A New Framework for Thinking About Life Extension
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 6: Old People Are People Too, So Let's Act
Career Planning & Adult Development JOURNAL Volume 31, Number 2 ISSN 0736-1920 Summer 2015 OUR FUTURE: Projections of Work and Life Helen Harkness, Guest Editor QThe Future Q The End of Work as We Know It QJobs and Careers on the Front Line of the Future QSilicon Valley and the New Rules of Work Q Training Challenges Facing Education and Training and Career Development in the Future QOld people are people too, so let’s act accordingly Q Crisis of Human Capital in Aerospace: It’s All About the STEM QCollege for All – Reality or Flawed Myth? QOur Jobs: The American Workforce and Economy in Crisis Q The Future Has Arrived: The Future is Now the Present Summer 2015..............................Career Planning and Adult Development JOURNAL..............................1 CAREER PLANNING and ADULT DEVELOPMENT JOURNAL Volume 31, Number 2 ISSN 0736-1920 Summer 2015 OUR FUTURE: Projections of Work and Life Looking Ahead with the Journal,E\Steven E. Beasley, Managing Editor4 Introduction to this Issue, E\ Helen Harkness, PhD, Guest Editor5 Chapter 1: 7KH)XWXUHE\ Leigh Ellen Key8 Chapter 2: 7KH(QGRI:RUNDV:H.QRZ,Wby Andy Hines10 Chapter 3: -REVDQG&DUHHUVRQWKH)URQW/LQHRIWKH)XWXUHby Gary Marx20 Chapter 4: 6LOLFRQ9DOOH\DQGWKH1HZ5XOHVRI:RUNE\Gary A. Bolles28 Chapter 5: 7UDLQLQJ&KDOOHQJHV)DFLQJ(GXFDWLRQDQG7UDLQLQJ DQG&DUHHU'HYHORSPHQWLQWKH)XWXUHE\Timothy C. Mack40 Chapter 6: 2OGSHRSOHDUHSHRSOHWRRVROHW·VDFWDFFRUGLQJO\by Aubrey de Grey47 Chapter 7: &ULVLVRI+XPDQ&DSLWDOLQ$HURVSDFH,W·V$OO$ERXWWKH67(0 by Deborah Westphal51 Chapter 8: &ROOHJHIRU$OO²5HDOLW\RU)ODZHG0\WK"E\ -

Mixing Old and Young: Enhancing Rejuvenation and Accelerating Aging
Mixing old and young: enhancing rejuvenation and accelerating aging Ashley Lau, … , James L. Kirkland, Stefan G. Tullius J Clin Invest. 2019;129(1):4-11. https://doi.org/10.1172/JCI123946. Review Donor age and recipient age are factors that influence transplantation outcomes. Aside from age-associated differences in intrinsic graft function and alloimmune responses, the ability of young and old cells to exert either rejuvenating or aging effects extrinsically may also apply to the transplantation of hematopoietic stem cells or solid organ transplants. While the potential for rejuvenation mediated by the transfer of youthful cells is currently being explored for therapeutic applications, aspects that relate to accelerating aging are no less clinically significant. Those effects may be particularly relevant in transplantation with an age discrepancy between donor and recipient. Here, we review recent advances in understanding the mechanisms by which young and old cells modify their environments to promote rejuvenation- or aging-associated phenotypes. We discuss their relevance to clinical transplantation and highlight potential opportunities for therapeutic intervention. Find the latest version: https://jci.me/123946/pdf REVIEW The Journal of Clinical Investigation Mixing old and young: enhancing rejuvenation and accelerating aging Ashley Lau,1 Brian K. Kennedy,2,3,4,5 James L. Kirkland,6 and Stefan G. Tullius1 1Division of Transplant Surgery, Department of Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts, USA. 2Departments of Biochemistry and Physiology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore. 3Singapore Institute for Clinical Sciences, Singapore. 4Agency for Science, Technology and Research (A*STAR), Singapore. -

Longevity Extension from a Socioeconomic Perspective: Plausibility, Misconceptions, and Potential Outcomes
Sound Decisions: An Undergraduate Bioethics Journal Volume 2 Issue 1 Article 4 2016-12-15 Longevity Extension from a Socioeconomic Perspective: Plausibility, Misconceptions, and Potential Outcomes Eric Ralph University of Puget Sound Follow this and additional works at: https://soundideas.pugetsound.edu/sounddecisions Part of the Bioethics and Medical Ethics Commons Recommended Citation Ralph, Eric (2016) "Longevity Extension from a Socioeconomic Perspective: Plausibility, Misconceptions, and Potential Outcomes," Sound Decisions: An Undergraduate Bioethics Journal: Vol. 2 : Iss. 1 , Article 4. Available at: https://soundideas.pugetsound.edu/sounddecisions/vol2/iss1/4 This Article is brought to you for free and open access by the Student Publications at Sound Ideas. It has been accepted for inclusion in Sound Decisions: An Undergraduate Bioethics Journal by an authorized editor of Sound Ideas. For more information, please contact [email protected]. Ralph: Longevity Extension Longevity Extension from a Socioeconomic Perspective: Plausibility, Misconceptions, and Potential Outcomes Eric Ralph Introduction In the last several decades, a significant amount of progress has been made in pursuits to better understand the process of aging and subsequently gain some level of control over it. Current theories of aging are admittedly lacking, but this has not prevented biogerontologists from drastically increasing the longevity of yeast, drosophilae, worms, and mice (Vaiserman, Moskalev, & Pasyukova 2015; Tosato, Zamboni et al. 2007; Riera & Dillin 2015). Wide-ranging successes with gene therapy and increased comprehension of the genetic components of aging have also recently culminated in numerous successes in extending the longevity of animals and the first human trial of a gene therapy to extend life through telomerase manipulation is already underway, albeit on a small scale (Mendell et al. -

Worms Under Stress: Unravelling Genetic Complex Traits Through Perturbation
Worms under stress: unravelling genetic complex traits through perturbation Miriam Rodriguez Sanchez Thesis committee Promotor Prof. Dr Jaap Bakker Professor of Nematology Wageningen University Co-promotor Dr Jan E. Kammenga Associate professor, Laboratory of Nematology Wageningen University Other members Prof. Dr Bas J. Zwaan, Wageningen University Prof. Dr Hendrik.C. Korswagen, Hubrecht Institute, Utrecht Prof. Dr Ellen Nollen, European Research Institute for the Biology of Ageing (ERIBA), Groningen Dr Gino B. Poulin, University of Manchester, United Kingdom This research was conducted under the auspices of the Graduate School of Production Ecology and Resource Conservation (PE&RC). Worms under stress: unravelling genetic complex traits through perturbation Miriam Rodriguez Sanchez Thesis submitted in fulfilment of the requirements for the degree of doctor at Wageningen University by the authority of the Rector Magnificus Prof. dr. M.J. Kropff, in the presence of the Thesis Committee appointed by the Academic Board to be defended in public on Friday 14 March 2014 at 11 a.m. in the Aula. Miriam Rodriguez Sanchez Worms under stress: unravelling genetic complex traits through perturbation 130 pages PhD thesis, Wageningen University, Wageningen, NL (2014) With references, with summaries in Dutch and English ISBN: 978-94-6173-851-6 A mi padre CONTENTS Contents Chapter 1 General Introduction ........................................................................... 3 Chapter 2 C. elegans stress response and its relevance to complex human disease and aging ................................................. 15 Chapter 3 Uncovering genotype specific variation of Wnt signaling in C. elegans .................................................................... 33 Chapter 4 Genetic variation for stress-response hormesis in C. elegans life span ......................................................................... 55 Chapter 5 Molecular confirmation of trans-regulatory eQTL in C. -

From Here to Immortality: Anti-Aging Medicine
FromFrom HereHere toto Immortality:Immortaalitty: AAnti-AgingAnnntti-AAgging MMedicineedicine Anti-aging medicine is a $5 billion industry. Despite its critics, researchers are discovering that inter ventions designed to turn back time may prove to be more science than fiction. By Trudie Mitschang 14 BioSupply Trends Quarterly • October 2013 he symptoms are disturbing. Weight gain, muscle Shifting Attitudes Fuel a Booming Industry aches, fatigue and joint stiffness. Some experience The notion that aging requires treatment is based on a belief Thear ing loss and diminished eyesight. In time, both that becoming old is both undesirable and unattractive. In the memory and libido will lapse, while sagging skin and inconti - last several decades, aging has become synonymous with nence may also become problematic. It is a malady that begins dete rioration, while youth is increasingly revered and in one’s late 40 s, and currently 100 percent of baby boomers admired. Anti-aging medicine is a relatively new but thriving suffer from it. No one is immune and left untreated ; it always field driven by a baby- boomer generation fighting to preserve leads to death. A frightening new disease, virus or plague? No , its “forever young” façade. According to the market research it’s simply a fact of life , and it’s called aging. firm Global Industry Analysts, the boomer-fueled consumer The mythical fountain of youth has long been the subject of base will push the U.S. market for anti-aging products from folklore, and although it is both natural and inevitable, human about $80 billion now to more than $114 billion by 2015. -

SENS-Research-Foundation-2019
by the year 2050, cardiovascular an estimated 25-30 the american 85 percent of adults disease years and older age 85 or older remains the most population will suffer from common cause of 2 1 2 dementia. death in older adults. triple. THE CLOCK IS TICKING. By 2030, annual direct The estimated cost of medical costs associated dementia worldwide was 62% of Americans with cardiovascular $818 billion diseases in the united over age 65 have in 2015 and is states are expected to more than one expected to grow to rise to more than chronic condition.1 3 $2 trillion $818 billion. by 2030.1 References: (1) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5732407/, (2) https://www.who.int/ageing/publications/global_health.pdf, (3) https://www.cdcfoundation.org/pr/2015/heart-disease-and-stroke-cost-america-nearly-1-billion-day-medical-costs-lost-productivity sens research foundation board of directors Barbara Logan Kevin Perrott Bill Liao Chairperson Treasurer Secretary Michael Boocher Kevin Dewalt James O’Neill Jonathan Cain Michael Kope Frank Schuler 02 CONTENTS 2019 Annual Report 04 Letter From The CEO 06 Outreach & Fundraising 08 Finances 09 Donors erin ashford photography 14 Education 26 Investments 20 Conferences & Events 30 Research Advisory Board 23 Speaking Engagements 31 10 Years Of Research 24 Alliance 32 MitoSENS 34 LysoSENS 35 Extramural Research 38 Publications 39 Ways to Donate cover Photo (c) Mikhail Leonov - stock.adobe.com special 10th anniversary edition 03 FROM THE CEO It’s early 2009, and it’s very late at night. Aubrey, Jeff, Sarah, Kevin, and Mike are sitting around a large table covered in papers and half-empty food containers. -

Read Our New Annual Report
The seeds of a concept. The roots of an idea. The potential of a world free of age-related disease. Photo: Sherry Loeser Photography SENS Research Foundation Board of Directors Barbara Logan, Chair Bill Liao, Secretary Kevin Perrott, Treasurer Michael Boocher Jonathan Cain Kevin Dewalt Michael Kope Jim O’Neill Frank Schüler Sherry Loeser Photography 2 Contents CEO Letter (Jim O’Neill) 4 Finances 5 Donors 6 - 7 Fundraising & Conferences 8 - 9 Around the World with Aubrey de Grey 10 Outreach 11 Founding CEO Tribute & Underdog Pharmaceuticals 12 - 13 Investments 14 Welcome New Team Members 15 Education 16 - 17 Publications & Research Advisory Board 18 Research Summaries 19 - 22 Ways to Donate 23 The SRF Team Front row: Anne Corwin (Engineer/Editor), Amutha Boominathan (MitoSENS Group Lead), Alexandra Stolzing (VP of Research), Aubrey de Grey (Chief Science Officer), Jim O’Neill (CEO), Bhavna Dixit (Research Associate). Center row: Caitlin Lewis (Research Associate), Lisa Fabiny-Kiser (VP of Operations), Gary Abramson (Graphics), Maria Entraigues-Abramson (Global Outreach Coordinator), Jessica Lubke (Administrative Assistant). Back row: Tesfahun Dessale Admasu (Research Fellow), Amit Sharma (ImmunoSENS Group Lead), Michael Rae (Science Writer), Kelly Protzman (Executive Assistant). Not Pictured: Greg Chin (Director, SRF Education), Ben Zealley (Website/Research Assistant/ Deputy Editor) Photo: Sherry Loeser Photography, 2019 3 From the CEO At our 2013 conference at Queens College, Cambridge, I closed my talk by saying, “We should not rest until we make aging an absurdity.” We are now in a very different place. After a lot of patient explanation, publication of scientific results, conferences, and time, our community persuaded enough scientists of the feasibility of the damage repair approach to move SENS and SENS Research Foundation from the fringes of scientific respectability to the vanguard of a mainstream community of scientists developing medical therapies to tackle human aging. -
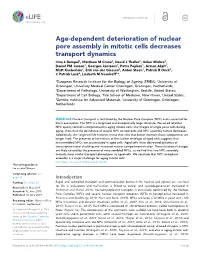
Age-Dependent Deterioration of Nuclear Pore Assembly in Mitotic
RESEARCH ARTICLE Age-dependent deterioration of nuclear pore assembly in mitotic cells decreases transport dynamics Irina L Rempel1, Matthew M Crane2, David J Thaller3, Ankur Mishra4, Daniel PM Jansen1, Georges Janssens1, Petra Popken1, Arman Aks¸it1, Matt Kaeberlein2, Erik van der Giessen4, Anton Steen1, Patrick R Onck4, C Patrick Lusk3, Liesbeth M Veenhoff1* 1European Research Institute for the Biology of Ageing (ERIBA), University of Groningen, University Medical Center Groningen, Groningen, Netherlands; 2Department of Pathology, University of Washington, Seattle, United States; 3Department of Cell Biology, Yale School of Medicine, New Haven, United States; 4Zernike Institute for Advanced Materials, University of Groningen, Groningen, Netherlands Abstract Nuclear transport is facilitated by the Nuclear Pore Complex (NPC) and is essential for life in eukaryotes. The NPC is a long-lived and exceptionally large structure. We asked whether NPC quality control is compromised in aging mitotic cells. Our images of single yeast cells during aging, show that the abundance of several NPC components and NPC assembly factors decreases. Additionally, the single-cell life histories reveal that cells that better maintain those components are longer lived. The presence of herniations at the nuclear envelope of aged cells suggests that misassembled NPCs are accumulated in aged cells. Aged cells show decreased dynamics of transcription factor shuttling and increased nuclear compartmentalization. These functional changes are likely caused by the presence -

Transhumanism, Metaphysics, and the Posthuman God
Journal of Medicine and Philosophy, 35: 700–720, 2010 doi:10.1093/jmp/jhq047 Advance Access publication on November 18, 2010 Transhumanism, Metaphysics, and the Posthuman God JEFFREY P. BISHOP* Saint Louis University, St. Louis, Missouri, USA *Address correspondence to: Jeffrey P. Bishop, MD, PhD, Albert Gnaegi Center for Health Care Ethics, Saint Louis University, 3545 Lafayette Avenure, Suite 527, St. Louis, MO 63104, USA. E-mail: [email protected] After describing Heidegger’s critique of metaphysics as ontotheol- ogy, I unpack the metaphysical assumptions of several transhu- manist philosophers. I claim that they deploy an ontology of power and that they also deploy a kind of theology, as Heidegger meant it. I also describe the way in which this metaphysics begets its own politics and ethics. In order to transcend the human condition, they must transgress the human. Keywords: Heidegger, metaphysics, ontology, ontotheology, technology, theology, transhumanism Everywhere we remain unfree and chained to technology, whether we passionately affirm or deny it. —Martin Heidegger I. INTRODUCTION Transhumanism is an intellectual and cultural movement, whose proponents declare themselves to be heirs of humanism and Enlightenment philosophy (Bostrom, 2005a, 203). Nick Bostrom defines transhumanism as: 1) The intellectual and cultural movement that affirms the possibility and desirability of fundamentally improving the human condition through applied reason, especially by developing and making widely available technologies to eliminate aging and to greatly enhance human intellectual, physical, and psychological capacities. 2) The study of the ramifications, promises, and potential dangers of technologies that will enable us to overcome fundamental human limitations, and the related study of the ethical matters involved in developing and using such technologies (Bostrom, 2003, 2). -

Dissecting Aging and Senescence—Current Concepts and Open Lessons
cells Review Dissecting Aging and Senescence—Current Concepts and Open Lessons 1,2, , 1,2, 1 1,2 Christian Schmeer * y , Alexandra Kretz y, Diane Wengerodt , Milan Stojiljkovic and Otto W. Witte 1,2 1 Hans-Berger Department of Neurology, Jena University Hospital, 07747 Jena, Thuringia, Germany; [email protected] (A.K.); [email protected] (D.W.); [email protected] (M.S.); [email protected] (O.W.W.) 2 Jena Center for Healthy Ageing, Jena University Hospital, 07747 Jena, Thuringia, Germany * Correspondence: [email protected] These authors have contributed equally. y Received: 2 October 2019; Accepted: 13 November 2019; Published: 15 November 2019 Abstract: In contrast to the programmed nature of development, it is still a matter of debate whether aging is an adaptive and regulated process, or merely a consequence arising from a stochastic accumulation of harmful events that culminate in a global state of reduced fitness, risk for disease acquisition, and death. Similarly unanswered are the questions of whether aging is reversible and can be turned into rejuvenation as well as how aging is distinguishable from and influenced by cellular senescence. With the discovery of beneficial aspects of cellular senescence and evidence of senescence being not limited to replicative cellular states, a redefinition of our comprehension of aging and senescence appears scientifically overdue. Here, we provide a factor-based comparison of current knowledge on aging and senescence, which we converge on four suggested concepts, thereby implementing the newly emerging cellular and molecular aspects of geroconversion and amitosenescence, and the signatures of a genetic state termed genosenium. -

Mechanisms and Rejuvenation Strategies for Aged Hematopoietic
Li et al. Journal of Hematology & Oncology (2020) 13:31 https://doi.org/10.1186/s13045-020-00864-8 REVIEW Open Access Mechanisms and rejuvenation strategies for aged hematopoietic stem cells Xia Li1,2,3†, Xiangjun Zeng1,2,3†, Yulin Xu1,2,3, Binsheng Wang1,2,3, Yanmin Zhao1,2,3, Xiaoyu Lai1,2,3, Pengxu Qian1,2,3 and He Huang1,2,3* Abstract Hematopoietic stem cell (HSC) aging, which is accompanied by reduced self-renewal ability, impaired homing, myeloid-biased differentiation, and other defects in hematopoietic reconstitution function, is a hot topic in stem cell research. Although the number of HSCs increases with age in both mice and humans, the increase cannot compensate for the defects of aged HSCs. Many studies have been performed from various perspectives to illustrate the potential mechanisms of HSC aging; however, the detailed molecular mechanisms remain unclear, blocking further exploration of aged HSC rejuvenation. To determine how aged HSC defects occur, we provide an overview of differences in the hallmarks, signaling pathways, and epigenetics of young and aged HSCs as well as of the bone marrow niche wherein HSCs reside. Notably, we summarize the very recent studies which dissect HSC aging at the single-cell level. Furthermore, we review the promising strategies for rejuvenating aged HSC functions. Considering that the incidence of many hematological malignancies is strongly associated with age, our HSC aging review delineates the association between functional changes and molecular mechanisms and may have significant clinical relevance. Keywords: Hematopoietic stem cells, Aging, Single-cell sequencing, Epigenetics, Rejuvenation Background in the clinic, donor age is carefully considered in HSC A key step in hematopoietic stem cell (HSC) aging re- transplantation, and young donors result in better sur- search was achieved in 1996, revealing that HSCs from vival after HSC transplantation [2–4]. -
Ÿþc R Y O N I C S M a G a Z I N E , Q 1 2 0
2007 RECAP 1st Quarter 2008 • Volume 29:1 2007 ANnual Review page 5 Member Profile: Wes Du Charme page 3 7th Alcor Conference Recap page 13 Cryonics and Religion: Friends or Foes? page 19 INSIDE CRYONICS 2 From the Editor 1ST QUARTER 2008 • VOLUME 29:1 19 Cryonics and Religion: Friends or Foes? The cryonics community recognizes the importance and challenge of being 1st Quarter 2008 • Volume 29:1 understood by the general 2007 RECAP public. Religion plays a sub- Cover shows opening reception stantial role in our diverse at the 7th Alcor conference. 2007 ANnual society and may seem to Review Photo by Brian Harris. page 5 some to be at odds with many facets of scientific COVER STORY: PAGE 5 advancement. Meet one theologian who feels the 2007 Annual Review: Today, over ultimate success of cryonics 850page people 3 in the world rely on the is contingent upon the sup- Member Profile: Wes Du CharmeAlcor Life Extension Foundation for Recap port of more than just great Conferencecryopreservation page 13 services. Enrich your 7th Alcor scientific minds. understanding of present-day clinical advancements with the potential to CryonicsFriends and Religion: or Foes?page 19 significantly benefit Alcor’s growing 22 Book Review: Ending membership base in years to come. Aging Likened to a good detective novel, Ending Aging allures the reader into a real- life tale of the mysteries of aging. The author, Dr. 3 Member Profile: Wes Du Charme Aubrey de Grey, has been Wes Du Charme – psychologist, author and barber shop quartet the center of controversy singer – celebrates his thirteenth year as an Alcor member in since proposing a systematic June 2008.