2017 Strategic Plan: Medicaid Behavioral Health Delivery & Payment System Reform
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
NBS 3Rd Quarter Report
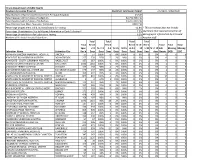
Illinois Department of Public Health Newborn Screening Program Specimen Submission Report 7/1/2018 - 9/30/2018 Total Number of Specimens Received from Perinatal Hospitals 43,345 Total Received within 3 Days of Collection 42,732 (98.6 %) Total Received within 5 Days of Collection 43,297 (99.9 %) Total Received 6 or More Days after Collection 24 (0.1%) Percentage of Specimens Valid and Satisfactory for Testing 92.8% * This percentage does not include Percentage Unsatisfactory Due to Missing Information or Early Collection* 7.0% specimens that required correction of Percentage Unsatisfactory for Laboratory Testing 0.2% demographic information by IDPH and Number of Perinatal Hospital Submitters 121 hospital staff. Total Total Total Total Total Rec'd Rec'd Rec'd % >5- Rec'd Total Total Total Spec. <=3 % <= 3 4-5 % 4-5 % 0-5 >5-14 14 >=14 % >= 14 Lab Missing Missing Submitter Name Submitter City Rec'd Days Days Days Days Days Days Days Days days Unsats DOB DOC ABRAHAM LINCOLN MEMORIAL HOSPITAL LINCOLN 57 57 100% 0 0% 100% 0 0% 0 0% 0 0 0 ADVENTIST BOLINGBROOK HOSPITAL BOLINGBROOK 257 250 97% 5 2% 99% 0 0% 0 0% 0 0 2 ADVOCATE - SOUTH SUBURBAN HOSPITAL HAZELCREST 167 167 100% 0 0% 100% 0 0% 0 0% 0 0 0 ADVOCATE CHRIST MEDICAL CENTER OAK LAWN 1592 1592 100% 0 0% 100% 0 0% 0 0% 2 0 0 ADVOCATE TRINITY HOSPITAL CHICAGO 162 158 98% 4 2% 100% 0 0% 0 0% 0 0 0 ALEXIAN BROS MEDICAL CENTER LAB ELK GROVE VILLAGE 570 557 98% 13 2% 100% 0 0% 0 0% 2 0 0 ALTON MEMORIAL HOSPITAL ALTON 199 197 99% 2 1% 100% 0 0% 0 0% 0 0 0 AMITA HEALTH ADVENTIST MEDICAL CENTER - HHINSDALE 805 801 100% 4 0% 100% 0 0% 0 0% 10 0 0 AMITA HEALTH ADVENTIST MEDICAL CENTER - LLA GRANGE 3 2 67% 1 33% 100% 0 0% 0 0% 0 0 0 AMITA HEALTH-ADVENTIST MEDICAL CENTER - GGLENDALE HEIGHTS 111 107 96% 4 4% 100% 0 0% 0 0% 1 0 0 ANDERSON HOSPITAL MARYVILLE 357 345 97% 12 3% 100% 0 0% 0 0% 0 0 0 ANN & ROBERT H. -

Hospital‐Reported Information on Diversity Expenditures on Capital Projects
Hospital‐Reported Information on Diversity Expenditures on Capital Projects On August 12, 2016, Public Act 99‐767 took effect, amending the Illinois Health Facilities Planning Act (20 ILCS 3960/5.3). Public Act 99‐767 added a provision for Illinois hospitals to report capital expenditures to female‐owned, minority‐owned, veteran‐owned and small business enterprises, and to provide information on hospital policies and activities related to promoting and realizing this diversity spending. The additional reporting requirement only effects hospitals having 100 or more service beds. Reporting is required from these hospitals beginning with their fiscal years starting on or after February 12, 2017. For the 2017 Annual Hospital Questionnaire, there were no hospitals meeting the statutory reporting requirements. However, we included a section for collecting diversity expenditure information in the 2017 questionnaire, requesting reporting on a voluntary basis. A copy of the 2017 Hospital Questionnaire is included in this report. The section on diversity expenditures is on pages 13 through 16 of the questionnaire. The information voluntarily provided by the hospitals which would have met the reporting requirements is presented in this report. Hospital ID 5496 Year 2017 Hospital Name Adventist Bolingbrook Hospital Bolingbrook Reporting Organization AMITA Health Contact Person David Evans / Katrina Scott Contact Telephone 847‐506‐6611 Contact Email [email protected] Facility Ownership Church‐Related Hospital Classification General Hospital Facility Fiscal Year Starting Date 7/1/2016 Ending Date 6/30/2017 Total Reported Capital Expenditures $1,854,999.00 Diversity Spending Goals and Actual Reported DIversity Spending Goals for Diversity Spending Actual Diversity Spending Female‐Owned Businesses 0 % 00% Minority‐Owned Businesses 0 % 0 0 % Veteran‐Owned Businesses 0 % 0 0 % Small Business Enterprises 0 % 0 0 % Facility Comments on Diversity Expenditures The state‐specific data cannot be provided due to the developing nature of this initiative. -
Needs of Specific Populations and Cost Strategies. with Unitedhealthcare, You Have Options
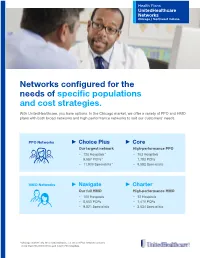
Health Plans UnitedHealthcare Networks Chicago / Northwest Indiana Networks configured for the needs of specific populations and cost strategies. With UnitedHealthcare, you have options. In the Chicago market, we offer a variety of PPO and HMO plans with both broad networks and high performance networks to suit our customers’ needs. PPO Networks ► Choice Plus ► Core Our largest network High-performance PPO − 120 Hospitals* − 103 Hospitals − 9,987 PCPs* − 7,783 PCPs − 11,900 Specialists* − 9,582 Specialists HMO Networks ► Navigate ► Charter Our full HMO High-performance HMO − 105 Hospitals − 12 Hospitals − 8,650 PCPs − 1,470 PCPs − 9,821 Specialists − 3,534 Specialists *Chicago market only. On a national basis, our Choice Plus network contains more than 783,000 doctors and over 5,700 hospitals. UnitedHealthcare Choice Plus With UnitedHealthcare Choice Plus, members choose from any health care professional in the network, including specialists, without a referral or selecting a primary care physician (PCP). Since Choice Plus is a network-based product, members can access care from any of nearly 800,000 network providers. There is coverage outside the Choice Plus network, but members can expect a lower benefit level. How we help members choose Additional services available to all the care that’s right for them. Choice Plus plan members. UnitedHealthcare helps deliver access to Virtual Visits. resources and personal support with our • Connect with a doctor for non-emergency care member website myuhc.com. Easy-to-use online, anytime. tools can help members: • Available 24/7 and takes about 20 minutes. • Find UnitedHealth Premium® doctors who Our Mobile App, Health4Me®. -
FY 2020 Proposed Rule Impact File.Xlsx
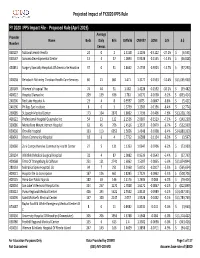
Projected Impact of FY2020 IPPS Rule FY 2020 IPPS Impact File ‐ Proposed Rule (April 2019) Average Provider Name Beds Daily Bills CMIV36 CMIV37 ∆CMI ∆ % ∆ $ Number Census 060107 National Jewish Health 24 0 2 1.5158 1.1036 ‐0.4122 ‐27.2%$ (6,595) 050547 Sonoma Developmental Center 13 4 37 1.0893 0.9338 ‐0.1555 ‐14.3% $ (46,028) 450831 Surgery Specialty Hospitals Of America Se Houston 37 0 31 2.8662 2.4739 ‐0.3923 ‐13.7%$ (97,290) 320038 Rehoboth Mckinley Christian Health Care Services 60 21 861 1.471 1.3177 ‐0.1533 ‐10.4%$ (1,055,930) 150149 Women's Hospital The 74 44 31 1.582 1.4228 ‐0.1592 ‐10.1%$ (39,482) 400022 Hospital Damas Inc 209 139 636 1.781 1.6172 ‐0.1638 ‐9.2%$ (833,414) 240206 Red Lake Hospital A 23 4 8 0.9597 0.875 ‐0.0847 ‐8.8%$ (5,421) 240196 Phillips Eye Institute 8 0 3 1.3739 1.2583 ‐0.1156 ‐8.4%$ (2,774) 260085 St Joseph Medical Center 173 104 2870 1.8602 1.7196 ‐0.1406 ‐7.6%$ (3,228,176) 400122 Professional Hospital Guaynabo Inc 54 13 122 2.1536 2.0007 ‐0.1529 ‐7.1%$ (149,230) 330086 Montefiore Mount Vernon Hospital 63 45 706 1.4516 1.3537 ‐0.0979 ‐6.7%$ (552,939) 050030 Oroville Hospital 133 113 6052 1.5656 1.4648 ‐0.1008 ‐6.4%$ (4,880,333) 460043 Orem Community Hospital 18 6 4 1.7712 1.6588 ‐0.1124 ‐6.3%$ (3,597) 320060 Zuni Comprehensive Community Health Center 27 5 131 1.1353 1.0647 ‐0.0706 ‐6.2%$ (73,989) 250134 Whitfield Medical Surgical Hospital 32 4 87 1.0082 0.9539 ‐0.0543 ‐5.4%$ (37,793) 420068 Trmc Of Orangeburg & Calhoun 251 121 2741 1.6062 1.5207 ‐0.0855 ‐5.3%$ (1,874,844) 280133 Nebraska Spine Hospital, -

Illinois Finance Authority Revenue Bonds, Series 2016C (Presence Health Network) (The “Bonds”)
SECOND SUPPLEMENT TO PRELIMINARY OFFICIAL STATEMENT $967,835,000* ILLINOIS FINANCE AUTHORITY REVENUE BONDS, SERIES 2016C (PRESENCE HEALTH NETWORK) (THE “BONDS”) The Preliminary Official Statement dated July 13, 2016 (the “Preliminary Official Statement”) relating to the above-referenced Bonds, as supplemented by the Supplement to Preliminary Official Statement dated July 15, 2016, is further supplemented and amended by this Second Supplement to Preliminary Official Statement dated July 26, 2016 (this “Supplement”), as follows: 1. As part of its Continuing Disclosure Agreement, the Corporation will host a call for the Beneficial Owners within seventy-five (75) days after the end of each fiscal quarter of the System through and including the fiscal quarter ending December 31, 2017. 2. The definition of “Cash and Liquid Investments” contained in Appendix D is hereby amended as follows (changed text shown in underline): “Cash and Liquid Investments” means all unrestricted cash and liquid investment balances, including, without limitation, such amounts that are on deposit in a funded depreciation fund or account, whether classified as current or noncurrent assets, held by the System Affiliates for any of their corporate purposes, but excluding any trustee held funds, creditor held funds, self insurance and captive insurance funds, pension and retirement funds and the proceeds of any short-term borrowings, including without limitation, draws on lines of credit regardless of the maturity date of the line of credit, all as set forth in the most recent Financial Statements of the System delivered under the Master Indenture. Capitalized terms in this Supplement have the meanings assigned thereto in the Preliminary Official Statement. -

FSN Healthcare Projects
QUALIFIED RELIABLE EXPERIENCED Featured Projects From Our Qualified Healthcare Contractors CALIFORNIA KANSAS San Francisco Kansas City California Pacific Medical Center University of Kansas Hospital Zuckerberg San Francisco General Hospital KENTUCKY COLORADO Paducah Colorado Springs Western Baptist Hospital Children’s Hospital Colorado Pikeville Denver Pikeville Medical Center Denver Health Medical Center MAINE Greeley Portland UCHealth Greeley Medical Center Maine Medical Center Lakewood MASSACHUSETTS Centura Health Lakewood Emergency & Urgent Care Boston CONNECTICUT Boston Children’s Hospital Greenwich Boston Medical Center Greenwich Hospital Brigham and Women’s Hospital Norwalk Brookline Norwalk Hospital Boston Children’s Hospital Stamford Burlington Stamford Hospital Lahey Medical Center HAWAII Salem Honolulu North Shore Medical Center Kaiser Permanente Hawaii Somerville Kapi’olani Medical Center for Women & Children Partners Healthcare St. Francis Healthcare System of Hawaii Waymouth The Queen’s Medical Center South Shore Hospital Tripler Army Medical Center MINNESOTA ILLINOIS Duluth Chicago Essentia Health-St. Mary’s Medical Center John H. Stroger Jr. Hospital Minneapolis Northwestern Memorial Hospital Fairview Health Services Rush University Medical Center Metropolitan Medical Center University of Chicago Medical Center Rochester Downers Grove Mayo Clinic Advocate Good Samaritan Hospital MISSOURI Elgin Kansas City Presence Health Belton Regional Medical Center Maywood Centerpoint Medical Center Loyola University Medical Center -

January 2015 Newsletter
First Illinois HFMA’s First Illinois Chapter Newsletter January 2015 Highlights and Recap First Illinois Chapter Events begin on page 21 News, Events & Updates In This Issue A Message from Joseph J. 1 A Message from Joseph J. Fifer, FHFMA, CPA Fifer, FHFMA, CPA HEALTHCARE FINANCIAL MANAGEMENT ASSOCIATION PRESIDENT AND CEO President’s Message 3 New Year’s Resolutions– 4 I’ve had a song stuck in my head for the past several effort, we established four new Affinity Groups, From HFMA Members to You days. And, as annoying as it can be to have Andy including payer health economics executives, Utilization of Healthcare 6 Williams on a continuous loop, I have to agree with academic medical center CFOs, physician practice Services Special Report him—this really is the most wonderful time of the administrators and value chief strategy officers. Medicare Physician Fee 10 year. From the festivities to the food to the family I am pleased to report that we continue to provide Schedule Announcement: gatherings, there are many reasons to love the holiday An Annual Tug of War? our members with much-needed best practices for season. It’s also a perfect time to take stock of the the ever-changing healthcare industry. This year, we Expanding the Provider Mix; 11 past year and to recognize those who’ve taken this added two new Value Project reports to encompass Transitioning the Use of APRNs journey with us. and Other Physician Extenders value-focused acquisitions and affiliations as well as Three Ways Healthcare 13 Looking back over the past 12 months, it’s clear that physician engagement and alignment. -

Provider Partners Chicago
Provider Partners Chicago Enjoy direct access to quality healthcare where you live. No Guesswork. Choose to see a carefully selected Imagine Health provider and receive affordable, quality care. No referrals. You have the simplicity of direct access to quality hospitals and physicians in your area. It’s that easy. Walk-in Care. You have access to all CVS MinuteClinic® locations nationwide, which provide a broad range of services to help keep you and your family healthy. Lab Services. Rely on Quest Diagnostics for all your lab-related diagnostic services. Peace of mind. When you use an Imagine Health provider, you won’t be billed for more than your patient responsibility. It makes good sense. Count on getting the most out of your plan when you see one of our partners in Chicago. For a current and complete list of Imagine providers in your area, visit hospitals + providers 22 8,100 providers.imaginehealth.com or download the mobile app. + urgent + ambulatory 70 cares 10 surgical centers Now it’s easier than ever before to get quality healthcare in Chicago. Provider Partners Include: AMITA Presence Health | Northwestern Medicine | Edward-Elmhurst Health Northwest Community Healthcare | Ann & Robert H. Lurie Childrens Hospital Hospitals 1. AMITA Health Mercy Medical Center Aurora 1325 N Highland Ave Aurora, IL 60506 2. AMITA Health Resurrection Medical Center Chicago 7435 W Talcott Ave Chicago, IL 60631 3. AMITA Health Saint Francis Hospital Evanston - Chicago 355 Ridge Ave Evanston, IL 60202 4. AMITA Health Saint Joseph Hospital - Chicago 2900 N Lake Shore Dr Chicago, IL 60657 5. AMITA Health Saint Joseph Hospital Elgin 77 N Airlite St Elgin, IL 60123 NOTE: Members also have access to ambulatory surgical centers, AMITA Health Saint Joseph 6. -

The World's Most Active Hospital & Healthcare
The USA's Most Active Hospital & Healthcare Professionals on Social - August 2021 Industry at a glance: Why should you care? So, where does your company rank? Position Company Name LinkedIn URL Location Employees on LinkedIn No. Employees Shared (Last 30 Days) % Shared (Last 30 Days) 1 symplr https://www.linkedin.com/company/symplr/United States 1,101 204 18.53% 2 Covenant Care https://www.linkedin.com/company/covenant-care-corp/United States 509 88 17.29% 3 Johnson & Johnson Consumer Health https://www.linkedin.com/company/johnson-johnson-consumer-health/United States 727 112 15.41% 4 Phreesia https://www.linkedin.com/company/phreesia/United States 1,201 185 15.40% 5 Labcorp Drug Development https://www.linkedin.com/company/labcorpdrugdev/United States 4,362 661 15.15% 6 BrightSpring Health Services https://www.linkedin.com/company/brightspringhealth/United States 17,110 2,500 14.61% 7 Teladoc Health https://www.linkedin.com/company/teladoc-health/United States 3,932 572 14.55% 8 Alto Pharmacy https://www.linkedin.com/company/altopharmacy/United States 749 104 13.89% 9 Quantum Health https://www.linkedin.com/company/quantum-health/United States 899 119 13.24% 10 Imprivata https://www.linkedin.com/company/imprivata/United States 612 78 12.75% 11 American College of Cardiology https://www.linkedin.com/company/american-college-of-cardiology/United States 771 97 12.58% 12 VillageMD https://www.linkedin.com/company/villagemd/United States 862 108 12.53% 13 Oak Street Health https://www.linkedin.com/company/oak-street-health/United States 1,692 211 12.47% 14 ECRI https://www.linkedin.com/company/ecri-org/United States 539 64 11.87% 15 Shields Health Solutions https://www.linkedin.com/company/shields-health-solutions/United States 603 70 11.61% 16 Amwell https://www.linkedin.com/company/amwellcorp/United States 1,104 125 11.32% 17 St. -

Community Health Needs Assessment
Community Health Needs Assessment Northwestern Medicine Huntley Hospital Northwestern Medicine McHenry Hospital Northwestern Medicine Woodstock Hospital Northwestern Medicine Community Health Needs Assessment Northwestern Medicine’s northwest region consists of the following hospitals: Northwestern Medicine Northwestern Medicine Northwestern Medicine Huntley Hospital McHenry Hospital Woodstock Hospital Northwestern Medicine Huntley Hospital, Northwestern Medicine McHenry Hospital, Northwestern Medicine Woodstock Hospital 2 2019 Community Health Needs Assessment Northwestern Medicine Table of contents Introduction . 4 Cancer About Northwestern Memorial HealthCare Respiratory Disease About Northwestern Medicine Huntley Hospital, Diabetes McHenry Hospital and Woodstock Hospital Reproductive Health Acknowledgements Risk Factors Impacting Health Outcomes The Community Health Needs Assessment . 9 Diet & Nutrition Background Physical Activity Goals Overweight and Obesity NM Medicine Huntley Hospital, McHenry Hospital Sexual Health and Woodstock Hospital Community Service Area Sexually Transmitted Diseases Methodology Access to Health Services & Primary Care Providers Primary Data Collection Oral Health Secondary Data Collection Interpreting and Prioritizing Health Needs . 36 Information Gaps Public Dissemination Additional Resources Available to Address Significant Health Needs . 38 Public Comment Prioritization Process of Health Needs . 39 Key Findings . 13 Community Description & Demographics Community Health Needs Assessment Social Determinants -

Mqii Stakeholders and Collaborators
MQii Stakeholders and Collaborators The Malnutrition Quality Improvement Initiative (MQii) is a project of the Academy of Nutrition and Dietetics, Avalere Health, and other stakeholders who provided guidance and expertise through a collaborative partnership. Support for the MQii is provided by Abbott. Special thanks to the members of the MQii Advisory Committee for their guidance in designing and informing the content of the Toolkit; to the members of the Technical Expert Panel for their guidance in specifying and testing the malnutrition electronic clinical quality measures (eCQMs); and to the members of the MQii Learning Collaborative for their work to implement the MQii Toolkit and eCQMs, and provide feedback to inform revisions and future iterations to MQii tools. MQii Advisory Committee Members Al Barrocas, MD, FACS, FASPEN Bob Blancato, MPA Owner of Alma, LLC President Fellow and Co-Chair of ASPEN’s Value Project Matz, Blancato and Associates (Former Chief Medical Officer of WellStar Atlanta (Former Chair of American Society on Aging, Director of Medical Center, Clinical Professor in the Surgery National Association of Nutrition and Aging Services Departments of LSU and Tulane Schools of Medicine) Programs, and board member for AARP) Member: 2020–Present Member: 2020–Present Charley John, PharmD Leslie Kelly-Hall Director of U.S. Public Policy Founder of Engaging Patient Strategy, Senior Vice Walgreens President of Policy Member of Government Affairs Committee at National Healthwise Association of Specialty Pharmacy Member: 2014–Present -

Compendium of US Health Systems, 2016, Technical Documentation-Appendix B
Comparative Health System Performance Initiative: Compendium of U.S. Health Systems, 2016, Technical Documentation Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services 5600 Fishers Lane Rockville, MD 20857 www.ahrq.gov Contract Number: HHSA290201600001C Prepared by: Mathematica Policy Research, Washington, DC Kirsten Barrett Ken Peckham David Jones Rachel Machta Jessica Heeringa Eugene Rich Laura Kimmey AHRQ Publication No. 17(19)-0047-EF September 2017 (updated January 2019) This page has been left blank for double-sided copying. COMPENDIUM OF U.S. HEALTH SYSTEMS Appendix B. Automated Matches Health HCOS health SK&A health SK&A health AHA health AHA health system ID HCOS health system name system address system name system address system name system address HSI00000002 AMG Integrated Healthcare 101 LA RUE AMG Integrated 101 LA RUE FRANCE, Management FRANCE, Healthcare Lafayette, LA, 70508- LAFAYETTE, LA, Management 3144 70508-3138 HSI00000005 Acadia Healthcare 830 CRES Acadia 830 CRESCENT CENTRE Healthcare CENTRE DR, Franklin, TN, Company, Inc. DRIVE, Franklin, TN, 37067-7323 37067-7323 HSI00000006 Acuityhealthcare, LP 10200 MALLARD AcuityHealthcare, 10200 MALLARD CREEK RD, LP CREEK CHARLOTTE, NC, ROAD, Charlotte, NC, 28262-9705 28262-9705 HSI00000008 Adena Health System 272 HOSPITAL RD, Adena Health System 272 HOSP RD, Adena Health 272 HOSPITAL ROAD, CHILLICOTHE, OH, Chillicothe, OH, System Chillicothe, OH, 45601-9031 45601-9031 45601-9031 HSI00000009 Adirondack Health 2233 STATE Adirondack