1078-0432.CCR-17-1960.Full-Text.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mrna Vaccine Era—Mechanisms, Drug Platform and Clinical Prospection
International Journal of Molecular Sciences Review mRNA Vaccine Era—Mechanisms, Drug Platform and Clinical Prospection 1, 1, 2 1,3, Shuqin Xu y, Kunpeng Yang y, Rose Li and Lu Zhang * 1 State Key Laboratory of Genetic Engineering, Institute of Genetics, School of Life Science, Fudan University, Shanghai 200438, China; [email protected] (S.X.); [email protected] (K.Y.) 2 M.B.B.S., School of Basic Medical Sciences, Peking University Health Science Center, Beijing 100191, China; [email protected] 3 Shanghai Engineering Research Center of Industrial Microorganisms, Shanghai 200438, China * Correspondence: [email protected]; Tel.: +86-13524278762 These authors contributed equally to this work. y Received: 30 July 2020; Accepted: 30 August 2020; Published: 9 September 2020 Abstract: Messenger ribonucleic acid (mRNA)-based drugs, notably mRNA vaccines, have been widely proven as a promising treatment strategy in immune therapeutics. The extraordinary advantages associated with mRNA vaccines, including their high efficacy, a relatively low severity of side effects, and low attainment costs, have enabled them to become prevalent in pre-clinical and clinical trials against various infectious diseases and cancers. Recent technological advancements have alleviated some issues that hinder mRNA vaccine development, such as low efficiency that exist in both gene translation and in vivo deliveries. mRNA immunogenicity can also be greatly adjusted as a result of upgraded technologies. In this review, we have summarized details regarding the optimization of mRNA vaccines, and the underlying biological mechanisms of this form of vaccines. Applications of mRNA vaccines in some infectious diseases and cancers are introduced. It also includes our prospections for mRNA vaccine applications in diseases caused by bacterial pathogens, such as tuberculosis. -

Small RNA Fragments Derived from Multiple RNA Classes – the Missing
Jackowiak et al. BMC Genomics (2017) 18:502 DOI 10.1186/s12864-017-3891-3 RESEARCHARTICLE Open Access Small RNA fragments derived from multiple RNA classes – the missing element of multi-omics characteristics of the hepatitis C virus cell culture model Paulina Jackowiak1, Anna Hojka-Osinska1, Anna Philips1, Agnieszka Zmienko1,2, Lucyna Budzko1, Patrick Maillard3, Agata Budkowska3,4 and Marek Figlerowicz1,2* Abstract Background: A pool of small RNA fragments (RFs) derived from diverse cellular RNAs has recently emerged as a rich source of functionally relevant molecules. Although their formation and accumulation has been connected to various stress conditions, the knowledge on RFs produced upon viral infections is very limited. Here, we applied the next generation sequencing (NGS) to characterize RFs generated in the hepatitis C virus (HCV) cell culture model (HCV-permissive Huh-7.5 cell line). Results: We found that both infected and non-infected cells contained a wide spectrum of RFs derived from virtually all RNA classes. A significant fraction of identified RFs accumulated to similar levels as miRNAs. Our analysis, focused on RFs originating from constitutively expressed non-coding RNAs, revealed three major patterns of parental RNA cleavage. We found that HCV infection induced significant changes in the accumulation of low copy number RFs, while subtly altered the levels of high copy number ones. Finally, the candidate RFs potentially relevant for host-virus interactions were identified. Conclusions: Our results indicate that RFs should be considered an important component of the Huh-7.5 transcriptome and suggest that the main factors influencing the RF biogenesis are the RNA structure and RNA protection by interacting proteins. -

Explore the RNA Universe!
Explore the RNA Universe! Circulating cell-free RNA (ccfRNA) Exosomes Exosomal RNA (exRNA) Ribonuclease P (RNase P) Small (short) interfering RNA (siRNA) Pre-miRNA Small nucleolar RNA Exportin-5 (snoRNA) MicroRNA (miRNA) Drosha Pri-miRNA RISC DGCR8 Ribosomal RNA (rRNA) Small nuclear RNA Ribonuclease MRP Y RNA (snRNA) (RNase MRP) Long non-coding RNA Messenger RNA (mRNA) (IncRNA) Transfer RNA (tRNA) Telomerase RNA Ribosomes Signal recognition particle RNA (SRP RNA) Mitochondria Piwi-interacting RNA (piRNA) Sample to Insight Explore the RNA Universe! RNA function RNA type Detailed role in the cell Protein synthesis Messenger RNA (mRNA) Carrying the genetic information copied from DNA in the form of three-nucleotide bases “codon,” each specifying a particular amino acid for protein synthesis at the ribosomes. Purify with: RNeasy® Plus Kits*, RNeasy Kits*, QIAamp® RNA Blood Kit*, QIAcube® Assay using: QuantiNova® Kits, RT2 Profiler™ PCR Assays and Arrays, Rotor-Gene® Q , QIAseq™ Targeted RNA Panels, QIAseq Stranded mRNA Select Library Kit, QIAseq UPX 3' Targeted RNA Panel, QIAseq UPX 3' Transcriptome RNA Library Kit, QIAseq Targeted RNAscan Panels, QIAseq FX Single Cell RNA Library Kit Transfer RNA Adapter molecule bringing the amino acid corresponding to a specific mRNA codon to the ribosome. Having an anticodon (complementary to the codon), a site (tRNA) binding a specific amino acid and a site binding aminoacyl-tRNA synthetase (enzyme catalyzing amino acid-tRNA binding). Ribosomal RNA (rRNA) RNA component of the ribosome, where protein is translated. Ribosomes align the anticodon of tRNA with the mRNA codon and are required for the peptidyl transferase activity catalyzing the assembly of amino acids into protein chains. -

Revealing the Missing Expressed Genes Beyond the Human Reference
Chen et al. BMC Genomics 2011, 12:590 http://www.biomedcentral.com/1471-2164/12/590 RESEARCH ARTICLE Open Access Revealing the missing expressed genes beyond the human reference genome by RNA-Seq Geng Chen1, Ruiyuan Li2, Leming Shi3, Junyi Qi1, Pengzhan Hu1, Jian Luo1, Mingyao Liu1 and Tieliu Shi1,4* Abstract Background: The complete and accurate human reference genome is important for functional genomics researches. Therefore, the incomplete reference genome and individual specific sequences have significant effects on various studies. Results: we used two RNA-Seq datasets from human brain tissues and 10 mixed cell lines to investigate the completeness of human reference genome. First, we demonstrated that in previously identified ~5 Mb Asian and ~5 Mb African novel sequences that are absent from the human reference genome of NCBI build 36, ~211 kb and ~201 kb of them could be transcribed, respectively. Our results suggest that many of those transcribed regions are not specific to Asian and African, but also present in Caucasian. Then, we found that the expressions of 104 RefSeq genes that are unalignable to NCBI build 37 in brain and cell lines are higher than 0.1 RPKM. 55 of them are conserved across human, chimpanzee and macaque, suggesting that there are still a significant number of functional human genes absent from the human reference genome. Moreover, we identified hundreds of novel transcript contigs that cannot be aligned to NCBI build 37, RefSeq genes and EST sequences. Some of those novel transcript contigs are also conserved among human, chimpanzee and macaque. By positioning those contigs onto the human genome, we identified several large deletions in the reference genome. -
Coding RNA Genes
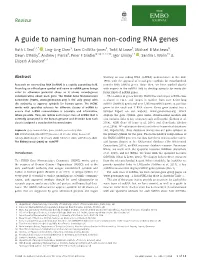
Review A guide to naming human non-coding RNA genes Ruth L Seal1,2,* , Ling-Ling Chen3, Sam Griffiths-Jones4, Todd M Lowe5, Michael B Mathews6, Dawn O’Reilly7, Andrew J Pierce8, Peter F Stadler9,10,11,12,13, Igor Ulitsky14 , Sandra L Wolin15 & Elspeth A Bruford1,2 Abstract working on non-coding RNA (ncRNA) nomenclature in the mid- 1980s with the approval of initial gene symbols for mitochondrial Research on non-coding RNA (ncRNA) is a rapidly expanding field. transfer RNA (tRNA) genes. Since then, we have worked closely Providing an official gene symbol and name to ncRNA genes brings with experts in the ncRNA field to develop symbols for many dif- order to otherwise potential chaos as it allows unambiguous ferent kinds of ncRNA genes. communication about each gene. The HUGO Gene Nomenclature The number of genes that the HGNC has named per ncRNA class Committee (HGNC, www.genenames.org) is the only group with is shown in Fig 1, and ranges in number from over 4,500 long the authority to approve symbols for human genes. The HGNC ncRNA (lncRNA) genes and over 1,900 microRNA genes, to just four works with specialist advisors for different classes of ncRNA to genes in the vault and Y RNA classes. Every gene symbol has a ensure that ncRNA nomenclature is accurate and informative, Symbol Report on our website, www.genenames.org, which where possible. Here, we review each major class of ncRNA that is displays the gene symbol, gene name, chromosomal location and currently annotated in the human genome and describe how each also includes links to key resources such as Ensembl (Zerbino et al, class is assigned a standardised nomenclature. -

Long Noncoding Rnas Involvement in Epstein-Barr Virus Infection And
Zhang et al. Virology Journal (2020) 17:51 https://doi.org/10.1186/s12985-020-01308-y REVIEW Open Access Long noncoding RNAs involvement in Epstein-Barr virus infection and tumorigenesis Jing Zhang1,2,3, Xiaohan Li1,2,3, Jingjin Hu1,2,3, Pengfei Cao2, Qijia Yan1,2, Siwei Zhang1,2,3, Wei Dang1,2,3 and Jianhong Lu1,2* Abstract The Epstein-Barr virus (EBV) is a ubiquitous γ-herpesvirus related to various types of cancers, including epithelial nasopharyngeal carcinoma, gastric carcinoma, and lymphoma. Long noncoding RNAs (lncRNAs) are expressed extensively in mammalian cells and play crucial roles in regulating various cellular processes and multiple cancers. Cellular lncRNAs can be differentially expressed induced by EBV infection. The dysregulated lncRNAs probably modulate the host immune response and other biological functions. At present, lncRNAs have been found to be significantly increased or decreased in EBV-infected cells, exosomes and EBV-associated cancers, suggesting their potential function and clinical application as biomarkers. In addition, EBV-encoded lncRNAs, BART and BHLF1 lncRNAs, may play roles in the viral oncogenesis. Analysis of the specific lncRNAs involved in interactions with the EBV machinery will provide information on their potential mechanism of action during multiple steps of EBV tumorigenesis. Here, we review the current knowledge regarding EBV- related lncRNAs and their possible roles in the pathogenesis of EBV-associated cancers. Keywords: Long noncoding RNA, Epstein-Barr virus, Tumorigenesis, Epithelial cancer, Lymphoma Background lymphoma, nasopharyngeal carcinoma (NPC), gastric can- Epstein-Barr virus (EBV) is a ubiquitous γ-herpesvirus, cer (GC), Hodgkin’s disease and breast cancer [1, 2]. -

Why Y Rnas? About Versatile Rnas and Their Functions
Biomolecules 2013, 3, 143-156; doi:10.3390/biom3010143 OPEN ACCESS biomolecules ISSN 2218-273X www.mdpi.com/journal/biomolecules/ Review Why Y RNAs? About Versatile RNAs and Their Functions Marcel Köhn, Nikolaos Pazaitis and Stefan Hüttelmaier * Martin-Luther-University Halle-Wittenberg, Institute of Molecular Medicine, Section Molecular Cell Biology, ZAMED, Heinrich-Damerow-Str.1, D-6120 Halle, Germany; E-Mails: [email protected] (M.K.) [email protected] (N.P.) * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel.: +0049-(0)3455522860; Fax: +0049-(0)3455522894. Received: 31 December 2012; in revised form: 27 January 2013 / Accepted: 31 January 2013 / Published: 8 February 2013 Abstract: Y RNAs constitute a family of highly conserved small noncoding RNAs (in humans: 83-112 nt; Y1, Y3, Y4 and Y5). They are transcribed from individual genes by RNA-polymerase III and fold into conserved stem-loop-structures. Although discovered 30 years ago, insights into the cellular and physiological role of Y RNAs remains incomplete. In this review, we will discuss knowledge on the structural properties, associated proteins and discuss proposed functions of Y RNAs. We suggest Y RNAs to be an integral part of ribonucleoprotein networks within cells and could therefore have substantial influence on many different cellular processes. Putative functions of Y RNAs include small RNA quality control, DNA replication, regulation of the cellular stress response and proliferation. This suggests Y RNAs as essential regulators of cell fate and indicates future avenues of research, which will provide novel insights into the role of small noncoding RNAs in gene expression. -

RNA Metabolism Guided by RNA Modifications
biomolecules Review RNA Metabolism Guided by RNA Modifications: The Role of SMUG1 in rRNA Quality Control Lisa Lirussi 1,2 , Özlem Demir 3, Panpan You 1,2, Antonio Sarno 4,5 , Rommie E. Amaro 3 and Hilde Nilsen 1,2,* 1 Department of Clinical Molecular Biology, University of Oslo, 0318 Oslo, Norway; [email protected] (L.L.); [email protected] (P.Y.) 2 Department of Clinical Molecular Biology (EpiGen), Akershus University Hospital, 1478 Lørenskog, Norway 3 Department of Chemistry and Biochemistry, University of California San Diego, La Jolla, CA 92093, USA; [email protected] (Ö.D.); [email protected] (R.E.A.) 4 Department of Clinical and Molecular Medicine, Norwegian University of Science and Technology, NTNU, NO-7491 Trondheim, Norway; [email protected] 5 SINTEF Ocean AS, 7010 Trondheim, Norway * Correspondence: [email protected]; Tel.: +47-67963922 Abstract: RNA modifications are essential for proper RNA processing, quality control, and matura- tion steps. In the last decade, some eukaryotic DNA repair enzymes have been shown to have an ability to recognize and process modified RNA substrates and thereby contribute to RNA surveil- lance. Single-strand-selective monofunctional uracil-DNA glycosylase 1 (SMUG1) is a base excision repair enzyme that not only recognizes and removes uracil and oxidized pyrimidines from DNA but is also able to process modified RNA substrates. SMUG1 interacts with the pseudouridine synthase dyskerin (DKC1), an enzyme essential for the correct assembly of small nucleolar ribonucle- oproteins (snRNPs) and ribosomal RNA (rRNA) processing. Here, we review rRNA modifications and RNA quality control mechanisms in general and discuss the specific function of SMUG1 in rRNA metabolism. -

Chicken Genome: Current Status and Future Opportunities
Downloaded from genome.cshlp.org on September 26, 2021 - Published by Cold Spring Harbor Laboratory Press Perspective Chicken genome: Current status and future opportunities David W. Burt Department of Genomics and Genetics, Roslin Institute (Edinburgh), Midlothian EH25 9PS, United Kingdom The chicken genome sequence is important for several reasons. First, the chicken shared a common ancestor with mammals ∼310 million years ago (Mya) at a phylogenetic distance not previously covered by other genome sequences. It therefore fills a gap in our knowledge and understanding of the evolution and conservation of genes, regulatory sequences, genomes, and karyotypes. The chicken is also a major source of protein in the world, with billions of birds used in meat and egg production each year. It is the first livestock species to be sequenced and so leads the way for others. The sequence and the 2.8 million genetic polymorphisms defined in a parallel project are expected to benefit agriculture and cast new light on animal domestication. Also, as the first bird to be sequenced, it is a model for the 9600 avian species thought to exist today. Many of the features of the chicken genome and its biology make it an ideal organism for studies in development and evolution, along with applications in agriculture and medicine. Avian genomics has its origins in genetic linkage mapping (Burt been an increase in the incidence of osteoporosis associated with and Cheng 1998), but our knowledge of the chicken genome has increased egg production. Given the possibility that genetic been transformed in recent years, mostly through the analysis of progress in egg and meat production will reach its limit within large numbers of partial cDNA sequences (Abdrakhmanov et al. -

Genome Sequence of the Nematode C. Elegans: a Platform for Investigating Biology the C
S PECIAL SECTION C. ELEGANS:SEQUENCE TO BIOLOGY Genome Sequence of the Nematode C. elegans: A Platform for Investigating Biology The C. elegans Sequencing Consortium* REVIEW represented only in YACs. By 1989, it became apparent that, with the physical map in hand, The 97-megabase genomic sequence of the nematode Cae- complete sequencing of the genome might be both feasible and norhabditis elegans reveals over 19,000 genes. More than 40 desirable. Joint funding [from the National Institutes of Health and the percent of the predicted protein products find significant UK Medical Research Council (MRC)] for a pilot study was arranged, matches in other organisms. There is a variety of repeated and in 1990, the first 3-megabase (Mb) sequence was undertaken. sequences, both local and dispersed. The distinctive distribu- Success in this venture (10, 11) resulted in full funding and the tion of some repeats and highly conserved genes provides expansion of the two groups of the consortium in 1993. evidence for a regional organization of the chromosomes. Sequencing began in the centers of the chromosomes, where cosmid coverage and the density of genetic markers are high. Cosmids The genome sequence of C. elegans is essentially complete. The were selected by fingerprint analysis to achieve a tiling path of sequence follows those of viruses, several bacteria, and a yeast (1, 2) overlapping clones (in practice, 25% overlap on average). Some and is the first from a multicellular organism. Some small gaps remain sequencing of YACs was explored (12), but because of yeast DNA to be closed, but this will be a prolonged process without much that contaminated preparations of YAC DNA, this approach was biological return. -

Sequence and Structure Requirements of Y RNA-Derived Small RNA Biogenesis
Sequence and structure requirements of Y RNA-derived small RNA biogenesis Carly Turnbull A thesis submitted to the University of East Anglia for the degree of Doctor of Philosophy University of East Anglia Norwich School of Biological Sciences May 2014 This copy of the thesis has been supplied on condition that anyone who consults it is understood to recognise that its copyright rests with the author and that use of any information derived there from must be in accordance with current UK Copyright Law. In addition, any quotation or extract must include full attribution. ABSTRACT Numerous small non-coding RNAs have been identified in mammalian cells, includ- ing microRNAs and piwi-interacting RNAs. The patterns of gene expression within cells can be altered in response to cellular stress. To examine the effects of cellu- lar stress on all small RNA types, a number of human cell lines were treated with Poly(I:C), a mimic of viral infection, and the levels of small RNAs were examined by next generation sequencing. Surprisingly, we did not find many differentially ex- pressed microRNAs, but we discovered a new class of small RNAs that were 30-35 nucleotides and showed up-regulation following Poly(I:C) treatment. These slightly longer small RNAs were derived from many different types of non-coding RNA and only very few small RNAs were derived directly from messenger RNAs. Small RNAs derived from various types of RNA were validated by northern blot. Further sequencing libraries were prepared for Poly(I:C)-treated and untreated MCF7 cells, as well as Poly(I:C)-treated and untreated SW1353 cells. -

Mrna Modification and Delivery Strategies Towards the Establishment of a Platform for Safe and Effective Gene Therapy
Ghent University Faculty of Veterinary Medicine mRNA modification and delivery strategies towards the establishment of a platform for safe and effective gene therapy Oliwia Andries Dissertation submitted in fulfillment of the requirements for the degree of Doctor of Philosophy (PhD) 2015 Promotor: Co-Promotors: Prof. Dr. Niek Sanders Prof. Dr. Stefaan De Smedt Laboratory of Gene Therapy, Laboratory of Biochemistry and Department of Nutrition, Ethology and Physical Pharmacy, Genetics, Faculty of Pharmaceutical Sciences, Faculty of Veterinary Medicine, Ghent University Ghent University Dr. Tasuku Kitada Synthetic Biology Center Department of Biological Engineering, Massachusetts Institute of Technology 1 The author and the promoters give the authorization to consult and to copy parts of this thesis for personal use only. Any other use is limited by the Laws of Copyright, especially the obligation to refer to the source whenever results from this thesis are cited. De auteur en de promotoren geven de toelating dit proefschrift voor consultering beschikbaar te stellen en delen ervan te kopiëren voor persoonlijk gebruik. Elk ander gebruik valt onder beperkingen van het auteursrecht, in het bijzonder met betrekking tot de verplichting uitdrukkelijk de bron te vermelden bij het aanhalen van resultaten uit dit proefschrift. Ghent, March 25th 2015 Promotor: Author: Prof. dr. Apr. Niek N. Sanders Oliwia Andries, MSc Copromotors: Prof. dr. Apr. Stefaan De Smedt Dr. Tasuku Kitada 2 Here’s to the crazy ones. The rebels. The troublemakers. The ones who see things differently. While some may see them as the crazy ones, we see genius. Because the people who are crazy enough to think they can change the world, are the ones who do.