Pediatric and Adolescent Skin Issues Disclosure • No Real Or Potential
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
CLAPA Adults Conference
Adults Cleft Conference Camden Lock, London, England Saturday 17 November 2018 The Cleft Lip and Palate Association (CLAPA) is the only national charity supporting people and families affected by cleft lip and/or palate in the UK from diagnosis through to adulthood. Timetable • • • • • • • • • • • • • • • • What’s today all about? • • • • Some ground rules and caveats • • • • • About the Adult Services Project • There are an estimated 75,000 people over the age of 16 living in the United Kingdom who were born with a cleft. • Understanding and supporting the unique needs and experiences of adults affected by cleft is very important to CLAPA. • From March 2018-February 2021, CLAPA is undertaking an exciting project looking at improving services for adults who were born with a cleft funded by the VTCT Foundation. • The goals are to research and understand the experiences, challenges and unmet needs of adults in the UK who were born with a cleft lip and/or palate. • The Adult Services Coordinator is the primary contact for this piece of work. What we did in Year One • • • • • So…what did we find at the roadshow? • We were humbled by how candidly people shared some of their most pivotal moments with us. • As you would expect, there were many different (oftentimes unique) experiences in the community, however there were some common themes that came up many times – these included: • The struggle of obtaining a successful referral to the cleft team as an adult • Being unsure what to expect at cleft team appointments • Not knowing (and health -

Familial Hyperinsulinism Due to HNF4A Deficiency and Benign Premature Adrenarche: a Case Report
Case Report Familial Hyperinsulinism due to HNF4A Deficiency and Benign Premature Adrenarche: A Case Report Edward Compton,1 David H. Geller,2 Alaina P. Vidmar MD.3 Abstract Background: Familial Hyperinsulinism due to HNF4A deficiency (FHI-HNF4A) is a form of diazoxide-sensitive, diffuse hyperinsulinism, characterized by transient or persistent hyperinsulinemic hypoglycemia, and a propensity to develop Maturity-Onset Diabetes of the Young type 1 (MODY1). The association between FHI-HNF4A deficiency and benign premature adrenarche (BPA) is unknown. The Case: We report the case of a 5-year-old girl with FHI-HNF4A, controlled on diazoxide, who presented with BPA and Tanner stage 3 pubic hair associated with body odor and acne. Work-up revealed elevated dehydroepiandrosterone sulfate (DHEAS), elevated free testosterone, and advanced bone age. Insulin levels were elevated in the setting of normal fasting blood glucose. We discuss the possible hormonal underpinnings of hyperandrogenism. Conclusion: Though the underlying pathophysiology of this phenotype is unclear, a possible synergistic mechanism exists between insulin-induced hyperandrogenism and HNF4A deficiency leading to a transient decrease of SHBG and thus increased free testosterone levels. Further investigation is required to determine the association between HNF4A dysfunction and BPA. Key Words: Hyperinsulinism; Congenital Hyperinsulinism; Adrenarche; HNF4A; Hyperandrogenism (Source: MeSH-NLM). Introduction Congenital hyperinsulinism (CHI) is due to a variety of etiologies that Highlights: result in dysregulated insulin release from pancreatic β-cells. There are Familial Hyperinsulinism due to HNF4A deficiency (FHI-HNF4A) is a two histological variants of CHI, focal and diffuse, which differ in the form of diazoxide-sensitive; diffuse hyperinsulinism, characterized by extent of pancreatic involvement. -

Oral Lichen Planus: a Case Report and Review of Literature
Journal of the American Osteopathic College of Dermatology Volume 10, Number 1 SPONSORS: ',/"!,0!4(/,/'9,!"/2!4/29s-%$)#)3 March 2008 34)%&%,,!"/2!4/2)%3s#/,,!'%.%8 www.aocd.org Journal of the American Osteopathic College of Dermatology 2007-2008 Officers President: Jay Gottlieb, DO President Elect: Donald Tillman, DO Journal of the First Vice President: Marc Epstein, DO Second Vice President: Leslie Kramer, DO Third Vice President: Bradley Glick, DO American Secretary-Treasurer: Jere Mammino, DO (2007-2010) Immediate Past President: Bill Way, DO Trustees: James Towry, DO (2006-2008) Osteopathic Mark Kuriata, DO (2007-2010) Karen Neubauer, DO (2006-2008) College of David Grice, DO (2007-2010) Dermatology Sponsors: Global Pathology Laboratory Stiefel Laboratories Editors +BZ4(PUUMJFC %0 '0$00 Medicis 4UBOMFZ&4LPQJU %0 '"0$% CollaGenex +BNFT2%FM3PTTP %0 '"0$% Editorial Review Board 3POBME.JMMFS %0 JAOCD &VHFOF$POUF %0 Founding Sponsor &WBOHFMPT1PVMPT .% A0$%t&*MMJOPJTt,JSLTWJMMF .0 4UFQIFO1VSDFMM %0 t'"9 %BSSFM3JHFM .% wwwBPDEPSg 3PCFSU4DIXBS[F %0 COPYRIGHT AND PERMISSION: written permission must "OESFX)BOMZ .% be obtained from the Journal of the American Osteopathic College of Dermatology for copying or reprinting text of .JDIBFM4DPUU %0 more than half page, tables or figurFT Permissions are $JOEZ)PGGNBO %0 normally granted contingent upon similar permission from $IBSMFT)VHIFT %0 the author(s), inclusion of acknowledgement of the original source, and a payment of per page, table or figure of #JMM8BZ %0 reproduced matFSJBMPermission fees -

Expanding Phenotype of Hereditary Fibrosing Poikiloderma with Tendon
CASE SERIES Expanding phenotype of hereditary fibrosing poikiloderma with tendon contractures, myopathy, and pulmonary fibrosis caused by FAM111B mutations: Report of an additional family raising the question of cancer predisposition and a short review of early-onset poikiloderma Rapha€elle Goussot, MD,a Megana Prasad, MD,b Corinne Stoetzel, MD,b Cedric Lenormand, MD, PhD,a Helene Dollfus, MD, PhD,b and Dan Lipsker, MD, PhDa Strasbourg, France Key words: FAM111B; inherited poikiloderma; pancreatic cancer. ereditary fibrosing poikiloderma with Abbreviations used: tendon contractures, myopathy, and pul- monary fibrosis (POIKTMP [MIM#615704]) IPMN: intraductal papillary mucinous H neoplasm is an extremely rare syndromic form of autosomal POIKTMP: hereditary fibrosing poikiloderma dominant poikiloderma. This genetic disorder was with tendon contractures, myopathy, first identified in a South African family in 2006.1 To and pulmonary fibrosis date, 3 families and 9 independent sporadic cases RTS: Rothmund-Thomson syndrome have been reported.2-4 Here we report an additional family of POIKTMP and expand the clinical spec- trum. We describe, for the first time to our knowl- early childhood. Clinical evaluation found a very edge, a pancreatic cancer in the clinical course in 1 severe case of poikiloderma, predominant in the patient. We also address the differential diagnosis of sun-exposed areas, resulting from the combination inherited poikiloderma and related disorders. of skin atrophy, mottled pigmentation with hyper- pigmented and hypopigmented lesions, and telan- CASE SERIES giectasia (Fig 1, A). He had a distinct intolerance for In 2007, at the Strasbourg University Hospital, the heat with marked hypohidrosis. Diffuse xerosis was department of medical genetics referred a family to combined with multiple depigmented macules on the dermatology department with a diverse clinical the trunk and limbs. -

Reticulate Hyperpigmentation of the Skin After Topical Application Of
Letters to the Editor 301 Reticulate Hyperpigmentation of the Skin After Topical Application of Benzoyl Peroxide Sir, Our two patients appeared to develop an irritant response on Benzoyl peroxide (BP) is an e¡ective and frequently used topical thetrunk afterapplication of 5% benzoyl peroxide. One medication for the treatment of acne vulgaris. It is a strong, patient applied BP to his face withnoirritation,consistentwith broad spectrum bactericidal agent that signi¢cantly decreases the ¢ndings of Hausteinetal.(3). Both patients then developed the number of Propionibacterium acnes in both the follicle and apattern of reticulate hyperpigmentation after their initial der- on surface skin (1). A common side e¡ect after usage is irritation matitis subsided. Biopsy in both cases was consistent with of the skin, usually manifested as a stinging or burning, and postin£ammatory hyperpigmentation. sometimes accompanied by erythema and scaling. Benzoyl per- Postin£ammatory hyperpigmentation develops after acute oxide is a strong irritant, but a weak allergen, rarely causing a or chronic in£ammation and trauma to the skin. The intensity contact dermatitis (2, 3). Tolerance can be achieved by gradually of the hypermelanosistendstobe more pronounced in darker- increasing the frequency of application over time. We describe skinnedindividuals. Other conditions that produce a pattern of two cases in which topical application of benzoyl peroxide reticulate hyperpigmentation include Riehl's melanosis, resulted in an unusual pattern of reticulate hyperpigmentation which is characterized by reticulate brown-black pigmenta- of the skin, most likely as a sequela of an irritant contact derma- tion of the face and neck. This is thought to be a result of a titis. -

Pattern of Skin Diseases at University of Benin Teaching Hospital, Benin City, Edo State, South-South Nigeria: a 12 Month Prospective Study
www.ccsenet.org/gjhs Global Journal of Health Science Vol. 4, No. 3; 2012 Pattern of Skin Diseases at University of Benin Teaching Hospital, Benin City, Edo State, South-South Nigeria: A 12 Month Prospective Study B. A. Ukonu1 & E. U. Eze2 1 University of Abuja Teaching Hospital, Gwagwalada, Abuja, Nigeria 2 University of Benin Teaching Hospital, Benin City, Edo State, Nigeria Correspondence: Ukonu, Agwu Bob (MBBS, FMCP), University of Abuja Teaching Hospital, Gwagwalada, Abuja, Nigeria. Tel: 234-805-791-5902, 234-702-675-1965. E-mail: [email protected] Received: January 4, 2012 Accepted: January 15, 2012 Online Published: May 1, 2012 doi:10.5539/gjhs.v4n3p148 URL: http://dx.doi.org/10.5539/gjhs.v4n3p148 Abstract Background and Objective: This study aims to look at the pattern and incidence of skin diseases seen in Dermatology/Venereology clinic at the University of Benin Teaching Hospital, Benin City, Edo State, South-South Zone, Nigeria and compare it with other zones of Nigeria. Materials and Methods: This was a prospective study on pattern and incidence of skin diseases in new patients presenting at the Dermatology/ Venereology outpatient clinic of the University of Benin Teaching Hospital, Benin City, Edo State, South-South, Nigeria, from September 2006 to August 2007. All patients were seen by the researchers. Diagnosis were made clinically and sometimes with the support of histopathology. Results: A total number of 4786 patients were seen during the study period and these comprised 2647 HIV/AIDS patients and 2112 pure Dermatological patients. Out of 4786 patients, 755 (15.8%) were new patients. -

4Th Annual Texas Children's Hospital Advanced Practice Provider
A Potpourri of Pediatric Dermatology 4th Annual Texas Children’s Hospital Advanced Practice Provider Conference April 2017 MOISE L. LEVY, M.D. DELL CHILDREN’S MEDICAL CENTER DELL MEDICAL SCHOOL/UT, AUSTIN AUSTIN, TX Conflicts of Interest Ø Anacor Ø Scioderm Ø Castle Creek Pharmaceuticals Ø Up to Date None Should Apply For This Presentation One way we are viewed… It’s just a birthmark 9 month old with asymptomatic scalp lesion noted in NICU; increases in size with straining But maybe something else… Sinus Pericranii Ø Communication between intra- and extracranial venous drainage pathways Ø Most are midline and non.pulsatile Ø Connect pericranial veins with superior sagittal sinus Ø TX depends on flow pattern/direction -Dominant; main flow via SP -Accessory; small flow via SP Neuroradiology 2007;49:505 Neurology 2009;72:e66 Case History 5 y/o girl w celiac disease Seen for evaluation of perianal growth Present, by hx, x 2 yrs No prior tx Case History Was seen by pediatric surgery Excised Condyloma - HPV 6, 16 Management? ARS – Pediatric Anogenital Warts When seeing a 5 yo with anogenital warts A. HPV testing should be done B. All cases are due to abuse C. All cases should be treated with imiquimod D. History and physical examination are key for suspicion of abuse E. Call Dr Eichenfield; he’ll know what to do Pediatric Anogenital Warts Age of onset and abuse - 6.5 ± 3.8 yrs (5.3 yrs) - 37% 2-12 yrs; 70% > 8 yrs - 4 yrs 8 months (83% female) HPV testing felt not of use… high subclinical History and PE key - physical findings abuse rare Arch Dermatol 1990;126:1575 Pediatrics 2005;116:815 Arch Dis Child 2006;91:696 Pediatr Dermatol 2006;23:199 J Pediatr Adolesc Gynecol 2013;26:e121 Age of Onset and Abuse Pediatr Dermatol 2006;23:199 ARS – Pediatric Anogenital Warts When seeing a 5 yo with anogenital warts A. -

The Effectiveness of Topical Scar-Reducing Therapies Administered for Scarring Due to Burns and Other Causes: a Retrospective Pilot Clinical Research
ORIGINAL ARTICLE Aksoy et al. / Gulhane Med J 2018;60: 139-144 139 The effectiveness of topical scar-reducing therapies administered for scarring due to burns and other causes: A retrospective pilot clinical research Hasan Mete Aksoy,1 Berna Aksoy,2 Aslı Tatlıparmak,2 Emel Çalıkoğlu3 (1) Bahçeşehir University, School of Medicine, Plastic and Reconstructive Surgery, Istanbul, Turkey (2) Bahçeşehir University, School of Medicine, Dermatology, Istanbul, Turkey (3) Aksaray University, Faculty of Medicine, Dermatology, Aksaray, Turkey Date submitted: ABSTRACT Oct 019, 2017 Aims: Multiple modalities are used to treat scarring; however, data on the efficacy of Date accepted: Aug 25, 2018 the topical scar-reducing treatments most frequently used by patients is insufficient. Online publication date: This study aimed to retrospectively determine the effectiveness of topical scar-reducing December 15, 2018 treatments and patients’ compliance. Methods: The medical records of patients adimitted for the treatment of scarring were retrospectively evaluated. Patient satisfaction with the treatment was assessed via telephone interviews. Each patient also sent recent photographs of their scars. Pre- and Corresponding Author: post-treatment photographs were scored according to the Manchester Scar Scale, and in Berna Aksoy terms of vascularity and scar surface area (modified MSS ). Bahcesehir University, School of Results: The study included 71 patients with a median scar age of 18 days at the time Medicine, Dermatology, Istanbul, treatment was initiated. Mean duration of follow-up was 41 months. The prescribed Turkey [email protected] treatments included onion extract, silicone gel or sheet, and a pressure garment. The patients reported that the treatments were effective, they were satisfied with the treatments, and the treatments were not excessively difficult to apply. -

Nevus Sebaceous
Nevus Sebaceous A nevus sebaceous (NEE vuhs sih BAY shus) is a type of birthmark that usually appears on the scalp. It may also appear on the face but this is less common. It is made of extra oil glands in the skin. It starts as a flat pink or orange plaque (slightly raised area). Hair does not grow in a nevus sebaceous. Typically, these are fairly small areas of skin. However, they can sometimes be larger and more noticeable. These birthmarks usually look the same until puberty. Hormonal changes cause them to become more raised. During adolescence (teen years) they can become very bumpy and wart-like. This can make them bothersome when brushing, combing or cutting the hair. A nevus sebaceous does not go away on its own. The cause is unknown. As a person gets older, typically after adolescence, abnormal changes to the area can sometimes occur. Your child’s doctor will monitor it over time. Diagnosis Your child’s doctor can usually diagnosis this kind of birthmark. If unsure, the doctor may take a small piece of the birthmark as a biopsy. The doctor will send it to a lab to be looked at under a microscope. This can confirm the diagnosis. Treatment Generally, it is very safe for your child’s doctor to simply watch a nevus sebaceous over time. This is especially true while your child is young (before puberty). A nevus sebaceous will not affect your child’s health, but you or your child may still want it to be taken off. If your child’s nevus sebaceous is large or becomes bothersome, it may be removed. -
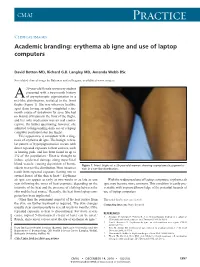
Erythema Ab Igne and Use of Laptop Computers
CMAJ Practice Clinical images Academic branding: erythema ab igne and use of laptop computers David Botten MD, Richard G.B. Langley MD, Amanda Webb BSc See related clinical image by Beleznay and colleagues, available at www.cmaj.ca 20-year-old female university student presented with a two-month history A of asymptomatic pigmentation in a net-like distribution, isolated to the front thighs (Figure 1). She was otherwise healthy, apart from having recently completed a six- month course of isotretinoin for acne. She had no history of trauma to the front of the thighs, and her only medication was an oral contra- ceptive. On further questioning, however, she admitted to longstanding daily use of a laptop computer positioned atop her thighs. This appearance is consistent with a diag- nosis of erythema ab igne. The benign, reticu- lar pattern of hyperpigmentation occurs with direct repeated exposure to heat sources, such as heating pads, and has been found in up to 3% of the population.1 Heat is thought to induce epidermal damage along superficial blood vessels, causing deposition of hemo- Figure 1: Front thighs of a 20-year-old woman showing asymptomatic pigmenta- siderin in a net-like distribution. Most instances tion in a net-like distribution. result from repeated exposure (lasting one to several hours) of the skin to heat.2,3 Erythema ab igne can appear as early as two weeks or as late as one With the widespread use of laptop computers, erythema ab year following the onset of heat exposure, depending on the igne may become more common. -
Assessment of Melanocyte-Specific Primary and Memory Autoimmune Responses in Vitiligo- Prone Smyth and Vitiligo-Susceptible, Non-Expressing Brown Line Chickens
University of Arkansas, Fayetteville ScholarWorks@UARK Theses and Dissertations 8-2018 Assessment of Melanocyte-Specific rP imary and Memory Autoimmune Responses in Vitiligo-Prone Smyth and Vitiligo-Susceptible, Non-Expressing Brown Line Chickens Daniel Morales Falcon University of Arkansas, Fayetteville Follow this and additional works at: https://scholarworks.uark.edu/etd Part of the Cell Biology Commons, and the Immunology of Infectious Disease Commons Recommended Citation Falcon, Daniel Morales, "Assessment of Melanocyte-Specific rP imary and Memory Autoimmune Responses in Vitiligo-Prone Smyth and Vitiligo-Susceptible, Non-Expressing Brown Line Chickens" (2018). Theses and Dissertations. 2912. https://scholarworks.uark.edu/etd/2912 This Dissertation is brought to you for free and open access by ScholarWorks@UARK. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of ScholarWorks@UARK. For more information, please contact [email protected], [email protected]. Assessment of Melanocyte-Specific Primary and Memory Autoimmune Responses in Vitiligo- Prone Smyth and Vitiligo-Susceptible, Non-Expressing Brown Line Chickens A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Cell and Molecular Biology by Daniel Morales Falcon University of California, Riverside Bachelor of Science in Biology, 2003 August 2018 University of Arkansas This dissertation is approved for recommendation to the Graduate Council. ____________________________________ Gisela F. Erf, Ph.D. Dissertation Director ____________________________________ ___________________________________ Yuchun Du, Ph.D. David McNabb, Ph.D. Committee Member Committee Member ____________________________________ Suresh Thallapuranam, Ph.D. Committee Member Abstract Vitiligo is an acquired de-pigmentation disorder characterized by the post-natal loss of epidermal melanocytes (pigment-producing cells) resulting in the appearance of white patches in the skin. -

Review Cutaneous Patterns Are Often the Only Clue to a a R T I C L E Complex Underlying Vascular Pathology
pp11 - 46 ABstract Review Cutaneous patterns are often the only clue to a A R T I C L E complex underlying vascular pathology. Reticulate pattern is probably one of the most important DERMATOLOGICAL dermatological signs of venous or arterial pathology involving the cutaneous microvasculature and its MANIFESTATIONS OF VENOUS presence may be the only sign of an important underlying pathology. Vascular malformations such DISEASE. PART II: Reticulate as cutis marmorata congenita telangiectasia, benign forms of livedo reticularis, and sinister conditions eruptions such as Sneddon’s syndrome can all present with a reticulate eruption. The literature dealing with this KUROSH PARSI MBBS, MSc (Med), FACP, FACD subject is confusing and full of inaccuracies. Terms Departments of Dermatology, St. Vincent’s Hospital & such as livedo reticularis, livedo racemosa, cutis Sydney Children’s Hospital, Sydney, Australia marmorata and retiform purpura have all been used to describe the same or entirely different conditions. To our knowledge, there are no published systematic reviews of reticulate eruptions in the medical Introduction literature. he reticulate pattern is probably one of the most This article is the second in a series of papers important dermatological signs that signifies the describing the dermatological manifestations of involvement of the underlying vascular networks venous disease. Given the wide scope of phlebology T and its overlap with many other specialties, this review and the cutaneous vasculature. It is seen in benign forms was divided into multiple instalments. We dedicated of livedo reticularis and in more sinister conditions such this instalment to demystifying the reticulate as Sneddon’s syndrome. There is considerable confusion pattern.