PTCH1 Mutation in a Patient with Metastatic Undifferentiated
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hedgehog Signaling Is Evolutionarily Conserved Cilium-Independent
Downloaded from genesdev.cshlp.org on August 14, 2009 - Published by Cold Spring Harbor Laboratory Press Cilium-independent regulation of Gli protein function by Sufu in Hedgehog signaling is evolutionarily conserved Miao-Hsueh Chen, Christopher W. Wilson, Ya-Jun Li, et al. Genes Dev. 2009 23: 1910-1928 Access the most recent version at doi:10.1101/gad.1794109 Supplemental http://genesdev.cshlp.org/content/suppl/2009/07/23/23.16.1910.DC1.html Material References This article cites 97 articles, 47 of which can be accessed free at: http://genesdev.cshlp.org/content/23/16/1910.full.html#ref-list-1 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at the service top right corner of the article or click here To subscribe to Genes & Development go to: http://genesdev.cshlp.org/subscriptions Copyright © 2009 by Cold Spring Harbor Laboratory Press Downloaded from genesdev.cshlp.org on August 14, 2009 - Published by Cold Spring Harbor Laboratory Press Cilium-independent regulation of Gli protein function by Sufu in Hedgehog signaling is evolutionarily conserved Miao-Hsueh Chen,1,3 Christopher W. Wilson,1,3 Ya-Jun Li,1 Kelvin King Lo Law,2 Chi-Sheng Lu,1 Rhodora Gacayan,1 Xiaoyun Zhang,2 Chi-chung Hui,2 and Pao-Tien Chuang1,4 1Cardiovascular Research Institute, University of California at San Francisco, San Francisco, California 94158, USA; 2Program in Developmental and Stem Cell Biology, The Hospital for Sick Children, and Department of Molecular Genetics, University of Toronto, Toronto, Ontario M5G 1L7, Canada A central question in Hedgehog (Hh) signaling is how evolutionarily conserved components of the pathway might use the primary cilium in mammals but not fly. -

Genetic Mutations Underlying Phenotypic Plasticity in Basosquamous Carcinoma Audris Chiang1,2,7, Caroline Z
See related commentary on pg 2258 ORIGINAL ARTICLE Genetic Mutations Underlying Phenotypic Plasticity in Basosquamous Carcinoma Audris Chiang1,2,7, Caroline Z. Tan1,7, Franc¸ois Kuonen1, Luqman M. Hodgkinson1, Felicia Chiang3, Raymond J. Cho4, Andrew P. South5,JeanY.Tang1, Anne Lynn S. Chang1, Kerri E. Rieger1,6, Anthony E. Oro1 and Kavita Y. Sarin1 Basosquamous carcinoma (BSC) is an aggressive skin neoplasm with the features of both basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). While genetic drivers of BCC and SCC development have been extensively characterized, BSC has not been well studied, and it remains unclear whether these tumors orig- inally derive from BCC or SCC. In addition, it is unknown which molecular pathways mediate the reprog- ramming of tumor keratinocytes toward basaloid or squamatized phenotypes. We sought to characterize the genomic alterations underlying sporadic BSC to elucidate the derivation of these mixed tumors. We identifed frequent Hedgehog (Hh) pathway mutations in BSCs, implicating Hh deregulation as the primary driving event in BSC. Principal component analysis of BCC and SCC driver genes further demonstrate the genetic similarity between BCC and BSC. In addition, 45% of the BSCs harbor recurrent mutations in the SWI/SNF complex gene, ARID1A, and evolutionary analysis revealed that ARID1A mutations occur after PTCH1 but before SCC driver mutations, indicating that ARID1A mutations may bestow plasticity enabling squamatization. Finally, we demonstrate mitogen-activated protein kinase pathway activation and the loss of Hh signaling associated with the squamatization of BSCs. Overall, these results support the genetic derivation of BSCs from BCCs and highlight potential factors involved in modulating tumor reprogramming between basaloid and squamatized phenotypes. -

Recent Advances in Signaling Pathways Comprehension As Carcinogenesis Triggers in Basal Cell Carcinoma
Journal of Clinical Medicine Review Recent Advances in Signaling Pathways Comprehension as Carcinogenesis Triggers in Basal Cell Carcinoma Mircea Tampa 1,2, Simona Roxana Georgescu 1,2,*, Cristina Iulia Mitran 3, Madalina Irina Mitran 3, Clara Matei 1, Cristian Scheau 4 , Carolina Constantin 5,6 and Monica Neagu 5,6,7 1 Department of Dermatology, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania; [email protected] (M.T.); [email protected] (C.M.) 2 Department of Dermatology, “Victor Babes” Clinical Hospital for Infectious Diseases, 030303 Bucharest, Romania 3 Department of Microbiology, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania; [email protected] (C.I.M.); [email protected] (M.I.M.) 4 Department of Physiology, “Carol Davila” University of Medicine and Pharmacy, 050474 Bucharest, Romania; [email protected] 5 Immunology Department, “Victor Babes” National Institute of Pathology, 050096 Bucharest, Romania; [email protected] (C.C.); [email protected] (M.N.) 6 Colentina Clinical Hospital, 020125 Bucharest, Romania 7 Faculty of Biology, University of Bucharest, 76201 Bucharest, Romania * Correspondence: [email protected] Received: 18 July 2020; Accepted: 16 September 2020; Published: 18 September 2020 Abstract: Basal cell carcinoma (BCC) is the most common malignant skin tumor. BCC displays a different behavior compared with other neoplasms, has a slow evolution, and metastasizes very rarely, but sometimes it causes an important local destruction. Chronic ultraviolet exposure along with genetic factors are the most important risk factors involved in BCC development. Mutations in the PTCH1 gene are associated with Gorlin syndrome, an autosomal dominant disorder characterized by the occurrence of multiple BCCs, but are also the most frequent mutations observed in sporadic BCCs. -

Loss of the PTCH1 Tumor Suppressor Defines a New
Banerjee et al. J Transl Med (2019) 17:246 https://doi.org/10.1186/s12967-019-1995-z Journal of Translational Medicine RESEARCH Open Access Loss of the PTCH1 tumor suppressor defnes a new subset of plexiform fbromyxoma Sudeep Banerjee1,2, Christopher L. Corless3, Markku M. Miettinen4, Sangkyu Noh1, Rowan Ustoy1, Jessica L. Davis3, Chih‑Min Tang1, Mayra Yebra1, Adam M. Burgoyne5 and Jason K. Sicklick1* Abstract Background: Plexiform fbromyxoma (PF) is a rare gastric tumor often confused with gastrointestinal stromal tumor. These so‑called “benign” tumors often present with upper GI bleeding and gastric outlet obstruction. It was recently demonstrated that approximately one‑third of PF have activation of the GLI1 oncogene, a transcription factor in the hedgehog (Hh) pathway, via a MALAT1‑GLI1 fusion protein or GLI1 up‑regulation. Despite this discovery, the biology of most PFs remains unknown. Methods: Next generation sequencing (NGS) was performed on formalin‑fxed parafn‑embedded (FFPE) samples of PF specimens collected from three institutions (UCSD, NCI and OHSU). Fresh frozen tissue from one tumor was utilized for in vitro assays, including quantitative RT‑PCR and cell viability assays following drug treatment. Results: Eight patients with PF were identifed and 5 patients’ tumors were analyzed by NGS. An index case had a mono‑allelic PTCH1 deletion of exons 15–24 and a second case, identifed in a validation cohort, also had a PTCH1 gene loss associated with a suspected long‑range chromosome 9 deletion. Building on the role of Hh signaling in PF, PTCH1, a tumor suppressor protein, functions upstream of GLI1. Loss of PTCH1 induces GLI1 activation and down‑ stream gene transcription. -

Understanding the Application: NGS Panel Testing for Hereditary Cancer Syndromes and Cancer Targeted Therapy
Understanding the Application: NGS Panel Testing for Hereditary Cancer Syndromes and Cancer Targeted Therapy Felicitas L. Lacbawan, MD, FCAP, FACMG Medical Director, Genetics Quest Diagnostics Nichols Institute, San Juan Capistrano, CA USA February 9, 2016 [email protected] http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf 2 http://www.nature.com/onc/journal/v23/n38/full/1207714a.html Hereditary Cancers About 5% to 10% of all cancers Inheriting a gene mutation or pathogenic variant does not necessarily mean that a person will develop cancer, but it increases his/her risk Most common hereditary cancers are: Breast cancer Ovarian cancer Colorectal cancer Prostate cancer Understanding if cancer is due to an inherited pathogenic variant/mutation can help clarify future risks of developing cancer and help determine options for cancer screening and prevention, possibly therapy 5 Lifetime Cancer Risks for Common Cancers Cancer Risk (%) Cancer Type http://seer.cancer.gov/ Lifetime Risks: Breast Cancer “Red Flags” for Inherited Susceptibility to Cancer Cancer in 2 or more closely related relatives Multiple generations affected Early age at diagnosis Multiple primary tumors Bilateral or rare cancers Constellation of tumors consistent with a specific cancer syndrome Certain ethnic backgrounds (e.g. Ashkenazi Jewish ancestry) 8 Assessing Patient’s Family History Ovarian, 52 Breast, 42 Breast, 45 9 Cost per Genome Decreasing Dramatically Diagnostic Applications of Sequencing -

Coincident Two Mutations and One Single Nucleotide Polymorphism of the PTCH1 Gene in a Family with Naevoid Basal Cell Carcinoma Syndrome
Letters to the Editor 635 Coincident Two Mutations and One Single Nucleotide Polymorphism of the PTCH1 Gene in a Family with Naevoid Basal Cell Carcinoma Syndrome Shoko Abe1, Kenji Kabashima1*, Jun-ichi Sakabe1, Takatoshi Shimauchi1, Zhang Yan2, Tetsuji Okamoto2 and Yoshiki Tokura1 1Department of Dermatology, University of Occupational and Environmental Health, 1-1 Iseigaoka, Yahatanishi-ku, Kitakyushu 807-8555, and 2Department of Molecular Oral Medicine and Maxillofacial Surgery 1, Division of Frontier Medical Science, Graduate School of Biomedical Sciences, Hiroshima University, Hiroshima, Japan. E-mail: [email protected] Accepted May 7, 2008. Sir, at nucleotide position 667 within exon 3 and an intervening se- Naevoid basal cell carcinoma syndrome (NBCCS, OMIM quence (IVS)16 -3T > C, and a SNP; IVS10 -8T > C, were detected in all three cases. A deletion of AGAC causes a frameshift and a #109400), also called Gorlin’s syndrome, is an autosomal subsequent stop codon in exon 3, which prematurely truncates dominant disease that affects about 1 in 60,000 indivi- the protein (Fig. 1a). In addition, the IVS16 -3T > C could lead duals (1, 2). NBCCS is associated with various skeletal to an aberrant splicing and truncation of PTCH1 (10–12). and neurocutaneous abnormalities. Major manifestations To detect the expression level of PTCH1 protein in the skin, are multiple basal cell carcinomas (BCCs), odontogenic an immunohistochemical study was performed using goat poly- clonal anti-PTCH1 antibody (G-19; Santa Cruz Biotechnology, keratocysts, palmoplantar dyskeratotic pits and intra- Santa Cruz, CA, USA). Enzyme reactions were developed with cranial calcification (3). In addition, rib and vertebral conventional substrates for diamino-benzidine (Sigma, St Louis, malformations, epidermal cysts, macrocephaly, facial MO, USA) (13). -
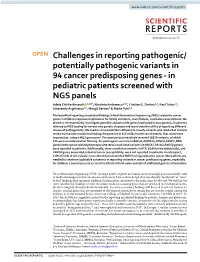
Challenges in Reporting Pathogenic/Potentially
www.nature.com/scientificreports OPEN Challenges in reporting pathogenic/ potentially pathogenic variants in 94 cancer predisposing genes - in pediatric patients screened with NGS panels Adela Chirita-Emandi 1,2,6*, Nicoleta Andreescu1,2,6, Cristian G. Zimbru1,3, Paul Tutac1,2, Smaranda Arghirescu4,5, Margit Serban5 & Maria Puiu1,2 The beneft of reporting unsolicited fndings in Next Generation Sequencing (NGS) related to cancer genes in children may have implications for family members, nevertheless, could also cause distress. We aimed to retrospectively investigate germline variants in 94 genes implicated in oncogenesis, in patients referred to NGS testing for various rare genetic diseases and reevaluate the utility of reporting diferent classes of pathogenicity. We used in silico prediction software to classify variants and conducted manual review to examine unsolicited fndings frequencies in 145 children with rare diseases, that underwent sequencing - using a 4813 gene panel. The anonymized reanalysis revealed 18250 variants, of which 126 were considered after fltering. Six pathogenic variants (in BRCA1,BMPR1A,FANCA,FANCC,NBN genes) with cancer related phenotype and three unsolicited variants (in BRCA2,PALB2,RAD50 genes) were reported to patients. Additionally, three unsolicited variants in ATR, BLM (in two individuals), and FANCB genes presented potential cancer susceptibility, were not reported to patients. In retrospect, 4.8% (7/145) of individuals in our cohort had unsolicited NGS fndings related to cancer. More eforts are needed to create an updatable consensus in reporting variants in cancer predisposing genes, especially for children. Consent process is crucial to inform of both value and risk of additional genetic information. Next-Generation Sequencing (NGS) for large panels of genes or exomes are increasingly and successfully used in medical management for rare diseases and cancer. -

Review of the Molecular Genetics of Basal Cell Carcinoma; Inherited Susceptibility, Somatic Mutations, and Targeted Therapeutics
cancers Review Review of the Molecular Genetics of Basal Cell Carcinoma; Inherited Susceptibility, Somatic Mutations, and Targeted Therapeutics James M. Kilgour , Justin L. Jia and Kavita Y. Sarin * Department of Dermatology, Stanford University School of Medcine, Stanford, CA 94305, USA; [email protected] (J.M.K.); [email protected] (J.L.J.) * Correspondence: [email protected] Simple Summary: Basal cell carcinoma is the most common human cancer worldwide. The molec- ular basis of BCC involves an interplay of inherited genetic susceptibility and somatic mutations, commonly induced by exposure to UV radiation. In this review, we outline the currently known germline and somatic mutations implicated in the pathogenesis of BCC with particular attention paid toward affected molecular pathways. We also discuss polymorphisms and associated phenotypic traits in addition to active areas of BCC research. We finally provide a brief overview of existing non-surgical treatments and emerging targeted therapeutics for BCC such as Hedgehog pathway inhibitors, immune modulators, and histone deacetylase inhibitors. Abstract: Basal cell carcinoma (BCC) is a significant public health concern, with more than 3 million cases occurring each year in the United States, and with an increasing incidence. The molecular basis of BCC is complex, involving an interplay of inherited genetic susceptibility, including single Citation: Kilgour, J.M.; Jia, J.L.; Sarin, nucleotide polymorphisms and genetic syndromes, and sporadic somatic mutations, often induced K.Y. Review of the Molecular Genetics of Basal Cell Carcinoma; by carcinogenic exposure to UV radiation. This review outlines the currently known germline and Inherited Susceptibility, Somatic somatic mutations implicated in the pathogenesis of BCC, including the key molecular pathways Mutations, and Targeted affected by these mutations, which drive oncogenesis. -

Underestimated PTCH1 Mutation Rate in Sporadic Keratocystic Odontogenic Tumors Q
Oral Oncology 51 (2015) 40–45 Contents lists available at ScienceDirect Oral Oncology journal homepage: www.elsevier.com/locate/oraloncology Underestimated PTCH1 mutation rate in sporadic keratocystic odontogenic tumors q Jiafei Qu a, Feiyan Yu a, Yingying Hong a, Yanyan Guo a, Lisha Sun b, Xuefen Li b, Jianyun Zhang a, ⇑ ⇑ Heyu Zhang b, Ruirui Shi b, Feng Chen b, , Tiejun Li a, a Department of Oral Pathology, Peking University School and Hospital of Stomatology, Beijing, China b Central Laboratory, Peking University School and Hospital of Stomatology, Beijing, China article info summary Article history: Objectives: Keratocystic odontogenic tumors (KCOTs) are benign cystic lesions of the jaws that occur spo- Received 11 July 2014 radically in isolation or in association with nevoid basal cell carcinoma syndrome (NBCCS). The protein Received in revised form 29 August 2014 patched homolog 1 gene (PTCH1) is associated with NBCCS development and tumor genesis associated Accepted 26 September 2014 with this syndrome. However, previous studies have revealed that more than 85% of syndromic KCOTs Available online 18 November 2014 and less than 30% of sporadic KCOTs harbor PTCH1 mutations. The significantly lower PTCH1 mutation rates observed in sporadic KCOTs suggest that they serve a minor role in pathogenesis. We aimed to Keywords: discern the importance of PTCH1 mutations in sporadic KCOTs. PTCH1 Materials and methods: PTCH1 mutational analysis was performed with 19 new sporadic KCOT cases by Mutation Keratocystic odontogenic tumors direct sequencing of epithelial lining samples separated from fibrous capsules. Using this approach, we further reexamined 9 sporadic KCOTs that were previously reported to lack PTCH1 mutations by our group. -

Intraepithelial Paracrine Hedgehog Signaling Induces the Expansion Of
Developmental Biology 372 (2012) 28–44 Contents lists available at SciVerse ScienceDirect Developmental Biology journal homepage: www.elsevier.com/locate/developmentalbiology Intraepithelial paracrine Hedgehog signaling induces the expansion of ciliated cells that express diverse progenitor cell markers in the basal epithelium of the mouse mammary gland Elena Garcı´a-Zaragoza a, Raquel Pe´rez-Tavarez a, Alicia Ballester b, Vanesa Lafarga c,1, Anaı¨s Jime´nez-Reinoso a,A´ ngel Ramı´rez c, Rodolfo Murillas c,d, Marta I. Gallego a,n a Laboratory of Mammary Pathology, Centro Nacional de Microbiologı´a, Instituto de Salud Carlos III, Carretera de Majadahonda a Pozuelo Km 2, Majadahonda 28220, Madrid, Spain b Laboratory of Gene Regulation, Department of Cell and Developmental Biology, Centro Nacional de Microbiologı´a, Instituto de Salud Carlos III, Carretera de Majadahonda a Pozuelo Km 2, Majadahonda 28220, Madrid, Spain c Epithelial Biomedicine Division, CIEMAT U714, Avenida Complutense, 40, Madrid 28040, Spain d CIBERER (Center for Biomedical Research on Rare Diseases) U714, Avenida Complutense, 40, Madrid 28040, Spain article info abstract Article history: The Hedgehog signaling pathway regulates embryo patterning and progenitor cell homeostasis in adult Received 11 November 2011 tissues, including epidermal appendages. A role for the Hh pathway in mammary biology and breast Received in revised form cancer has also been suggested. The aim of this study was to analyze Hh signaling in the mouse 10 September 2012 mammary gland through the generation of transgenic mice that express Sonic Hedgehog (Shh) under Accepted 11 September 2012 the control of the mammary-specific WAP promoter (WAP-Shh mice). -

Regulation of Sonic Hedgehog-GLI1 Downstream Target Genes PTCH1
Shahi et al. BMC Cancer 2010, 10:614 http://www.biomedcentral.com/1471-2407/10/614 RESEARCH ARTICLE Open Access Regulation of sonic hedgehog-GLI1 downstream target genes PTCH1, Cyclin D2, Plakoglobin, PAX6 and NKX2.2 and their epigenetic status in medulloblastoma and astrocytoma Mehdi H Shahi1,2,3, Mohammad Afzal2, Subrata Sinha3, Charles G Eberhart4, Juan A Rey5, Xing Fan6, Javier S Castresana1* Abstract Background: The Sonic hedgehog (Shh) signaling pathway is critical for cell growth and differentiation. Impairment of this pathway can result in both birth defects and cancer. Despite its importance in cancer development, the Shh pathway has not been thoroughly investigated in tumorigenesis of brain tumors. In this study, we sought to understand the regulatory roles of GLI1, the immediate downstream activator of the Shh signaling pathway on its downstream target genes PTCH1, Cyclin D2, Plakoglobin, NKX2.2 and PAX6 in medulloblastoma and astrocytic tumors. Methods: We silenced GLI1 expression in medulloblastoma and astrocytic cell lines by transfection of siRNA against GLI1. Subsequently, we performed RT-PCR and quantitative real time RT-PCR (qRT-PCR) to assay the expression of downstream target genes PTCH1, Cyclin D2, Plakoglobin, NKX2.2 and PAX6. We also attempted to correlate the pattern of expression of GLI1 and its regulated genes in 14 cell lines and 41 primary medulloblastoma and astrocytoma tumor samples. We also assessed the methylation status of the Cyclin D2 and PTCH1 promoters in these 14 cell lines and 58 primary tumor samples. Results: Silencing expression of GLI1 resulted up-regulation of all target genes in the medulloblastoma cell line, while only PTCH1 was up-regulated in astrocytoma. -
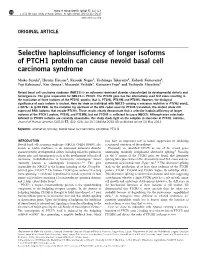
Selective Haploinsufficiency of Longer Isoforms of PTCH1 Protein Can
Journal of Human Genetics (2012) 57, 422–426 & 2012 The Japan Society of Human Genetics All rights reserved 1434-5161/12 $32.00 www.nature.com/jhg ORIGINAL ARTICLE Selective haploinsufficiency of longer isoforms of PTCH1 protein can cause nevoid basal cell carcinoma syndrome Maiko Suzuki1, Hiromi Hatsuse1, Kazuaki Nagao1, Yoshinaga Takayama1, Kohzoh Kameyama1, Yuji Kabasawa2, Ken Omura2, Masayuki Yoshida3, Katsunori Fujii4 and Toshiyuki Miyashita1 Nevoid basal cell carcinoma syndrome (NBCCS) is an autosomal dominant disorder characterized by developmental defects and tumorigenesis. The gene responsible for NBCCS is PTCH1. The PTCH1 gene has five alternatively used first exons resulting in the translation of three isoforms of the PTCH1 protein; that is, PTCHL, PTCHM and PTCHS. However, the biological significance of each isoform is unclear. Here we show an individual with NBCCS carrying a nonsense mutation in PTCH1 exon2, c.387G4A (p.W129X). As the mutation lay upstream of the ATG codon used for PTCHS translation, the mutant allele still expressed RNA isoforms that encode PTCHS. These results clearly demonstrate that a selective haploinsufficiency of longer isoforms of the PTCH1 protein, PTCHL and PTCHM, but not PTCHS is sufficient to cause NBCCS. Although mice selectively deficient in PTCHS isoforms are currently unavailable, this study sheds light on the complex in vivo roles of PTCH1 isoforms. Journal of Human Genetics (2012) 57, 422–426; doi:10.1038/jhg.2012.45; published online 10 May 2012 Keywords: alternative splicing; nevoid basal cell carcinoma syndrome; PTCH1 INTRODUCTION may have an important role in tumor suppression by inhibiting Nevoid basal cell carcinoma syndrome (NBCCS; OMIM 109400), also a sustained activation of the pathway.