Introduction to Pathology Pathology:พยาธิวิทยา
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Università Degli Studi Di Milano
UNIVERSITÀ DEGLI STUDI DI MILANO SCUOLA DI DOTTORATO IN MEDICINA MOLECOLARE CICLO XXVIII Anno Accademico 2014/2015 TESI DI DOTTORATO DI RICERCA MED09 STUDIES OF HEME-REGULATED eIF2α KINASE STRESS SIGNALING ON MATURATION OF MACROPHAGES AND ERYTHROBLASTIC ISLAND FORMATION IN IRON RESTRICTIVE ERYTHROPOIESIS Dottorando : Elena PALTRINIERI Matricola N° R10203 TUTORE : Chiar.ma Prof.ssa Maria Domenica CAPPELLINI CO-TUTORE: Prof.ssa Jane-Jane CHEN DIRETTORE DEL DOTTORATO: Chiar.mo Prof. Mario CLERICI ABSTRACT Iron is the most important metal for the human body. Different states of iron deficiency have long existed and remain very common in today’s population. The vast majority of cases of iron deficiency are acquired as a result from blood loss. Any condition in which dietary iron intake does not meet the body’s demands will result in iron deficiency. Iron and heme are both fundamental in hemoglobin synthesis and erythroid cell differentiation. In addition to act as a prosthetic group for hemoglobin, heme regulates the transcription of globin genes and controls the translational activity in erythroid precursors through modulation of the kinase activity of the eIF2α kinase HRI which is regulated by heme. HRI, the heme-regulated inhibitor of translation, was first discovered in reticulocytes under the conditions of iron and heme deficiencies. During heme deficiency conditions, in the erythroid precursors protein synthesis is inhibited by phosphorylation of the α-subunit of the eukaryotic initiation factor 2 (eIF2α) as the result of the activation of HRI. The role of HRI is to control that the amount of globin chains synthesized are not in excess of what can be utilized for hemoglobin tetramers depending of heme available. -

General Pathology
Jordan University of Science and Technology Faculty of Medicine 2018-2019 COURSE TITLE : GENERAL PATHOLOGY. COURSE CODE : MED 231. CREDIT HOURS : 3 CREDIT HOURS SEQUENCE : YEAR 2, FIRST SEMESTER COURSE COORDINATOR: Dr. Alia AlMuhtaseb; Dr. Mohammad Orjani CONTACT: [email protected]; [email protected] Course Description: This course deals with the investigation of those pathological mechanisms common to all tissue-cell pathology. Attention is paid to the processes of cellular adaptation, inflammation, repair, immunology, cellular accumulation, and neoplasia. Lecture will attempt first to familiarize the student with our basic layers of defense. Next those vocabulary terms and concepts relevant to the disease process will be introduced. The terminology employed is both medical and chiropractic. Processes and concepts will be developed with the aid of Data show. An interactive format is employed in which the instructor poses questions to enable the student to self-test their knowledge prior to exams and develop skills in communicating these basic pathological concepts to others. During the course and whenever relevant the students are exposed to clinical problems to emphasize the explanations of symptoms, signs, investigations and forms of treatments. Practical sessions are planned to give students the opportunity to expose their knowledge for discussion and confirm concepts learned in lectures. Small group discussions of clinical cases are planned at the end of the course were students are divided into small groups and with the help of an instructor they analyze and discuss the problem. The course will be given through 28 lectures, 7 practical (laboratory) sessions, and one small group discussion activity over 15 weeks and for one whole semester. -

1 Pathology Week 1 – Cellular Adaptation, Injury and Death
Pathology week 1 – Cellular adaptation, injury and death Cellular responses to injury Cellular Responses to Injury Nature and Severity of Injurious Stimulus Cellular Response Altered physiologic stimuli: Cellular adaptations: • ↑demand, ↑ trophic stimulation (e.g. growth factors, hormones) • Hyperplasia, hypertrophy • ↓ nutrients, stimulation • Atrophy • Chronic irritation (chemical or physical) • Metaplasia Reduced oxygen supply; chemical injury; microbial infection Cell injury: • Acute and self-limited • Acute reversible injury • Progessive and severe (including DNA damage) • Irreversible injury → cell death Necrosis Apoptosis • Mild chronic injury • Subcellular alterations in organelles Metabolic alterations, genetic or acquired Intracell accumulations; calcifications Prolonged life span with cumulative sublethal injury Cellular aging Hyperplasia - response to increased demand and external stimulation - ↑ number cells - ↑ volume of organ - often occurs with hypertrophy - occurs if cells able to synthesize DNA – mitotic division - physiologic or pathologic Physiological hyperplasia A) hormonal – ↑ functional capacity tissue when needed (breast in puberty, uterus in pregnancy) B) compensatory - ↑ tissue mass after damage/resection (post-nephrectomy) Mechanisms: - ↑ local production growth factors or activation intracellular signaling pathways o both → production transcription factors that turn on cellular genes incl those encoding growth factors, receptors for GFs, cell cycle regulators →→ cellular proli feration - in hormonal hyperplasia -
Cellular Adaptation
Cellular Adaptation Dr. Adeboye OO (MBBS, Cert. LMIH, FMCPath) Dept of Anatomic Pathology Bowen University Cellular adaptation • Cell death is not the only consequence of cellular injury or stress • Cells can respond to excessive physiologic or pathologic stimuli by undergoing both functional and morphologic change in which a new steady state is achieved that preserves the viability of the cell(Adaptation) . • The adaptive response include- • Adaptation of growth and differentiation • Intracellular accumulation • Pathologic calcification • Hyaline change • Cellular aging Adaptation of growth and differentiation • Adaptations are reversible changes in the size, number,phenotype, metabolic activity, or functions of cells in response to changes in their environment. Such adaptations may take several distinct forms : • 1. hyperplasia • 2. hypertrophy • 3. atrophy • 4. metaplasia hypertrophy • Increase in the size of cells that result in the increase in size of the affected organ. • No new cells just larger cells • May coexist with hyperplasia in cells capable of division( eg epithelial, hematopoesis etc), in non dividing cells (eg the nerve ,cardiac and skeletal muscle) increase tissue mass is due to hypertrophy • Can be physiologic or pathologic Physiologic hypertrophy • Caused by- (a) increased functional demand eg hypertrophy of striated muscle in muscle builder.(b) stimulation by hormones or growth factors eg physiologic hypertrophy of the uterus during pregnancy Hypertrophy of uterus during pregnancy Micrograph showing smooth muscle -

Clinical Pathology, Immunopathology and Advanced Vaccine Technology in Bovine Theileriosis: a Review
pathogens Review Clinical Pathology, Immunopathology and Advanced Vaccine Technology in Bovine Theileriosis: A Review Onyinyechukwu Ada Agina 1,2,* , Mohd Rosly Shaari 3, Nur Mahiza Md Isa 1, Mokrish Ajat 4, Mohd Zamri-Saad 5 and Hazilawati Hamzah 1,* 1 Department of Veterinary Pathology and Microbiology, Faculty of Veterinary Medicine, Universiti Putra Malaysia, Serdang 43400, Malaysia; [email protected] 2 Department of Veterinary Pathology and Microbiology, Faculty of Veterinary Medicine, University of Nigeria Nsukka, Nsukka 410001, Nigeria 3 Animal Science Research Centre, Malaysian Agricultural Research and Development Institute, Headquarters, Serdang 43400, Malaysia; [email protected] 4 Department of Veterinary Pre-clinical sciences, Faculty of Veterinary Medicine, Universiti Putra Malaysia, Serdang 43400, Malaysia; [email protected] 5 Research Centre for Ruminant Diseases, Faculty of Veterinary Medicine, Universiti Putra Malaysia, Serdang 43400, Malaysia; [email protected] * Correspondence: [email protected] (O.A.A.); [email protected] (H.H.); Tel.: +60-11-352-01215 (O.A.A.); +60-19-284-6897 (H.H.) Received: 2 May 2020; Accepted: 16 July 2020; Published: 25 August 2020 Abstract: Theileriosis is a blood piroplasmic disease that adversely affects the livestock industry, especially in tropical and sub-tropical countries. It is caused by haemoprotozoan of the Theileria genus, transmitted by hard ticks and which possesses a complex life cycle. The clinical course of the disease ranges from benign to lethal, but subclinical infections can occur depending on the infecting Theileria species. The main clinical and clinicopathological manifestations of acute disease include fever, lymphadenopathy, anorexia and severe loss of condition, conjunctivitis, and pale mucous membranes that are associated with Theileria-induced immune-mediated haemolytic anaemia and/or non-regenerative anaemia. -

Tissue Engineering Strategies to Improve Tendon Healing and Insertion Site Integration
Tissue Engineering Strategies to Improve Tendon Healing and Insertion Site Integration A dissertation submitted to the Division of Research and Advanced Studies of the University of Cincinnati in partial fulfillment of the of the requirements for the degree of DOCTOR OF PHILOSOPHY (Ph.D.) in the Department of Biomedical Engineering of the College of Engineering and Applied Science 2011 by Kirsten Rose Carol Kinneberg B.S., University of Minnesota, Twin Cities, MN, 2006 Committee Chair: Jason T. Shearn Abstract Tendon and ligament tears and ruptures remain common and significant musculoskeletal injuries. Repairing these injuries continues to be a prominent challenge in orthopaedics and sports medicine. Despite advances in surgical techniques and procedures, traditional repair techniques maintain a high incidence of re-rupture. This has led some researchers to consider using tissue engineered constructs (TECs). Previous studies in our laboratory have demonstrated that TEC stiffness at the time of surgery is positively correlated with repair tissue stiffness 12 weeks post-surgery. This correlation provided the rationale for implanting a soft tissue patellar tendon autograft (PTA) to repair a central-third defect in the rabbit patellar tendon (PT). The PTA was significantly stiffer than previous TECs and matched the stiffness of the normal central-third PT. Accordingly, we expected a significant improvement in repair tissue biomechanics relative to both natural healing (NH) and TEC repair. At 12 weeks, treatment with PTA improved repair tissue stiffness relative to NH. However, PTA and NH tissues did not differ in maximum force, modulus or maximum stress. Additionally, neither repair group regenerated normal zonal insertion sites. -

Seventh Congress of the International Bioiron Society (IBIS)
Seventh Congress of the International BioIron Society (IBIS) Biennial World Meeting (BioIron 2017) May 7 – 11, 2017 UCLA Meyer & Renee Luskin Conference Center | Los Angeles, USA Featuring Special Events: Introductory Course – May 7, 2017 “Essentials of BioIron for Clinicians and Scientists” “Meet the Expert” Sessions for Trainees May 10 – 11, 2017 INTERNATIONAL BIOIRON SOCIETY PROGRAM BOOK Acknowledgments IBIS This conference has received support from the NIH NCATS UCLA CTSI Grant Number UL1TR0001881. This conference has received support from the NIH/NIDDK R-13 Grant. This conference has received support from the NIXHNHLBI-R-13 Grant. Seventh Congress of the International BioIron Society Page 2 Table of Contents IBIS Seventh Congress of the Internationl BioIron Society (IBIS) Biennial World Meeting (BioIron 2017) May 7 - 11, 2017 UCLA Meyer & Renee Luskin Conference Center | Los Angeles, USA Welcome Message ..............................................................................................................................Page 4 Board of Directors ................................................................................................................................Page 5 General Meeting Information ...............................................................................................................Page 6 Special Events .....................................................................................................................................Page 8 Local Activities .....................................................................................................................................Page -
General User Charges in AIIMS Raipur
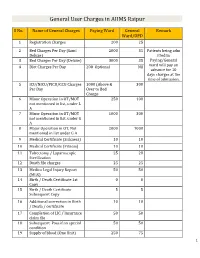
General User Charges in AIIMS Raipur S No. Name of General Charges Paying Ward General Remark Ward/OPD 1 Registration Charges 200 25 2 Bed Charges Per Day (Sami 2000 35 Patients being adm Deluxe) itted in 3 Bed Charges Per Day (Deluxe) 3000 35 Paying/General 4 Diet Charges Per Day 200 Optional Nil ward will pay an advance for 10 days charges at the time of admission. 5 ICU/NICU/PICU/CCU Charges 1000 (Above & 300 Per Day Over to Bed Charge 6 Minor Operation in OT/MOT 250 100 not mentioned in list, under L A 7 Minor Operation in OT/MOT 1000 300 not mentioned in list, under G A 8 Major Operation in OT, Not 2000 1000 mentioned in list under G A 9 Medical Certificate (Sickness) 10 10 10 Medical Certificate (Fitness) 10 10 11 Tubectomy / Laparoscopic 25 20 Sterilization 12 Death file charges 25 25 13 Medico Legal Injury Report 50 50 (MLR) 14 Birth / Death Certificate 1st 0 0 Copy 15 Birth / Death Certificate 5 5 Subsequent Copy 16 Additional correction in Birth 10 10 / Death / certificate 17 Completion of LIC / Insurance 50 50 claim file 18 Subsequent Pass if on special 50 50 condition 19 Supply of blood (One Unit) 250 75 1 20 Medical Board Certificate 500 500 On Special Case User Charges for Investigations in AIIMS Raipur S No. Name of Investigations Paying General Remark Ward Ward/OPD Anaesthsia 1 ABG 75 50 2 ABG ALONGWITH 150 100 ELECTROLYTES(NA+,K+)(Na,K) 3 ONLY ELECTROLYTES(Na+,K+,Cl,Ca+) 75 50 4 ONLY CALCIUM 50 25 5 GLUCOSE 25 20 6 LACTATE 25 20 7 UREA. -

Practice Parameter for the Diagnosis and Management of Primary Immunodeficiency
Practice parameter Practice parameter for the diagnosis and management of primary immunodeficiency Francisco A. Bonilla, MD, PhD, David A. Khan, MD, Zuhair K. Ballas, MD, Javier Chinen, MD, PhD, Michael M. Frank, MD, Joyce T. Hsu, MD, Michael Keller, MD, Lisa J. Kobrynski, MD, Hirsh D. Komarow, MD, Bruce Mazer, MD, Robert P. Nelson, Jr, MD, Jordan S. Orange, MD, PhD, John M. Routes, MD, William T. Shearer, MD, PhD, Ricardo U. Sorensen, MD, James W. Verbsky, MD, PhD, David I. Bernstein, MD, Joann Blessing-Moore, MD, David Lang, MD, Richard A. Nicklas, MD, John Oppenheimer, MD, Jay M. Portnoy, MD, Christopher R. Randolph, MD, Diane Schuller, MD, Sheldon L. Spector, MD, Stephen Tilles, MD, Dana Wallace, MD Chief Editor: Francisco A. Bonilla, MD, PhD Co-Editor: David A. Khan, MD Members of the Joint Task Force on Practice Parameters: David I. Bernstein, MD, Joann Blessing-Moore, MD, David Khan, MD, David Lang, MD, Richard A. Nicklas, MD, John Oppenheimer, MD, Jay M. Portnoy, MD, Christopher R. Randolph, MD, Diane Schuller, MD, Sheldon L. Spector, MD, Stephen Tilles, MD, Dana Wallace, MD Primary Immunodeficiency Workgroup: Chairman: Francisco A. Bonilla, MD, PhD Members: Zuhair K. Ballas, MD, Javier Chinen, MD, PhD, Michael M. Frank, MD, Joyce T. Hsu, MD, Michael Keller, MD, Lisa J. Kobrynski, MD, Hirsh D. Komarow, MD, Bruce Mazer, MD, Robert P. Nelson, Jr, MD, Jordan S. Orange, MD, PhD, John M. Routes, MD, William T. Shearer, MD, PhD, Ricardo U. Sorensen, MD, James W. Verbsky, MD, PhD GlaxoSmithKline, Merck, and Aerocrine; has received payment for lectures from Genentech/ These parameters were developed by the Joint Task Force on Practice Parameters, representing Novartis, GlaxoSmithKline, and Merck; and has received research support from Genentech/ the American Academy of Allergy, Asthma & Immunology; the American College of Novartis and Merck. -

Microbiology and Immunology
College of Medicine MI Microbiology and Immunology MI 494G IMMUNOBIOLOGY. (3) A survey of theories and mechanisms of immunity, including: nature of antigens and antibodies, antigen-antibody reactions, immunocompetent cells, immunogenetics, allergic reactions, tumor immunology and transplantation immunology. Prereq: BCH 401G (may be taken concurrently) and BIO 208 or BIO 308 or consent of instructor. (Same as BIO 494G.) MI 590 CELLULAR AND MOLECULAR PHYSIOLOGY. (4) This course will focus on the cellular and molecular physiology of inter-and intracellular communication. In particular, it will provide an overview of established and emerging intracellular signaling mechanisms which utilize i) cyclic nucleotides (cAMP; cGMP), ii) calcium (phosphatidylinositol metabolism: cyclic ADP-ribose), iii) transmembrane ion fluxes (voltage- and receptor-operated channels), iv) tyrosine kinases, and v) nuclear transcription factors. The material will be presented in a number of formats including didactic lecture and group discussions of selected readings. Prereq: PGY 412G, PGY 502 or consent of instructor. (Same as PGY 590.) MI 595 IMMUNOBIOLOGY LABORATORY. (2) Laboratory in immunology and serology. Preparation, standardization, and uses of biological products; serology. Laboratory; four hours. Prereq: BIO/MI 494G or concurrently; or consent of instructor. (Same as BIO 595.) MI 598 CLINICAL MICROBIOLOGY. (3) An introduction to the concepts of clinical microbiology through a survey of the microbial diseases of man using an organ system approach. Prereq: BIO 208 and 209, BIO 476G recommended, CHE 230 or 236, or consent of instructor. (Same as PAT 598.) MI 601 SPECIAL TOPICS IN MOLECULAR AND CELLULAR GENETICS. (1) Each semester five distinguished scientists visit the UK campus to deliver a series of three formal lectures each and participate in numerous informal contacts with graduate students. -

Cellular Adaptation
ALTERATIONS IN CELLULAR AND TISSUE FUNCTION Lois E. Brenneman, MSN, APN, CELLULAR ADAPTATION Atrophy - decrease or shrinkage in cell size - Can (if sufficient numbers) result in shrinkage of entire organ Example: muscular atrophy after cast is removed Example: sports steroid abuse causes atrophy of penis - Physiologic atrophy - normal process Example: atrophy of thymus during childhood - Pathologic atrophy - disease process Example: Addison’s disease -> atrophy adrenal glands - Disuse Atrophy Example: Prolonged bed rest causes muscle atrophy Example: Casting limb causes atrophy Atrophic cells have fewer mitochondria and myofilaments Autophagic vacuoles occurs with malnutrition Lipofuscin - yellow-brown age pigment (may resist destruction) - Persists as membrane-bound residue bodies - Accumulates w age: liver, myocardial and atrophic cells - Results in “age spots” to skin “Age spots” Lipofuscin accumulation to skin © 2004 Lois E. Brenneman, MSN, CS, ANP, FNP all rights reserved - www.npceu.com 1 Hypertrophy - increase in cell size (vs cell number with hyperplasia) Results in increased size of organ Cardiac and kidney esp prone to hypertrophy Increased size -> increased cellular protein and not increased fluid Physiologic hypertrophy - normal process Example: muscle increase with exercise Example: genital size increase with hormones of puberty Pathologic hypertrophy - disease process Example - Left ventricular hypertrophy from hypertension -> congestive heart failure Triggers for hypertrophy Mechanical: stretch, exercise Trophic: growth factors, hormones, vasoactive agents CELLULAR HYPERTROPY Left: dependent edema in CHF Right: dilated cardiomyopathy Left ventricular hypertrophy (bottom) vs normal (top) © 2004 Lois E. Brenneman, MSN, CS, ANP, FNP all rights reserved - www.npceu.com 2 Hyperplasia - increase in number of cells (increased rate of cell division) - Can occur in response to injury esp with cell death - Can occur together with hypertrophy note: if organ with non-dividing cells (e.g. -

Chapter 1 Cellular Reaction to Injury 3
Schneider_CH01-001-016.qxd 5/1/08 10:52 AM Page 1 chapter Cellular Reaction 1 to Injury I. ADAPTATION TO ENVIRONMENTAL STRESS A. Hypertrophy 1. Hypertrophy is an increase in the size of an organ or tissue due to an increase in the size of cells. 2. Other characteristics include an increase in protein synthesis and an increase in the size or number of intracellular organelles. 3. A cellular adaptation to increased workload results in hypertrophy, as exemplified by the increase in skeletal muscle mass associated with exercise and the enlargement of the left ventricle in hypertensive heart disease. B. Hyperplasia 1. Hyperplasia is an increase in the size of an organ or tissue caused by an increase in the number of cells. 2. It is exemplified by glandular proliferation in the breast during pregnancy. 3. In some cases, hyperplasia occurs together with hypertrophy. During pregnancy, uterine enlargement is caused by both hypertrophy and hyperplasia of the smooth muscle cells in the uterus. C. Aplasia 1. Aplasia is a failure of cell production. 2. During fetal development, aplasia results in agenesis, or absence of an organ due to failure of production. 3. Later in life, it can be caused by permanent loss of precursor cells in proliferative tissues, such as the bone marrow. D. Hypoplasia 1. Hypoplasia is a decrease in cell production that is less extreme than in aplasia. 2. It is seen in the partial lack of growth and maturation of gonadal structures in Turner syndrome and Klinefelter syndrome. E. Atrophy 1. Atrophy is a decrease in the size of an organ or tissue and results from a decrease in the mass of preexisting cells (Figure 1-1).