How Does It Feel to Be on Psilocybin? Dose-Response Relationships of Subjective Experiences in Humans
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hallucinogens - LSD, Peyote, Psilocybin, and PCP
Hallucinogens - LSD, Peyote, Psilocybin, and PCP Hallucinogenic compounds found in some • Psilocybin (4-phosphoryloxy-N,N- plants and mushrooms (or their extracts) dimethyltryptamine) is obtained from have been used—mostly during religious certain types of mushrooms that are rituals—for centuries. Almost all indigenous to tropical and subtropical hallucinogens contain nitrogen and are regions of South America, Mexico, and classified as alkaloids. Many hallucinogens the United States. These mushrooms have chemical structures similar to those of typically contain less than 0.5 percent natural neurotransmitters (e.g., psilocybin plus trace amounts of acetylcholine-, serotonin-, or catecholamine- psilocin, another hallucinogenic like). While the exact mechanisms by which substance. hallucinogens exert their effects remain • PCP (phencyclidine) was developed in unclear, research suggests that these drugs the 1950s as an intravenous anesthetic. work, at least partially, by temporarily Its use has since been discontinued due interfering with neurotransmitter action or to serious adverse effects. by binding to their receptor sites. This DrugFacts will discuss four common types of How Are Hallucinogens Abused? hallucinogens: The very same characteristics that led to • LSD (d-lysergic acid diethylamide) is the incorporation of hallucinogens into one of the most potent mood-changing ritualistic or spiritual traditions have also chemicals. It was discovered in 1938 led to their propagation as drugs of abuse. and is manufactured from lysergic acid, Importantly, and unlike most other drugs, which is found in ergot, a fungus that the effects of hallucinogens are highly grows on rye and other grains. variable and unreliable, producing different • Peyote is a small, spineless cactus in effects in different people at different times. -

The Varieties of Self-Transcendent Experience David Bryce Yaden, Jonathan Haidt, Ralph W
Review of General Psychology The Varieties of Self-Transcendent Experience David Bryce Yaden, Jonathan Haidt, Ralph W. Hood, Jr., David R. Vago, and Andrew B. Newberg Online First Publication, May 1, 2017. http://dx.doi.org/10.1037/gpr0000102 CITATION Yaden, D. B., Haidt, J., Hood, R. W., Jr., Vago, D. R., & Newberg, A. B. (2017, May 1). The Varieties of Self-Transcendent Experience. Review of General Psychology. Advance online publication. http://dx.doi.org/10.1037/gpr0000102 Review of General Psychology © 2017 American Psychological Association 2017, Vol. 0, No. 999, 000 1089-2680/17/$12.00 http://dx.doi.org/10.1037/gpr0000102 The Varieties of Self-Transcendent Experience David Bryce Yaden Jonathan Haidt University of Pennsylvania New York University Ralph W. Hood Jr. David R. Vago University of Tennessee at Chattanooga Harvard Medical School Andrew B. Newberg Thomas Jefferson University Various forms of self-loss have been described as aspects of mental illness (e.g., depersonalization disorder), but might self-loss also be related to mental health? In this integrative review and proposed organizational framework, we focus on self-transcendent experiences (STEs)—transient mental states marked by decreased self-salience and increased feelings of connectedness. We first identify common psychological constructs that contain a self-transcendent aspect, including mindfulness, flow, peak experiences, mystical-type experiences, and certain positive emotions (e.g., love, awe). We then propose psychological and neurobiological mechanisms that may mediate the effects of STEs based on a review of the extant literature from social psychology, clinical psychology, and affective neuroscience. We conclude with future directions for further empirical research on these experiences. -

Hallucinogens - LSD, Peyote, Psilocybin, and PCP
Information for Behavioral Health Providers in Primary Care Hallucinogens - LSD, Peyote, Psilocybin, and PCP What are Hallucinogens? Hallucinogenic compounds found in some plants and mushrooms (or their extracts) have been used— mostly during religious rituals—for centuries. Almost all hallucinogens contain nitrogen and are classified as alkaloids. Many hallucinogens have chemical structures similar to those of natural neurotransmitters (e.g., acetylcholine-, serotonin-, or catecholamine-like). While the exact mechanisms by which hallucinogens exert their effects remain unclear, research suggests that these drugs work, at least partially, by temporarily interfering with neurotransmitter action or by binding to their receptor sites. This InfoFacts will discuss four common types of hallucinogens: LSD (d-lysergic acid diethylamide) is one of the most potent mood-changing chemicals. It was discovered in 1938 and is manufactured from lysergic acid, which is found in ergot, a fungus that grows on rye and other grains. Peyote is a small, spineless cactus in which the principal active ingredient is mescaline. This plant has been used by natives in northern Mexico and the southwestern United States as a part of religious ceremonies. Mescaline can also be produced through chemical synthesis. Psilocybin (4-phosphoryloxy-N, N-dimethyltryptamine) is obtained from certain types of mushrooms that are indigenous to tropical and subtropical regions of South America, Mexico, and the United States. These mushrooms typically contain less than 0.5 percent psilocybin plus trace amounts of psilocin, another hallucinogenic substance. PCP (phencyclidine) was developed in the 1950s as an intravenous anesthetic. Its use has since been discontinued due to serious adverse effects. How Are Hallucinogens Abused? The very same characteristics that led to the incorporation of hallucinogens into ritualistic or spiritual traditions have also led to their propagation as drugs of abuse. -
How Should Therapists Respond to Client Accounts of Out-Of-Body Experience? Alexander De Foe Monash University
International Journal of Transpersonal Studies Volume 31 | Issue 1 Article 10 1-1-2012 How Should Therapists Respond to Client Accounts of Out-of-Body Experience? Alexander De Foe Monash University Follow this and additional works at: https://digitalcommons.ciis.edu/ijts-transpersonalstudies Part of the Philosophy Commons, Psychology Commons, and the Religion Commons Recommended Citation De Foe, A. (2012). De Foe, A. (2012). How should therapists respond to client accounts of out-of-body experience? International Journal of Transpersonal Studies, 31(1), 75–82.. International Journal of Transpersonal Studies, 31 (1). http://dx.doi.org/10.24972/ ijts.2012.31.1.75 This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 4.0 License. This Special Topic Article is brought to you for free and open access by the Journals and Newsletters at Digital Commons @ CIIS. It has been accepted for inclusion in International Journal of Transpersonal Studies by an authorized administrator of Digital Commons @ CIIS. For more information, please contact [email protected]. How Should Therapists Respond to Client Accounts of Out-of-Body Experience? Alexander De Foe Monash University Melbourne, Australia During an out-of-body experience (OBE) a person experiences their center of consciousness from a spatial location that is distinctly different to their physical body. Prior research has suggested that psychologists and psychotherapists may be reluctant to discuss the content of their clients OBE accounts due to a lack of understanding about the nature of these experiences. Yet, other research has highlighted the substantial value of discussing OBEs in the therapeutic process. -

From Sacred Plants to Psychotherapy
From Sacred Plants to Psychotherapy: The History and Re-Emergence of Psychedelics in Medicine By Dr. Ben Sessa ‘The rejection of any source of evidence is always treason to that ultimate rationalism which urges forward science and philosophy alike’ - Alfred North Whitehead Introduction: What exactly is it that fascinates people about the psychedelic drugs? And how can we best define them? 1. Most psychiatrists will define psychedelics as those drugs that cause an acute confusional state. They bring about profound alterations in consciousness and may induce perceptual distortions as part of an organic psychosis. 2. Another definition for these substances may come from the cross-cultural dimension. In this context psychedelic drugs may be recognised as ceremonial religious tools, used by some non-Western cultures in order to communicate with the spiritual world. 3. For many lay people the psychedelic drugs are little more than illegal and dangerous drugs of abuse – addictive compounds, not to be distinguished from cocaine and heroin, which are only understood to be destructive - the cause of an individual, if not society’s, destruction. 4. But two final definitions for psychedelic drugs – and those that I would like the reader to have considered by the end of this article – is that the class of drugs defined as psychedelic, can be: a) Useful and safe medical treatments. Tools that as adjuncts to psychotherapy can be used to alleviate the symptoms and course of many mental illnesses, and 1 b) Vital research tools with which to better our understanding of the brain and the nature of consciousness. Classifying psychedelic drugs: 1,2 The drugs that are often described as the ‘classical’ psychedelics include LSD-25 (Lysergic Diethylamide), Mescaline (3,4,5- trimethoxyphenylathylamine), Psilocybin (4-hydroxy-N,N-dimethyltryptamine) and DMT (dimethyltryptamine). -

Evaluation of the Evidence for the Trauma and Fantasy Models of Dissociation
Psychological Bulletin © 2012 American Psychological Association 2012, Vol. 138, No. 3, 550–588 0033-2909/12/$12.00 DOI: 10.1037/a0027447 Evaluation of the Evidence for the Trauma and Fantasy Models of Dissociation Constance J. Dalenberg Bethany L. Brand California School of Professional Psychology at Alliant Towson University International University, San Diego David H. Gleaves and Martin J. Dorahy Richard J. Loewenstein University of Canterbury Sheppard Pratt Health System, Baltimore, Maryland, and University of Maryland School of Medicine, Baltimore Etzel Carden˜a Paul A. Frewen Lund University University of Western Ontario Eve B. Carlson David Spiegel National Center for Posttraumatic Stress Disorder, Menlo Park, Stanford University School of Medicine and Veterans Administration Palo Alto Health Care System, Palo Alto, California The relationship between a reported history of trauma and dissociative symptoms has been explained in 2 conflicting ways. Pathological dissociation has been conceptualized as a response to antecedent traumatic stress and/or severe psychological adversity. Others have proposed that dissociation makes individuals prone to fantasy, thereby engendering confabulated memories of trauma. We examine data related to a series of 8 contrasting predictions based on the trauma model and the fantasy model of dissociation. In keeping with the trauma model, the relationship between trauma and dissociation was consistent and moderate in strength, and remained significant when objective measures of trauma were used. Dissociation was temporally related to trauma and trauma treatment, and was predictive of trauma history when fantasy proneness was controlled. Dissociation was not reliably associated with suggestibility, nor was there evidence for the fantasy model prediction of greater inaccuracy of recovered memory. -

Psilocybin Mushrooms Fact Sheet
Psilocybin Mushrooms Fact Sheet January 2017 What are psilocybin, or “magic,” mushrooms? For the next two decades thousands of doses of psilocybin were administered in clinical experiments. Psilocybin is the main ingredient found in several types Psychiatrists, scientists and mental health of psychoactive mushrooms, making it perhaps the professionals considered psychedelics like psilocybin i best-known naturally-occurring psychedelic drug. to be promising treatments as an aid to therapy for a Although psilocybin is considered active at doses broad range of psychiatric diagnoses, including around 3-4 mg, a common dose used in clinical alcoholism, schizophrenia, autism spectrum disorders, ii,iii,iv research settings ranges from 14-30 mg. Its obsessive-compulsive disorder, and depression.xiii effects on the brain are attributed to its active Many more people were also introduced to psilocybin metabolite, psilocin. Psilocybin is most commonly mushrooms and other psychedelics as part of various found in wild or homegrown mushrooms and sold religious or spiritual practices, for mental and either fresh or dried. The most popular species of emotional exploration, or to enhance wellness and psilocybin mushrooms is Psilocybe cubensis, which is creativity.xiv usually taken orally either by eating dried caps and stems or steeped in hot water and drunk as a tea, with Despite this long history and ongoing research into its v a common dose around 1-2.5 grams. therapeutic and medical benefits,xv since 1970 psilocybin and psilocin have been listed in Schedule I of the Controlled Substances Act, the most heavily Scientists and mental health professionals criminalized category for drugs considered to have a consider psychedelics like psilocybin to be “high potential for abuse” and no currently accepted promising treatments as an aid to therapy for a medical use – though when it comes to psilocybin broad range of psychiatric diagnoses. -

PSYCHEDELIC DRUGS (P.L) 1. Terminology “Hallucinogens
PSYCHEDELIC DRUGS (p.l) 1. Terminology “hallucinogens” – induce hallucinations, although sensory distortions are more common “psychotomimetics” – to minic psychotic states, although truly most drugs in this class do not do so “phantasticums”or “psychedelics” – alter sensory perception (Julien uses “psychedelics”) alterations in perception, cognition, and mood, in presence of otherwise clear ability to sense” may increase sensory awareness, increase clarity, decrease control over what is sensed/experienced “self-A” may feel a passive observer of what “self-B” is experiencing often accompanied by a sense of profound meaningfulness, of divine or cosmic importance (limbic system?) these drugs can be classified by what NT they mimic: anti-ACh, agonists for NE, 5HT, or glutamate (See p. 332, Table 12.l in Julien, 9th Ed.) 2. The Anti-ACh Psychedelics e.g. scopolamine (classified as an ACh blocker) high affinity, no efficacy plant product: Belladonna or “deadly nightshade” (Atropa belladonna) Datura stramonium (jimson weed, stinkweed) Mandragora officinarum (mandrake plant) pupillary dilation (2nd to atropine) PSYCHEDELIC DRUGS (p.2) 2. Anti-ACh Psychedelics (cont.) pharmacological effects: e.g. scopolamine (Donnatal) clinically used to tx motion sickness, relax smooth muscles (gastric cramping), mild sedation/anesthetic effect PNS effects --- dry mouth relaxation of smooth muscles decreased sweating increased body temperature blurred vision dry skin pupillary dilation tachycardia, increased BP CNS effects --- drowsiness, mild euphoria profound amnesia fatigue decreased attention, focus delirium, mental confusion decreased REM sleep no increase in sensory awareness as dose increases --- restlessness, excitement, hallucinations, euphoria, disorientation at toxic dose levels --- “psychotic delirium”, confusion, stupor, coma, respiratory depression so drug is really an intoxicant, amnestic, and deliriant 3. -

CLINICAL STUDY PROTOCOL Psilocybin-Assisted Psychotherapy
CLINICAL STUDY PROTOCOL Psilocybin-assisted Psychotherapy in the Management of Anxiety Associated With Stage IV Melanoma. Version: Final IND: [79,321] SPONSOR Multidisciplinary Association for Psychedelic PRINCIPAL INVESTIGATOR Sameet Kumar Ph.D. MEDICAL MONITOR Michael C. Mithoefer MD. STUDY PERSONNEL XXXXXXXXXXXXX XXXXXXXXXXXXX XXXXXXXXXXXXX STUDY MONITOR [CRA] Valerie Mojeiko IRB Study Site IRB Sponsor Signatory Rick Doblin Ph.D. Study Period 2008 For trial related emergencies please contact: Dr. Michael Mithoefer MAPS: S Kumar PI Clinical Study Protocol PCA1 Final December 1, 2007 Confidential Page 2 of 83 Table of Contents Introduction......................................................................................................................... 4 Background..................................................................................................................... 4 Disease History and Related Research ........................................................................... 5 Rationale ......................................................................................................................... 7 Summary......................................................................................................................... 7 Ethics................................................................................................................................... 8 Informed Consent of Subject .......................................................................................... 9 Recruitment and Screening............................................................................................ -
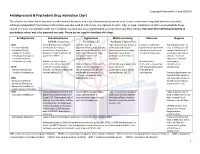
Antidepressant & Psychedelic Drug Interaction Chart
Copyright Psychedelic School 8/2020 Antidepressant & Psychedelic Drug Interaction Chart This chart is not intended to be used to make medical decisions and is for informational purposes only. It was constructed using data whenever possible, although extrapolation from known information was also used to inform risk. Any decision to start, stop, or taper medication and/or use psychedelic drugs should be made in conjunction with your healthcare provider(s). It is recommended to not perform any illicit activity. This chart the intellectual property of psychedelic school and is for personal use only. Please do not copy or distribute this chart. Antidepressant Phenethylamines Tryptamines MAOI-containing Ketamine Ibogaine -MDMA, mescaline -Psilocybin, LSD -Ayahuasca, Syrian Rue SSRIs Taper & discontinue at least 2 Consider taper & Taper & discontinue at least 2 Has been studied and Taper & discontinue at · Paroxetine (Paxil) weeks prior (all except discontinuation at least 2 weeks weeks prior (all except found effective both with least 2 weeks prior (all · Sertraline (Zoloft) fluoxetine) or 6 weeks prior prior (all except fluoxetine) or 6 fluoxetine) or 6 weeks prior and without concurrent except fluoxetine) or 6 · Citalopram (Celexa) (fluoxetine only) due to loss of weeks prior (fluoxetine only) (fluoxetine only) due to use of antidepressants weeks prior (fluoxetine · Escitalopram (Lexapro) psychedelic effect due to potential loss of potential risk of serotonin only) due to risk of · Fluxoetine (Prozac) psychedelic effect syndrome additive QTc interval · Fluvoxamine (Luvox) MDMA is unable to cause Recommended prolongation, release of serotonin when the Chronic antidepressant use may Life threatening toxicities can to be used in conjunction arrhythmias, or SPARI serotonin reuptake pump is result in down-regulation of occur with these with oral antidepressants cardiotoxicity · Vibryyd (Vilazodone) blocked. -

Ce4less.Com Ce4less.Com Ce4less.Com Ce4less.Com Ce4less.Com Ce4less.Com Ce4less.Com
Hallucinogens And Dissociative Drug Use And Addiction Introduction Hallucinogens are a diverse group of drugs that cause alterations in perception, thought, or mood. This heterogeneous group has compounds with different chemical structures, different mechanisms of action, and different adverse effects. Despite their description, most hallucinogens do not consistently cause hallucinations. The drugs are more likely to cause changes in mood or in thought than actual hallucinations. Hallucinogenic substances that form naturally have been used worldwide for millennia to induce altered states for religious or spiritual purposes. While these practices still exist, the more common use of hallucinogens today involves the recreational use of synthetic hallucinogens. Hallucinogen And Dissociative Drug Toxicity Hallucinogens comprise a collection of compounds that are used to induce hallucinations or alterations of consciousness. Hallucinogens are drugs that cause alteration of visual, auditory, or tactile perceptions; they are also referred to as a class of drugs that cause alteration of thought and emotion. Hallucinogens disrupt a person’s ability to think and communicate effectively. Hallucinations are defined as false sensations that have no basis in reality: The sensory experience is not actually there. The term “hallucinogen” is slightly misleading because hallucinogens do not consistently cause hallucinations. 1 ce4less.com ce4less.com ce4less.com ce4less.com ce4less.com ce4less.com ce4less.com How hallucinogens cause alterations in a person’s sensory experience is not entirely understood. Hallucinogens work, at least in part, by disrupting communication between neurotransmitter systems throughout the body including those that regulate sleep, hunger, sexual behavior and muscle control. Patients under the influence of hallucinogens may show a wide range of unusual and often sudden, volatile behaviors with the potential to rapidly fluctuate from a relaxed, euphoric state to one of extreme agitation and aggression. -

The Use of Psychedelic Drugs in the Treatment of Problematic Drug and Alcohol Use
Tripping up addiction: The use of psychedelic drugs in the treatment of problematic drug and alcohol use Short Title: Illicit drugs in the treatment of addiction Celia Morgan 1,3, Amy McAndrew1, Tobias Stevens1, David Nutt2, Will Lawn1,3 1. Psychopharmacology and Addiction Research Centre, University of Exeter, UK 2. Centre for Neuropsychopharmacology, Imperial College London, UK 3. Clinical Psychopharmacology Unit, University College London, UK Address Corrrespondence to: Celia Morgan Psychopharmacology and Addiction Research Centre Washington Singer Laboratory University of Exeter Perry Road, Exeter Devon UK EX4 4QG Key words: addiction, psychedelics, ketamine, ibogaine, ayahuasca, LSD , psilocybin, neurogenesis, 1 Highlights: Psilocybin may reduce alcohol and tobacco use in addicted samples. Ibogaine and ayahuasca have shown promise in the treatment of various addictions through observational studies. Ketamine has been used to treat alcohol dependence and reduces cocaine self- administration in the human laboratory. Randomised controlled trials are greatly needed to further test the efficacy of all of these compounds. Psychedelic drugs may have their therapeutic qualities due to anti-depressant effects, stimulating neuroplasticity and long-term psychological changes. 2 Abstract Psychedelic drugs have been used as treatments in indigenous cultures for thousands of years. Yet, due to their legal status, there has been limited scientific research into the therapeutic potential of these compounds for psychiatric disorders. In the absence of other effective treatments however, researchers have begun again to systematically investigate such compounds and there is now evidence pointing to the use of psychedelic drugs in the treatment of addiction. In this review we focus on human evidence for the effectiveness of preparations used by indigenous cultures in the Amazon (ayahausca) and Africa (ibogaine) and worldwide (psilocybin), and more recently synthetised drugs such as the serotonergic hallucinogen LSD and the dissociative anaesthetic ketamine.