Common Lameness in the Cutting and Reining Horse
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reining & Working Cow Horse
UTAH SUMMER GAMES EQUESTRIAN – REINING & WORKING COW HORSE DATES: June 18, Saturday REGISTRATION FEE: $25.00 This is an annual registration fee per individual athlete. Ann additional sport fee will be added based on the sport participated in. SPORT FEE: $10.00 Fees payable to CCEC will be listed on the CCEC entry form SPORT COORDINATOR: Shelby Sorenson [email protected] Alexis Campbell [email protected] HOW TO REGISTER: Register online. If you are mailing in your registration form, send it to Utah Summer Games Registration, 351 West University Blvd, Cedar City, UT 84720. Use the Individual Registration Form. After completing your USG registration, please go to the following link to submit your CCEC class entries https://rwch.wufoo.com/forms/ccec-reining-working-cowhorse-show/ REGISTRATION DEADLINE: Final online registration is due by Thursday, June 16, at 10:00 AM. NO POST ENTRIES VENUE: Iron Ranger Arena – Cross Hollow Event Center 11 N Cross Hollow Drive Cedar City, UT SCHEDULES: CHECK-IN: Equestrian - Reining/Working Cow Athletes need to check in at the Cross Hollows Event Center on Saturday, June 20, between 7:00 AM and 8:30 AM. Each athlete will receive a welcome packet containing the official Utah Summer Games Athlete shirt and other assorted goodies. REINING & WORKING COW HORSE CLASSDESCRIPTIONS AND RULES Page | 1 UTAH SUMMER GAMES EQUESTRIAN – REINING & WORKING COW HORSE WORKING COW HORSE CLASSES Class # Name of Class Description 60 Green As Grass Riders 1st year in Working Cow Horse. May ride any age horse in any bridle (one handed in shank bit or two-hands with snaffle or hackamore). -

Double the Double
Digital Update Breaking News SUBSCRIBE NOW Peptoboonsmal to to Quarter Horse News Stand the 2010 Season and get the Nov. 1 issue • NRCHA Snaffle in Weatherford Bit Futurity Jackson Land and Cattle LLC • Christmas Gift Guide announced that Peptoboonsmal, • Brazos Bash one of the leading sires of perfor- mance horses, will stand the 2010 season at ESMS on the Brazos, a WEEK OF OCTOBER 12, 2009 QUARTERHORSENEWS.COM new facility in Weatherford, Texas. ESMS on the Brazos, Equine JReproduction Center & Fertility Lab, is the newest division of Equine Sports Medicine and ... Double the Read more at quarterhorsenews.com. Video See the Action Central Custom Cash Advance and Duane Latimer Watch Custom Cash Advance KIRKBRID and Duane Latimer’s Futurity Open finals winning run at the E Ariat Tulsa Reining Classic. Fun! PHO T im Blumer’s Double OG GET THE LATEST J Ranches, Maysville, RAP ONLINE NOW AT JOkla., and Moscow, HY Pa., had double the fun at The Tradition Reining Futurity, held Sept. 12 Jenna Blumer and Sweet Sugarpepto n GUNNATRASHYA / SHAWN at the Kentucky Horse Park, Lexington, Ky. FLARIDA WIN CONGRESS REINING FUTURITY Double J Ranches is home to Lenas Sugarman Sugars Lil Whiz is by West Coast Whiz Gunnatrashya (Colonels Smoking (Doc O’Lena x Sugar Gay Bar x Doc’s out of Sugarmans Belle; Sweet Sugarpepto is Gun x Natrasha x Trashadeous), rid- Sug) and Imasmartpepto (Peptoboonsmal x by Imasmartpepto out of Sweet Sugar Peppy. den by Shawn Flarida for Arcese Imasmartlittlesugar x Smart Little Lena). Both dams are by Lenas Sugarman. Both Quarter Horses, Weatherford, Texas, 3-year-olds were bred, raised and started at scored a 225.5 to win the Reining Lenas Sugarman started his career as a Futurity Open finals. -
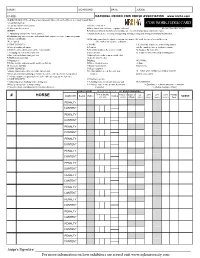
NRCHA Judge Cards 2019 Proposed.Xlsx
EVENT GO-ROUND DATE JUDGE CLASS NATIONAL REINED COW HORSE ASSOCIATION www.nrcha.com GUIDE FOR NEW COW: (At judges'discretion, rider will receive new cow(s) as necessary to show Horse) A- Cow that won't run COW WORK JUDGE CARD B- Cow that doesn't respect horse 5 POINT PENALTIES C- When cow leaves arena A-Not getting a turn each way (5 points each way) Effective November 16, 2018 CREDITS B-Spurring or hitting in front of cinch at anytime or excessively whipping or spurring the horse. A- Maintaining control of the cow at all times C-Blatant disobedience including kicking, biting, bucking, rearing and striking or obviously insubordinate B- Exhibiting superior cow sense and natural ability without excessive reining or spurring C- Degree of difficulity NOTE: Judge may blow the whistle at anytime to terminate the work. A score of zero will be given D- Eye Appeal if the work is not complete at that time. 1 POINT PENALTIES 0- SCORE L-If a rider hits or kicks the animal being worked A- Loss of working advantage A- Turn tail with the romal or reins, in an abusive manner C-Cow's head breaks the plane of the 1 point marker B- Using two hands on the reins in a bridle N- Improper Western Attire E-Changing sides of arena to turn cow or two rein class O - Failure to work in the proper working order L-For each length horse runs past cow C-Fingers between the reins in a bridle class P-Working out of position except the two rein class S-Slipping rein D-Balking NO SCORE: T-Failure to drive cow pass middle marker on first run E-Extremely out of control A-Abuse -
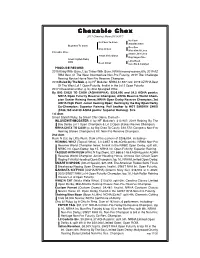
2020 Story Book Mares B01-B08
Chexable Chex 2011 Chestnut Mare (5418357) Nu Cash Nu Chex To Cash Amarilla Chex Big Chex To Cash One Gun Snip O Gun Miss Kim O Lena Chexable Chex Smart Little Lena Smart Chic Olena Gay Sugar Chic Smart Stylish Ruby 2006 Little Rush Rush N Cat Sure Be A Catalyst PRODUCE RECORD: 2015 Kinky With Guns, f. by Tinker With Guns. NRHA money-earner: 6th, 2019 AZ RHA Best Of The West Intermediate Non-Pro Futurity; 2019 The Challenge Reining Novice Horse Non-Pro Reserve Champion. 2016 Ruled By The Mob, g. by HF Mobster. NRHA $1,927: 3rd, 2019 AZ RHA Best Of The West Lvl 1 Open Futurity, finalist in the Lvl 2 Open Futurity. 2017 Chexsational Star, g. by Star Spangled Whiz. By BIG CHEX TO CASH (AQHA/APHA). $220,826 and 58.5 AQHA points: NRHA Open Futurity Reserve Champion; AQHA Reserve World Cham- pion Senior Reining Horse; NRHA Open Derby Reserve Champion; 3rd AQHA High Point Junior Reining Open; Reining by the Bay Open Derby Co-Champion; Superior Reining. Full brother to HOT SMOKIN CHEX ($188,160 and 90 AQHA points: Superior Reining). Sire 1st dam Smart Stylish Ruby, by Smart Chic Olena. Dam of-- INLOVEWITHMOBSTER (f. by HF Mobster). $13,907: 2019 Reining By The Bay Derby Lvl 1 Open Champion & Lvl 2 Open Stakes Resrve Champion. NRHA CHEX TO CASH (c. by Big Chex To Cash). $10,572: Congress Non-Pro Reining Stakes Champion & Int. Non-Pro Reserve Champion. 2nd dam Rush N Cat, by Little Rush. Dam of the earners of $206,054, including-- REINING WHIZ (Topsail Whiz). -

A≤HA Professional Horsewoman Carla Wennberg Shows You How To
Riding D RESSAGE A≤HA Professional Horsewoman Carla Wennberg shows you how to get started in the exciting sport of dressage. Plus, learn how the fundamentals of dressage can help you in other horse disciplines. By Andrea Caudill From the America’s Horse library americashorsedaily.com 1 americashorsedaily.com LESSON ONE: Enter at A IF I ASKED YOU IF YOU’D EVER RIDDEN DRESSAGE, WHAT WOULD I would love to see more American Quarter Horses trying dressage you say? Would you picture those giant Olympic warmbloods as an event, but because dressage is merely the methodic prancing in front of the judges, scoff, and say of course not training of an athletic, obedient horse, the exercises we will work – there’s no place for prancing on a cow horse! on can be used to improve any horse or any riding activity you What if I said that if you’ve ever sidepassed your horse up wish to pursue. to work a gate, if you’ve taught your horse to yield his hind- For example: Do you want your reiner, hunter or other quarters, if you’ve spent time perfecting your walk-trot performance horse to score more points with a soft, round, transitions for a flowing equitation pattern or keeping balanced circle? Would you rather your trail horse smoothly your reiner balanced in his rundowns, you’ve been doing canter off instead of making a jaw-rattling run into it? Can dressage? And if you’re having trouble with any of those you get your horse to trot a straight line and halt softly off things, or if you’ve had a desire to try riding competitive the seat, or does it more resemble a serpentine-shaped dressage, then this series is here to help. -
Section K Reining and Para-Reining
SECTION K REINING AND PARA-REINING Rules of Equestrian Canada 2021 CHANGES VISIBLE EDITION This document illustrates all changes following the final 2020 edition. Changes are noted with additions underlined in red ink; deletions presented by strikethrough text, also in red. EQUESTRIAN CANADA RULEBOOK SECTION K: REINING AND PARA-REINING The rules published herein are effective on January 1, 2020 2021 and remain in effect for one year except as superseded by rule changes or clarifications published in subsequent editions of this section. Section K as printed herein is the official version of Reining for 20202021. The Rule Book comprises the following sections: A General Regulations B Breeds C Driving and Para-Driving D Eventing E Dressage and Para-Dressage F General Performance, Western, Equitation G Hunter, Jumper, Equitation and Hack J Endurance K Reining and Para-Reining L Vaulting Section K: REINING AND PARA-REINING is part of the Rule Book of Equestrian Canada and is published by: Equestrian Canada 11 Hines Rd., Suite 201308 Legget Drive, Suite 100 Ottawa, Ontario K2K 2X1K2K 1Y6 Tel: (613) 287-1515; Fax: (613) 248-3484 1-866-282-8395 Email: [email protected] Web site: www.equestrian.ca © 2021 Equestrian Canada ISBN 978-1-77288-109-7 Reining Competition Chart Bronze Silver Gold Platinum Competition Operations Classes Open AAA, Open Open AAA, Open Grand Prix CRI AA, Open A, Open AA, Open A, Open Open AAA, Open Grand Prix Amateur AAA, Amateur AAA, AA, Open A, Open Open AAA, Amateur AA, Amateur AA, Amateur AAA, Amateur Amateur A, Amateur -
Fall Classic Patterns
PATTERN BOOK Arabian Fall Classic at The Oregon Horse Center October 2-4, 2020 Trail Horse C N / T P P 08 Arabian English Trail Horse .............................................................................English .........25 09 HA/AA English Trail Horse ...............................................................................English .........25 09.1 TBA024 Arabian English Trail Horse ATR (to run after class 9) ......................English .........25 10 Walk/Trot English Trail Horse 10 & Under ................................................... Walk/Trot .........24 11 Arabian Western Trail Horse JTR 18 & Under ............................................... Western .........26 12 HA/AA Western Trail Horse JTR 18 & Under ................................................ Western .........26 13 Arabian Western Trail Horse ......................................................................... Western .........26 14 HA/AA Western Trail Horse ........................................................................... Western .........26 15 Opportunity Trail ............................................................................................ Western .........26 16 Walk/Trot Western Trail Horse 10 & Under ................................................. Walk/Trot .........24 17 Arabian Western Trail Horse ATR* ................................................................ Western .........26 18 HA/AA Western Trail Horse ATR* .................................................................. Western .........26 19 Arabian -
OFFICIAL HANDBOOK of RULES and REGULATIONS 2020 | 68Th Edition
OFFICIAL HANDBOOK OF RULES AND REGULATIONS 2020 | 68th edition AMERICAN QUARTER HORSE An American Quarter Horse possesses acceptable pedigree, color and mark- ings, and has been issued a registration certificate by the American Quarter Horse Association. This horse has been bred and developed to have a kind and willing disposition, well-balanced conformation and agile speed. The American Quarter Horse is the world’s most versatile breed and is suited for a variety of purposes - from working cattle on ranches to international reining competition. There is an American Quarter Horse for every purpose. AQHA MISSION STATEMENT • To record and preserve the pedigrees of the American Quarter Horse, while maintaining the integrity of the breed and welfare of its horses. • To provide beneficial services for its members that enhance and encourage American Quarter Horse ownership and participation. • To develop diverse educational programs, material and curriculum that will position AQHA as the leading resource organization in the equine industry. • To generate growth of AQHA membership via the marketing, promo- tion, advertising and publicity of the American Quarter Horse. • To ensure the American Quarter Horse is treated humanely, with dignity, respect and compassion, at all times. FOREWORD The American Quarter Horse Association was organized in 1940 to collect, record and preserve the pedigrees of American Quarter Horses. AQHA also serves as an information center for its members and the general public on matters pertaining to shows, races and projects designed to improve the breed and aid the industry, including seeking beneficial legislation for its breeders and all horse owners. AQHA also works to promote horse owner- ship and to grow markets for American Quarter Horses. -

A Key to Abbreviations
Abbreviation in Database Translation 1/2YO 1 & 2 Year-Olds 1D, 2D, 3D, etc. 1st Division, 2nd Division, 3rd Division, etc. 1K, 2K, etc. $1,000, $2,000, etc. 1Y- 1-Year-Old & Under 2/3YO 2 & 3 Year-Olds 2/4YO 2 to 4 Year-Olds 2-HND Two-Hand 4/6YO 4 to 6 Year-Olds 5/6YO 5 & 6 Year-Olds 5Y- 5 & Under 5Y+ 5 & Over 5YO 5-Year-Old 6Y- 6 & Under 6Y+ 6-Year-Old & Over 6YO 6-Year-Old 7-UP 7 & Up (sometimes called "Uncola") A/A All-Age A/D All Divisions ABI Atlantic Breeders Incentive ADLT Adult ADVTG Advantage AFF Affiliate AGD Aged AGG Aggregate AICH NCHA of Italy AK Alaska AL Alabama AL-ARND All-Around AL-BRED Alabama Bred ALB Alberta ALL/AMER All-American AM Amateur AMELITE Elite Amateur AMER American AM-OWNER Amateur-Owner AM-TX Amateur of Texas AMPR Amateur Progeny Rewards (Breeders Halter Futurity) ANHA American Novice Horse Association ANYBODY/WIN Anybody Can Win ApCHA Appaloosa CHA ApCHAHF Appaloosa CHA Hall of Fame APHA American Paint Horse Association APHC Appaloosa Horse Club AQANZ AQHA of New Zealand AQHA American Quarter Horse Association AQHYA American Quarter Horse Youth Association AQQH Quebec Quarter Horse Association AR Arkansas ARAB Arabian ARG Argentina ARHFA American Rope Horse Futurity Association ARNHA American Ranch Horse Association AROAHA American Roan Horse Association ASHA American Stock Horse Association ASSN Association A-T All-Time ATL Atlantic AUG August AUP Australian Paint AUS Australia AUS N CHA Australia NCHA (cutting) AUSQHA Australia QHA (Quarter Horse Assoc.) AVG Average AWD Award AZ Arizona AZ-OWNED Arizona-Owned -
2020 Handbook-All Pages
REVISED 11/6/19 Foreword The National Reining Horse Association is a non-profit Organization dedicated to the promotion of the Reining Horse. The Association was formed in 1966 to encourage the showing of reining horses by providing worthwhile purses for which they can compete, by developing a standard method under which all reining contests can be conducted, and by acting as a forum for their breeders and trainers. In the fall of 1967 the Executive Committee of the National Reining Horse Association appointed its first Directors. A Rules Committee was chosen from these men. This booklet contains a revised version of the original ground rules and further changes will be adopted by the Board of Directors as deemed necessary. Deciding rule changes will not be difficult if our officers and Board of Directors remember the dedication and original intent of our founders. © The NRHA Handbook is the copyrighted property of the National Reining Horse Association. No person may use and/or reproduce this Handbook without the express written permission of the National Reining Horse Associ- ation. Shows seeking sanctioning and receiving approval from the Association are expressly authorized to use the information contained in this Handbook. FOR THE MOST CURRENT OFFICIAL VERSION OF THE HANDBOOK, VISIT OUR WEBSITE AT NRHA.COM. New rules and changes to rules are highlighted in gray. Sub- sequent updates will be noted in a different color. NRHA Bylaws, Corporate Record Book, policies, and other important references can be found in the Members Only section of nrha.com. 1 TABLE OF CONTENTS GENERAL RULES AND REGULATIONS A. -

Reined Cow Horse 2019 - 2020
REINED COW HORSE 2019 - 2020 General Rules: REINED COW HORSE will use NRCHA rules when not in conflict with NHSRA rules. Contestant may change horses in the Reined Cow Horse throughout the season. A Contestant may not change horses between the rein work and cow work portion of an event. 1. Reined Cow Horse must be offered at all State/Province Finals. States/Provinces will have two options in conducting their qualify Reined Cow Horses. a. Option I: Reined Cow Horse will be held at, or assigned to each qualifying rodeo. All points earned in the Reined Cow Horse will be applied to the All Around. b. Option II: The Reined Cow Horse will be offered at a minimum of three (3) times at the qualifying level. If option II is used, only points earned at State/Province and District Finals will be applied to the All Around. c. Choice of Option I or Option II must be approved by the State/Province Board of Directors prior to the rodeo season. The decision must be conveyed to state/province membership and the NHSRA office prior to start of rodeo season. 2. The State/Province may hold their Reined Cow Horse Finals prior to their State/Province Finals Rodeo. If they choose to do so, the Reined Cow Horse must be held within 60 days of the State/Province Finals Rodeo. a. All Reined Cow Horse must be approved on an activity sheet by the National Director and the National Executive Director. b. States/Provinces are encouraged to hold as many Reined Cow Horse events as possible. -
REINING RULES 5Th Edition, Effective 1St January 2016 Updates Effective 1St January 2021
REINING RULES 5th Edition, effective 1st January 2016 Updates effective 1st January 2021 Copyright © 2017 Fédération Equestre Internationale Reproduction strictly reserved Fédération Equestre Internationale HM King Hussein I Building t +41 21 310 47 47 Chemin de la Joliette 8 f +41 21 310 47 60 1006 Lausanne [email protected] Switzerland www.fei.org REINING RULES TABLE OF CONTENTS TABLE OF CONTENTS PREAMBLE 4 FEI CODE OF CONDUCT FOR THE WELFARE OF THE HORSE ............................................... 5 CHAPTER I GENERAL ........................................................................................................ 8 ARTICLE 300 INTERNATIONAL RULES ........................................................................... 8 CHAPTER II STRUCTURE OF COMPETITIONS .................................................................... 9 ARTICLE 301 COMPETITIONS ............................................................................................ 9 CHAPTER III ELIGIBILITY .............................................................................................. 11 ARTICLE 302 ATHLETE ............................................................................................... 11 ARTICLE 303 QUALIFICATIONS ......................................................................................... 11 ARTICLE 304 STAR LEVEL QUALIFICATION ......................................................................... 11 ARTICLE 305 FAST TRACK PROCEDURE ............................................................................. 12 ARTICLE