure: Part One: Making the Synthetic Urine 1. Place 1000 mL (1 L) of deionized water in a large flask. 2. Add 24.3 g of urea to the water and stir until dissolved. 3. Add 10.0 g sodium chloride (NaCl), 6.0 g potassium chloride (KCl), and 6.3 g sodium dihydrogen phosphate (NaH2PO4) to this solution and stir until dissolved. 4. Add a few drops of yellow food coloring to the solution (for affect). Part Two: Comparing the Engineering of the Diapers 1. -

Super Absorbent Polymer – Sodium Polyacrylate
NCSU – Dept. of Chemistry – Lecture Demonstrations Organic Chemistry Super Absorbent Polymer – Sodium Polyacrylate Description: A solidified gel is formed when water is poured into a container with sodium polyacrylate powder. Materials: Sodium polyacrylate Beaker w/ glass stir rod NaCl Deionized water Procedure: 1. Add 0.5 g of sodium polyacrylate to a beaker (or Styrofoam cup). To this, add water (for visual effect add food coloring) and stir mixture until gel forms. A salt water solution can be added to this gel to “melt” the gel and retain a liquid mixture. 2. This demonstration is commonly performed to younger audiences as a magic trick in which water can be made to disappear by adding it to an “empty” cup. The cup actually contains the absorbent polymer and a solid mass is formed. The cup can be tilted and no water is spilled. Discussion: Sodium polyacrylate (below w/ crosslink) is the absorbing agent found in disposable diapers. This polymer can absorb up to 800 times its own weight in distilled water, 300 times in tap water and 60 times in 0.9% NaCl (a standard solution to mimic urine absorbency). The difference in these three solutions is the electrolyte concentration. This is due to the property of this polymer that increases osmotic pressure under low electrolyte concentrations, allowing the polymer to swell and decreases osmotic pressure under higher electrolyte concentrations causing release of water from the polymer. In deionized water, water is absorbed by the polymer to lower the [Na +] inside the polymer. When salt water is added to the gel, the electrolyte concentration outside of the polymer increases and water exits the polymer to equilibrate [Na +].